
Abstract
Study Design
Case series of two arytenoid dislocations after anterior cervical discectomy.
Objective
To recognize arytenoid dislocation as a possible cause of prolonged hoarseness in patients after anterior cervical discectomies.
Summary of Background Data
Prolonged hoarseness is a common postoperative complication after anterior cervical spine surgery. The etiology of prolonged postoperative hoarseness is usually related to a paresis of the recurrent laryngeal nerve. However, other causes of postoperative hoarseness may be overlooked in this clinical scenario. Other possible etiologies include pharyngeal and laryngeal trauma, hematoma and edema, injury of the superior laryngeal nerve, as well as arytenoid cartilage dislocation. Arytenoid dislocation is often misdiagnosed as vocal fold paresis due to recurrent or laryngeal nerve injury.
Methods
We report two cases of arytenoid dislocation and review the literature on this pathology.
Results
Two patients treated with anterior cervical discectomy and fusion experienced prolonged postoperative hoarseness. Arytenoid dislocation was confirmed by flexible fiber-optic laryngoscopy in both cases. The dislocations experienced spontaneous reduction at 6 weeks and 3 months postsurgery.
Conclusions
Arytenoid dislocation must be considered in the differential diagnosis of prolonged postoperative hoarseness and evaluated for using direct laryngoscopy, computed tomography, or a laryngeal electromyography. Upon diagnosis, treatment must be considered immediately. Slight dislocations can reduce spontaneously without surgical intervention; however, operative intervention may be required at times.
Hoarseness is a common postoperative complication, reported in ∼50% of cases requiring intubation. 1 In 1.6% of such cases, this hoarseness will not resolve after the first week and may continue indefinitely. 1 The etiology of prolonged postoperative hoarseness is often difficult to establish; it can be caused by pharyngeal and laryngeal trauma, hematoma and edema, injury to the recurrent or superior laryngeal nerves, as well as arytenoid cartilage dislocation. 2 , 3 , 4 Postoperative hoarseness due to arytenoid dislocation is often misdiagnosed as recurrent laryngeal nerve (RLN) palsy. Arytenoid dislocations are reported in nearly 0.1% of all surgeries requiring intubation and must be carefully considered during a postoperative evaluation. Arytenoid dislocation can be caused by intubation, external blunt trauma, laryngoscopy, as well as any acute trauma to the cricoarytenoid joint. 5 Intubation is the most common etiology. Arytenoid dislocation results in a hypomobile vocal cord complex, which can be readily observed via strobovideolaryngoscopy, laryngeal electromyography (EMG), or computed tomography (CT). Treatment commonly includes closed reduction and chemical splinting, and spontaneous reduction can also occur. 3 , 5 We present two cases of arytenoid dislocation after anterior cervical discectomy and fusion (ACDF). This complication has not yet been reported in anterior cervical discectomy cases.
Case Reports
Case 1
A 39-year-old woman diagnosed with C5–6, C6–7 posterolateral disk herniations causing cervical myeloradiculopathy underwent an ACDF with allograft and instrumentation. The patient had an uneventful intubation. A standard Smith-Robinson approach was taken to the cervical spine. The exposure was done by an ear, nose, and throat (ENT) surgeon. Central and bilateral decompressions were performed, and a graft was applied at both levels. An anterior cervical plate spanning C5–7 was then applied. The RLN was not visualized during the procedure. The operative time was under 90 minutes; as standard clinical practice, the transverse retraction was let down every 20 to 30 minutes, and the endotracheal tube cuff was inflated to the just sealed pressure and let down and reinflated after each level. The patient was shown to be moving all four extremities. On postoperative day 1 the patient experienced difficulty clearing her throat, and mild intermittent hoarseness. The hoarseness progressed and became moderate and persistent in nature. The ENT surgeon followed the patient from postoperative day 1 due to the surgeon's involvement in the exposure. The ENT team suggested a laryngoscopy. A flexible fiber-optic laryngoscopy performed 3 weeks after the procedure revealed a hypomobile vocal cord complex as a result of an arytenoid dislocation (Fig. 1). The dislocation reduced spontaneously 8 weeks following surgery, with hoarseness and difficulty clearing throat completely resolved.
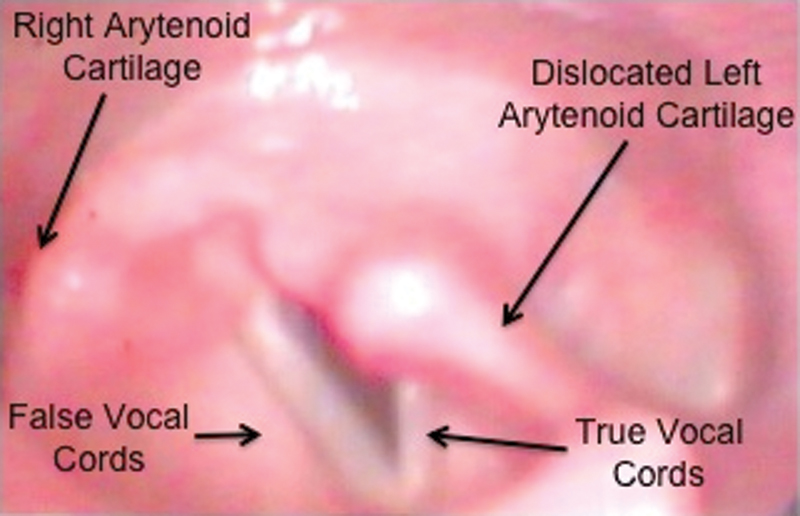
Flexible fiber-optic laryngoscopy showing a hypomobile vocal cord complex due to arytenoid dislocation.
Case 2
A 39-year-old man presenting with cervical radiculopathy underwent a C6–7 ACDF with anterior cervical plate and allograft, similar to the previous case. The patient was under general anesthesia. The intubation was uneventful. The only complaint postoperatively was hoarseness, which presented immediately. Hoarseness persisted postoperatively until the time of discharge and an outpatient ENT consult was obtained. Postoperative laryngoscopy confirmed the diagnosis of arytenoid dislocation. The dislocation spontaneously reduced at ∼6 weeks. The patient noted that the hoarseness normalized when he put on his tie for the first time after the procedure. No recurrence of hoarseness has been observed since.
Discussion
Arytenoid dislocation is a possible cause of prolonged postoperative hoarseness. Although this is not a common complication, occurring in only 0.1% of cases requiring intubation, it must be considered as a possible postoperative complication. 1 Arytenoid dislocation is especially relevant as a cause of postoperative hoarseness after procedures involving manipulation of the laryngeal region. The anatomy of the larynx predisposes the arytenoid cartilage to perioperative injury (Figs. 2, 3). An arytenoid dislocation can be caused by intubation, retraction, or perioperative trauma to the cricoarytenoid joint. However, it is often not considered as a diagnostic possibility after routine anterior cervical spine surgery as it is not nearly as frequently reported as RLN palsies.
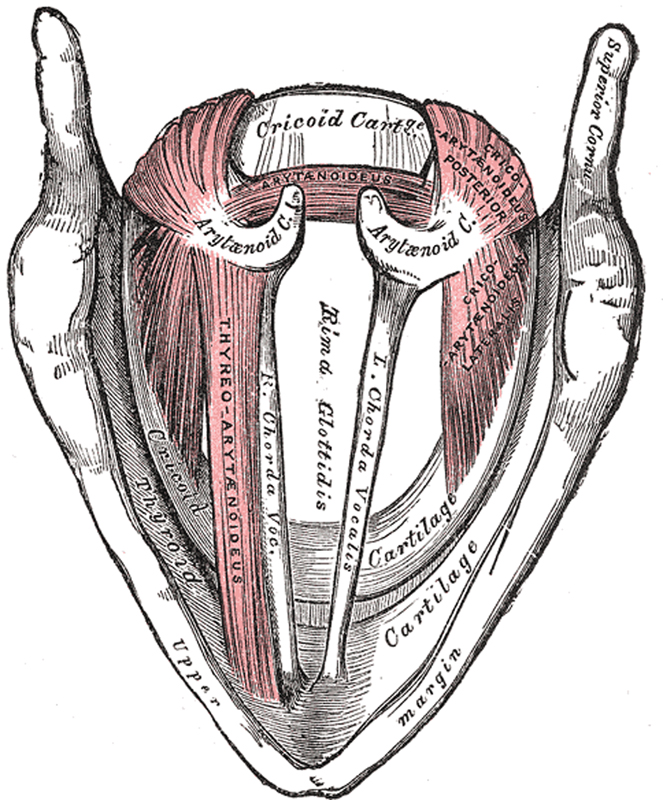
Illustration of the muscles and cartilages of the larynx (superior view).
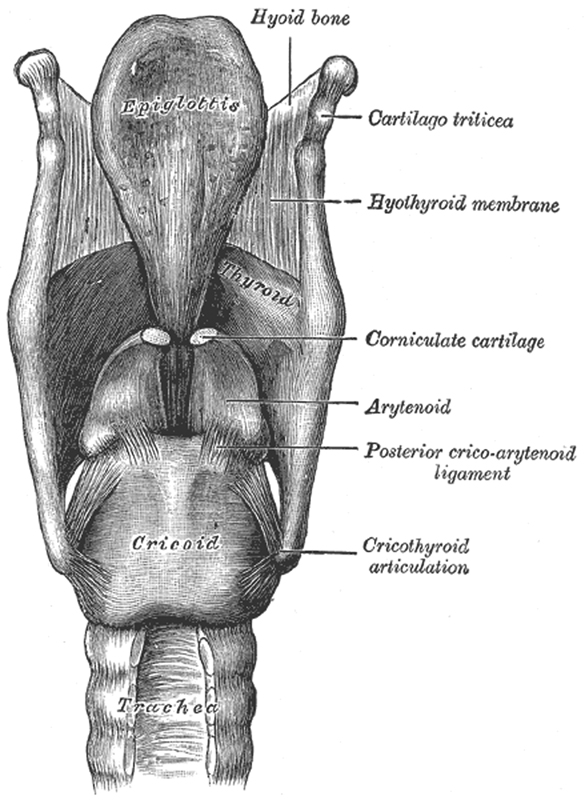
Illustration of the cartilages of the larynx (posterior view).
An arytenoid dislocation has minimal life-threatening effects but has a significant negative impact on quality of life. The most common symptom of dislocation is prolonged hoarseness due to hypomobility of the vocal cords. Early diagnosis and treatment are pivotal for return of optimal voice quality. Late diagnosis worsens prognosis, thus it is important to maintain suspicion of arytenoid dislocation in cases of postoperative prolonged hoarsenss. 5 It is often difficult to differentiate between an arytenoid dislocation and vocal cord paralysis/paresis due to their similar presentation.
Injury to the RLNs or the superior laryngeal nerves (SLNs) can result in vocal cord paralysis or paresis. The position of the right and left RLNs within the tracheoesophageal groove makes them especially susceptible to iatrogenic injury.6 The most common mechanism of injury to the RLN during anterior cervical spine surgery is neuropraxia due to compression of the RLN against the endotracheal tube. 7 , 8 The occurrence of RLN injury after anterior cervical spine surgery has been reported as between 2% and 21.6% 9 , 10 . Injury to the SLN nerve results in hypomobility of the cricothyroid muscle and a hoarse/breathy voice. RLN and SLN injuries are symptomatically similar to arytenoid dislocation. Arytenoid dislocation is often misdiagnosed as vocal fold paralysis/paresis resultant from RLN/SLN injury. A laryngoscopy, video fluorography, computed tomography, and EMG can be useful tools to distinguish the two. 11
Laryngoscopy and stroboscopy in patients with suspected arytenoid joint injury may display either an anteromedial or posterolateral arytenoid position with reduced vocal fold motion. Discriminating between arytenoid dislocation and vocal cord paralysis secondary to nerve injury can be difficult based on laryngoscopy alone. The absence of a jostle sign is one indicator consistent with arytenoid dislocation. The jostle sign describes passive medial movement of the affected vocal cord during adduction due to absence of lateral tension from the denervated musculature. CT scans may be useful in showing malpositioning of the affected joint including displacement of the arytenoid body or altered angulation of the aryepiglottic fold. EMG studies are useful for distinguishing arytenoid dislocation from vocal cord paralysis. In the case of arytenoid dislocation, a normal recruitment pattern on EMG will be expected, as opposed to an absence of electrical activity in the damaged nerve with RLN or SLN injury. Even upon the diagnosis of arytenoid dislocation, its etiology may be difficult to deduce.
The most common cause of arytenoid dislocation is intubation trauma, reported as being responsible for between 80 and 87% of arytenoid dislocations. 4 , 5 However, insertion of any instruments, such as a transesophageal endocardiography probe, into the upper aerodigestive tract predisposes the patient to possible arytenoid injury. 12 Several theories have been postulated regarding the mechanism of dislocation associated with intubation. Posterior lateral dislocation of the left arytenoid can result from direct pressure from the endotracheal tube. 13 The endotracheal tube is most often held in the right hand and the endoscope in the left; this conformation allows the distal end of the endotracheal tube to apply direct pressure on the left arytenoid cartilage in the posterolateral direction. Another possible mechanism is a posterosuperior dislocation of the arytenoid cartilage during extubation if the cuff of the endotracheal tube is not fully deflated. 14 Anterior dislocations by the blade of the laryngoscope or by the endotracheal tube tip while the anesthesiologist searches for the glottal opening are also possible. 15
Several treatment options exist for arytenoid dislocations. Voice therapy is recommended for all patients. Closed reduction under local anesthesia with slight sedation is typically the first treatment approach. After successful closed reduction, joint stability is assessed. If closed reduction is unsuccessful and proper repositioning is not achieved, then medialization procedures are considered to attain proper glottic closure; medialization of posterior dislocations can be achieved by injecting fat lateral to the thyroarytenoid muscle or injecting Botox (Allergan, Irvine, CA) into the posterior cricoarytenoid muscle. Anterior dislocations have been treated via Botox injection into the thyroarytenoid muscle. 4 , 5 Steroid injections can help reduce inflammation and healing postsurgery. Open reductions are considered if the closed reduction approach, with or without medialization, is unsuccessful and recurrent dislocations are observed. Prompt treatment is essential to attain full recovery. 13 , 14 , 16 , 17 Sataloff et al found that the average time between injury and surgical reduction was 10 weeks for patients who experienced full vocal recovery, compared with 29 weeks for patients who had residual voice alteration. 5 Delaying treatment may lead to fibrosis of the injured joint prohibiting later reduction. 18 For this reason, it is pivotal to obtain an ENT consultation early, with the goal of intervention within 10 weeks.
In both of our cases, the diagnosis was confirmed via a flexible fiber-optic laryngoscopy. Paralysis of the vocal cords due to injury of the RLN is unlikely because the nerve was noted to be intact at the end of the procedure. The etiology of the dislocation is difficult to ascertain. Statistically, the most likely cause is intubation. Other possible causes include perioperative trauma during the Smith Robinson anterior approach to the cervical spine, traction-related injury, or injury during instrumentation of the cervical spine.
ACDF is a common procedure, with over 500,000 performed annually in the United States with excellent clinical results. 19 Dysphagia is noted in 9.5% of ACDF cases; however, the great majority of the cases resolve within 48 hours. If prolonged hoarseness occurs, we recommend that arytenoid dislocation be considered in the differential diagnosis and evaluated for using laryngoscopy, CT, or a laryngeal EMG. Upon diagnosis, treatment must be considered immediately. Slight dislocations can reduce spontaneously without surgical intervention; however, delaying treatment may lead to fibrosis of the injured joint prohibiting later reduction.
In summary, we present two cases of arytenoid dislocation associated with ACDF. This is the first time an arytenoid dislocation has been reported in association with an ACDF procedure. The dislocations were confirmed via flexible fiber-optic laryngoscopy. Both cases reduced spontaneously.
Disclosures
Vadim Goz, None
Sheeraz Qureshi, Consulting: Stryker Spine, Medtronic, Zimmer Spine, Orthofix Spine; Royalties: Zimmer Spine; Speakers’ Bureau: Stryker Spine, Medtronic, Zimmer Spine
Andrew C. Hecht, None