
Abstract
We set out to define the prevalence, clinical features and severity of chronic headache among the affiliates of two groups of general practitioners (GPs) and to illustrate the diagnostic and therapeutic modalities employed. A semistructured questionnaire was completed for 2291 children and adults, seen at office or home consultations over a 6-month period by 44 GPs in two areas of Northern Italy (Varese and Sondrio) and Southern Italy (San Giovanni Rotondo), to assess the presence and the clinical features of chronic headache, the severity of the disease (i.e. the degree of interference with work and daily living activities), the diagnostic work-up, and the main treatment modalities. GPs attempted the classification of headache according to the International Headache Society (IHS) criteria. The sample comprised 910 men and 1381 women aged 2-92 years; 39% of cases reported chronic headache (Varese/Sondrio 40%; San Giovanni Rotondo 38%; men 28%; women 47%). Headache was mostly present for >10 years, with one to three attacks/month lasting 4-24 h. Headache was mild in 18% of cases, moderate in 29%, severe in 24%, and very severe in 29%. Diagnostic assessment and treatment varied in the study areas. Diagnostic work-up, hospital admissions, referral to headache centres, and treatment modalities tended to be correlated with headache severity. The GPs could not classify headache using the IHS categories in 27% of cases (Varese/Sondrio 11%; San Giovanni Rotondo 78%). An inverse correlation was found between case classification and use of subsidiary diagnostic and therapeutic aids. Chronic headache is common among individuals seen in general practice. The patterns of health care use tend to be correlated to its severity. A better knowledge of the IHS criteria may be directly related to lower management costs.
Introduction
Migraine and other headaches are frequently chronic disorders involving repeated attacks sometimes leading to poor performance at school, impairment of work and leisure activities, and reduction of the quality of life. However, the burden of chronic headache as a disabling condition and a source of health care use is still ill-defined. Better knowledge of this burden could help map the distribution of headache-related disability in the population and identify subgroups of patients requiring health care interventions. As patterns of health care use may also reflect different socio-cultural backgrounds, national and even regional surveys are required, comparing different sample populations.
A self-administered questionnaire survey was therefore undertaken in two areas of Italy, with the following aims: (i) to assess the prevalence of chronic headache in those areas; (ii) to define the main clinical features of the disease, with special reference to pain and the commonest accompanying symptoms; (iii) to report the degree of interference with work and daily living activities; (iv) to outline the diagnostic work-up and the main treatment modalities in clinical practice.
Materials and methods
The Italian Health National Science Service (HNS) serves virtually all the resident individuals and provides a unique source for epidemiological data on several clinical conditions. Medical assistance (which includes office and home calls as well as hospitalizations) is largely free of charge and prescriptions for essential drugs at no cost are possible for any person registered with the HNS. Residents of a study area with a given disease can be traced through the local general practitioners (GPs) who provide medical assistance through office and home visits.
Patients seen by 44 GPs in two areas of Northern Italy (Varese/Sondrio) and Southern Italy (San Giovanni Rotondo) during a 6-month period were the study population. The age and sex distribution of the two populations is illustrated in Table 1. After giving informed consent, each patient was invited to fill up a semistructured questionnaire with data on the presence and clinical characteristics of headache, past diagnostic assessment, current treatment(s), and the impact of the disease on daily living activities (ADL). Headache sufferers were identified among those answering affirmatively the question: ‘Do you usually suffer from headache?’. Patients were then invited to return the questionnaire to the GP who checked its completeness, reported the patient as being (or not being) known to suffer from headache, and attempted to classify the headache according to the International Headache Society (IHS) criteria (1). To improve the quality of the GPs' diagnoses, the neurologists participating in the study (E.B., M.L.M., L.A., M.M.Z.) held seminars on headache characteristics, diagnosis (with special reference to the IHS classification), and treatment.
Age and sex distribution of the target populations in Varese/Sondrio (Northern Italy) and San Giovanni Rotondo (Southern Italy)

The questionnaire was also tested in a pilot study conducted in Varese on a sample of 304 patients with chronic headache, which enabled us to optimize its structure.
Overall and sex-specific period prevalence ratios were calculated from the Poisson's distribution for the entire sample and in the two areas separately. Depending on its interference with ADL, headache was classified as mild (no interference), moderate (interference with work or home activities), severe (interference with work and home activities), and very severe (confined to bed). The correlations between severity and the patterns of health care use were assessed as odds ratios (OR) using the Mantel–Haenszel χ2 test, adjusted for study area.
Results
The study population comprised 1730 individuals from Varese/Sondrio (Northern Italy) and 561 from San Giovanni Rotondo (Southern Italy). The main demographic characteristics of the sample were similar in the two areas (Table 2). There was a slight preponderance of women in both areas. The mean age was 45.5 years (range 2–92) in Varese/Sondrio and 46.6 years (7–90), in San Giovanni Rotondo. Sixty-one percent of the cases had 8 years of education. Unskilled blue-collar workers were the commonest job category (14%), followed by white-collar workers (11%).
Demographic characteristics of the samples in the two study areas (Varese/Sondrio 1730, San Giovanni Rotondo 561)

NS, Not specified.
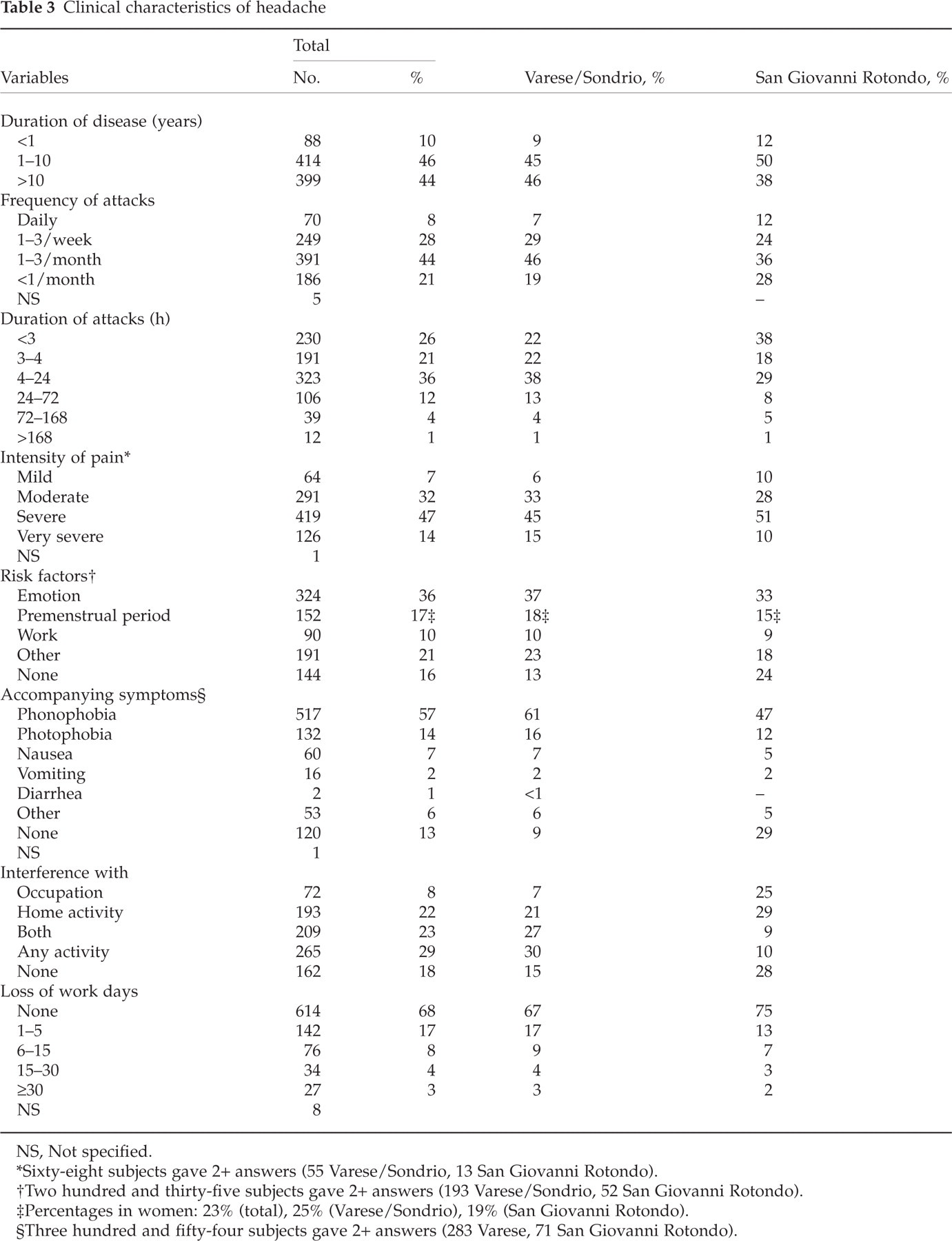
Nine hundred and one persons (39%) declared they suffered from headache (Varese/Sondrio 40%; San Giovanni Rotondo 38%). The period prevalence of headache was 28% in men and 47% in women. The clinical features of headache are shown in Table 3. Forty-four percent of cases reported headache present for> 10 years. The predominant frequency of attacks was 1–3/month and the commonest duration was 4–24 h, with small differences between the two study areas. The pain was mostly moderate to severe and tended to occur after emotion or stress and, in women, during the premenstrual period. Phonophobia was the commonest accompanying symptom, followed by photophobia. Eighty-two percent of cases reported pain interfering with ADL, with moderate differences between the two areas. Interference with occupation was reported by 25% of headache sufferers in San Giovanni Rotondo and interference with any activity by 30% of those in Varese/Sondrio. About one-third of individuals from Varese/Sondrio and one-quarter of those from San Giovanni Rotondo declared loss of work days due to headache attacks.
Clinical characteristics of headache
NS, Not specified.
∗Sixty-eight subjects gave 2+ answers (55 Varese/Sondrio, 13 San Giovanni Rotondo).
†Two hundred and thirty-five subjects gave 2+ answers (193 Varese/Sondrio, 52 San Giovanni Rotondo).
‡Percentages in women: 23% (total), 25% (Varese/Sondrio), 19% (San Giovanni Rotondo).
§Three hundred and fifty-four subjects gave 2+ answers (283 Varese, 71 San Giovanni Rotondo).
Diagnostic and therapeutic approaches to headache tended to differ in the two study populations (Table 4). In general, subjects living in San Giovanni Rotondo reported a larger number of diagnostic tests, including computed tomography (CT) and magnetic resonance imaging (MRI) of the brain. GP and neurologist consultations were commoner in San Giovanni Rotondo, as were hospital admissions for headache. Although the percentages of persons receiving treatment for headache were fairly similar in the two areas, self-treatment was commoner in Varese/Sondrio (31% vs. 5%). There were also more people in Varese/Sondrio whose treatment had been suggested by a pharmacist. By contrast, the majority of people with headache in San Giovanni Rotondo received treatment from their GPs (Table 4). Only 6% of patients with headache in Varese/Sondrio and 4% in San Giovanni Rotondo reported consultation at a headache centre. Non-steroidal anti-inflammatory drugs (NSAIDs) and drug combinations were the leading treatment in both study areas, while use of sumatriptan, β-blockers, tricyclic antidepressants, and muscle relaxants was rare and was reported only in Varese/Sondrio.
Diagnosis and treatment of headache

∗One hundred and forty-nine subjects were submitted +2 diagnostic assessments (91 Varese/Sondrio, 58 San Giovanni Rotondo).
†One hundred and twenty-eight subjects were in treatment with +2 drugs (108 Varese/Sondrio, 20 San Giovanni Rotondo).
NSAIDs, Non-steroidal anti-inflammatory drugs.
Headache was mild in 162 cases (18%), moderate in 265 (29%), severe in 209 (24%), and very severe in 265 (29%). Compared with mild headache, the OR of having a diagnostic work-up was 1.0 for moderate headache, 1.1 for severe headache, and 1.9 for very severe headache (P < 0.0001). The corresponding values for neuroradiological tests were 1.1, 2.4, and 2.7 (P < 0.001). The values for hospital admission were 1.4, 2.7, 3.9 (P < 0.0001) and for headache centre consultation 1.7, 5.8, and 7.9 (P < 0.0001). The ORs for drug treatment were 1.7, 2.1, and 2.8 (P < 0.0001) (self-treatment 0.7, 0.5, and 0.4; P < 0.0001).
The GPs did not specify the headache diagnosis in 27% of their patients, with significant differences between the two areas (Varese/Sondrio 11%; San Giovanni Rotondo 78%) (Table 5). Except for chronic tension-type headache, there were striking differences in the distribution of the main diagnostic categories. Secondary headaches accounted for 7% in Varese/Sondrio and 2% in San Giovanni Rotondo.
Headache diagnosis (International Headache Society)

NS, Not specified.
Discussion
The major weakness of this study may be the method used for the screening process. The question ‘Do you usually suffer from headache’ can be considered vague and perhaps too broad, thus leading to an incorrect estimate of the prevalence of headache in the two Italian communities. However, based on the use of this simple, patient-orientated question, similar prevalence rates were obtained from the two study areas (Varese/Sondrio 40%; San Giovanni Rotondo 38%). In addition, the Italian version of the question (‘Lei soffre di mal di testa?’) is phrased in such a way that persons with episodic or chronic headache can be separated from persons by whom the symptom is perceived as an unusual complaint. By contrast, the use of more restrictive screening criteria could lead to selection bias (towards more severe or physician-orientated headache varieties).
The prevalence of headache has been estimated to range from 35% to 84% in men and from 46% to 95% in women, depending on the study populations and methods of assessment (2). In our study, 28% of men and 47% of women complained of headache, with small differences between the two study areas. Although the comparability of the data from Varese/Sondrio and San Giovanni Rotondo strengthens the validity of our findings, our rates are lower than in most other reports. The prevalence estimates tend to vary significantly with the target population, the epidemiological index (point, period or lifetime prevalence), and the type of interview (3). In this study, the period prevalence of headache was reported, which leads to a fairly conservative estimate of the frequency of the disease.
The characteristics of pain in our sample population tend to confirm the variability of the impact of headache on each individual. Population-based studies (4) report different measures of pain and disability in headache sufferers. Although the frequency and duration of headache attacks can be assessed more objectively than intensity and provoked disability, no straightforward measures of pain are available. Several scales have been developed to assess the degree of interference caused by headache, with or without reference to the degree of limitation in work or social function (5, 6). Interference with work is a valuable measure of disability, but does not entirely define the impact of headache on ADL because unemployed persons are excluded, loss of work days is seen only in a subgroup of headache sufferers, and other social functions, such as leisure activities, interactions with others, etc., are not considered. This study assessed headache severity and its impact on ADL with reference to simple categories defined by the interference with work and/or home activities. On this basis, the patterns of health care use were significantly correlated to headache severity and the degree of functional impairment.
In our study 30% of people with headache had skull X-rays, 21% had an EEG and 10% a CT scan or MRI. As there is no justification for the use of EEG to screen for malignant headache aetiology (7), and the utility of neuroimaging for headache in patients with a normal neurological examination is very limited (total yield of pathology 2.4%) (8), these findings merit some comment. The use of diagnostic aids tends to reflect the national patterns of health care (9) and does not necessarily follow guidelines dictated by evidence-based medicine. Defensive medical practice and the positive emotional impact of negative testing must also be considered. The wide range of use of CT scans across countries (2–57%) (10, 11) confirms our data and can be explained on this basis.
The GP is still the leading physician consulted for headache in Italy. This is in keeping with other European countries with similar health care systems (10, 12), although lower consultation rates (12–13% for men and 18–19% for women) have been reported by others (13–15). A neurologist was consulted by 18% of cases, while 11% used emergency departments, and 6% were referred to a headache centre. Like access to technology, the referral to specialists and the use of emergency departments may reflect the national and local patterns of health care, with the highest rates found in North America (9, 16).
Despite the frequent consultations by headache sufferers, our GPs were unable to classify 27% of cases according to the IHS categories, with significant differences between the two study areas. More specifically, the GPs in San Giovanni Rotondo did not classify the headache type in 78% of their patients. In addition, an IHS diagnosis of migraine (with or without aura) was reported in 40% of cases (Varese/Sondrio 51%) and tension headache (whether chronic or episodic) in 23% (Varese/Sondrio 26%). This is in contrast to several other reports showing a clear predominance of tension headache in the general population (17). These findings probably reflect an inadequate use of the IHS classification by Italian GPs, which seems most common in Southern Italy. This finding is in contrast with Olesen and Rasmussen's belief that ‘ … It is possible to classify virtually all chronic headache patients using the IHS classification …’ (18). A possible interpretation of the GPs' incorrect use of the IHS classification is the limited knowledge of the patient's headache. Interestingly, the use of the IHS categories was inversely correlated here to the number of subsidiary diagnostic and therapeutic aids.
There are other possible explanations for the problems our GPs had with the classification of the headache phenotypes within the IHS categories. First, muscle contraction and migraine symptoms may coexist in the same patient (19–22). Second, there is the tendency for headache characteristics to change over time (23, 24). Third, the effects of medical and self-treatment may obscure manifestations of the headache syndromes. Fourth, there is still uncertainty that migraine and tension-type headache are distinct disorders with a different biological basis (25). Fifth, several studies tend to confirm the limited validity (3, 26, 27) and reliability (28) of the IHS classification criteria based on the proband report or medical interview.
Of our patients, 27% were self-medicated and 49% did not report their headaches to the GP, with significant differences between the two study areas. In a population-based US study, 29% of men and 41% of women declared their headache had been diagnosed by a doctor (29). In Canada, only 64% of migraine and 45% of tension-type headache had ever sought medical attention (16). Even larger amounts of over-the-counter medications were taken by patients from other countries: France 50% (12), Japan 57% (30), Canada 90% (16). The medications used in this study (mostly NSAIDs) were similar to those in other countries (9, 31). Our low rate of prophylactic medication, which is confirmed by other reports from general practice (32) or households (12), tends to reflect the heterogeneity of headache patterns in our population and the low proportion of headache sufferers who may need chronic prophylaxis.