
Abstract
Headache prevalence, characteristics and impact in adults were measured using a cross-sectional general population survey in North Staffordshire, UK. A postal survey was mailed out to 4885 adults (aged ≥ 18 years) with an adjusted response rate of 56% (n = 2662). Of respondents 93% reported headache ever and 70% in the last 3 months. Women and younger people reported higher headache prevalences. Of those reporting headache in the last 3 months, 23% experienced headache at least weekly and 16% experienced severe headache pain. Headaches affected work, home or social activities in 43% of sufferers and 20% reported at least moderate headache-related disability. Higher levels of disability were associated with higher levels of pain, 61% with severe disability reporting severe pain compared with 13% who had mild or moderate disability. In the total adult population sample headache affected more than two-thirds in the last 3 months and 14% of all adults reported headache-related disability of at least moderate level, which translates to a large burden in the general population.
Introduction
Headaches are a public health problem both in terms of the number of people experiencing headache and the effects of headaches on work and social functioning. A population survey in Denmark has shown a lifetime prevalence of headache of over 90% in both men and women (1). UK studies have found the 1 year prevalence of headache to be 63.5–83.6% for men and 78.4–90.4% for women (2–7). Although there have been population-based studies of specific headache diagnoses such as migraine, the most recent UK studies which investigated all headaches was published more than 20 years ago.
The impact of headaches and their associated disability on the lives of sufferers can be considerable, including reduced quality of life (8), reduced capability for work (9, 10) and a detrimental effect on relationships and social activities (11). However, headache treatment in the UK is largely through self-care, with evidence from family or general practitioner (GP) records that <20% of patients consult their GP because of headache in a 5-year period (12, 13). Similar results were found in a Canadian study, with 87% of headache sufferers using over-the-counter (OTC) medicines compared with 26% using prescription medicines (11).
The implications of this are that most headaches will not be identified through studies of health care users, and that much of the societal burden of headache may only be identified by studies outside the clinical arena which are not restricted to specific diagnostic categories. We have therefore carried out a survey which estimated the prevalence, characteristics and impact of headache in a UK general population.
Methods
The design of the study was a cross-sectional postal survey of an adult population sample using a self-completed questionnaire. Five practices from the North Staffordshire GP Research Network were recruited to the study and 1000 adults aged ≥ 18 years were randomly selected from each practice list. The practices were selected to contain a mix of urban and rural settings, and a spread of social class. In the UK, about 98% of the population are registered with a GP and so practice registers provide a convenient frame for sampling a local population (14). The samples were then checked by the GPs for exclusions (e.g. severe psychiatric or terminal illness). The questionnaires were mailed with a letter from their GP practice and a study information leaflet, and reminders sent to non-responders after 2 and 5 weeks.
The North Staffordshire Headache Survey questionnaire consisted of five sections: headache experiences, headache effects and medicines used, advice sought about headaches, general health, and demographic information. The questionnaire was developed using a combination of literature sources, advice from physicians and researchers, and recognized standard instruments. The questionnaire has been previously tested in three ways: (i) pilot study in a general population sample; (ii) validation study comparing headache consulters from primary and secondary care with the pilot study responders; and (iii) reliability study in the general population sample. We have reported this elsewhere (15).
Respondents were asked to include in their responses all headaches of all types. They were first asked if they had ever experienced a headache and then if they had experienced a headache in the previous 3 months. Those who reported headache in the previous 3 months were asked for more information about their headaches in that 3-month period. They were asked for descriptions of their headaches in terms of frequency, duration, and pain severity, together with symptoms experienced with their headaches. The effects of those headaches were then measured in terms of actions taken and medication or other therapies used. Disability was measured using the Migraine Disability Assessment (MIDAS) (16), a previously validated schedule developed in migraine sufferers. All respondents were asked their gender, date of birth, ethnic group, employment status and occupation (own and partner's) to determine household occupational social class (17, 18).
On return of the completed questionnaires, the date of birth and gender given by respondents were checked against those from the surgery records to ensure the replies were from the intended respondents. Data were entered onto a prepared database and checked for errors. Ethical approval for the study was obtained from the Local Research Ethics Committee.
Statistical analysis
Data analysis consisted of simple frequencies of prevalence, headache characteristics and impact, stratified by demographic variables. People who delay response may share characteristics with non-responders, and so to gain insight into non-response characteristics we compared headache prevalences of early and late responders. Age and gender of responders and non-responders were compared to determine if the responders were representative of the whole sample. Estimates of general population headache prevalence were then calculated by direct standardization, applying the study age/gender-specific prevalences to the age and gender structure of the original 5000 sample and to an estimate of the UK population in 1999 (19). Prevalences obtained for employment status and social class were adjusted to account for age and gender by indirect standardization. Cross-tabulations of headache features and effects were performed to determine if there were any associations between the variables. Statistical analysis was performed in SPSS 10.0 (20).
Results
Four thousand eight hundred and eighty-five questionnaires were mailed and 2698 (55.2%) completed questionnaires were returned after three mailings. Subsequent to the mailing of the first batch of questionnaires there were 57 deaths and departures from the practice and 71 questionnaires were returned as addressee unknown. During the data cleaning, 36 questionnaires were found to have been completed by someone other than intended. Thus 2662 completed questionnaires were received from a possible 4757, giving an adjusted response rate of 56.0%.
One thousand four hundred and eighty-seven (55.9%) of respondents were female and the median age of respondents was 52 years (range 18–98 years). There were differences between the genders in the age distribution of the respondents: 24.0% of females were aged 18–35 compared with 18.9% of males. More than half the respondents were employed, either full or part-time, and almost one-third retired. There were subjects categorized into each of the social classes and only a very small number of respondents from non-white ethnic groups. This ethnic response reflects the population structure of this particular district of England (21) (Table 1).
Characteristics of responders (n = 2662)

∗These groupings do not total 2662 due to missing data.
Comparisons of responders and non-responders are shown in Table 2. Response was higher in women than men, 60.7% compared with 50.9%, and higher in older age groups than younger, 65.1% age ≥ 66 years compared with 43.3% of 18–35-year-olds.
Age and gender of responders and non-responders (n = 4757)

∗Percentage difference in gender of 9.9% (95% CI 7.0–12.7%).
†χ2 3 = 143.6, P < 0.001.
Headache prevalence
Lifetime prevalence of headache was 92.6% (n = 2466) and 3-month prevalence was 70.3% (n = 1871). Women reported higher prevalence of headache compared with men for both lifetime and 3-month periods. Headache prevalence, particularly 3-month prevalence, decreased with increasing age (Table 3).
Lifetime and 3-month headache prevalence and responder characteristics (n = 2662)

Headache prevalence was not related to employment status. It was, however, lower in retired respondents and higher in those in full-time education. There was a general decrease in 3-month headache prevalence by social class (Table 3), but indirect standardization confirmed that this was explained by age and gender differences (data not shown).
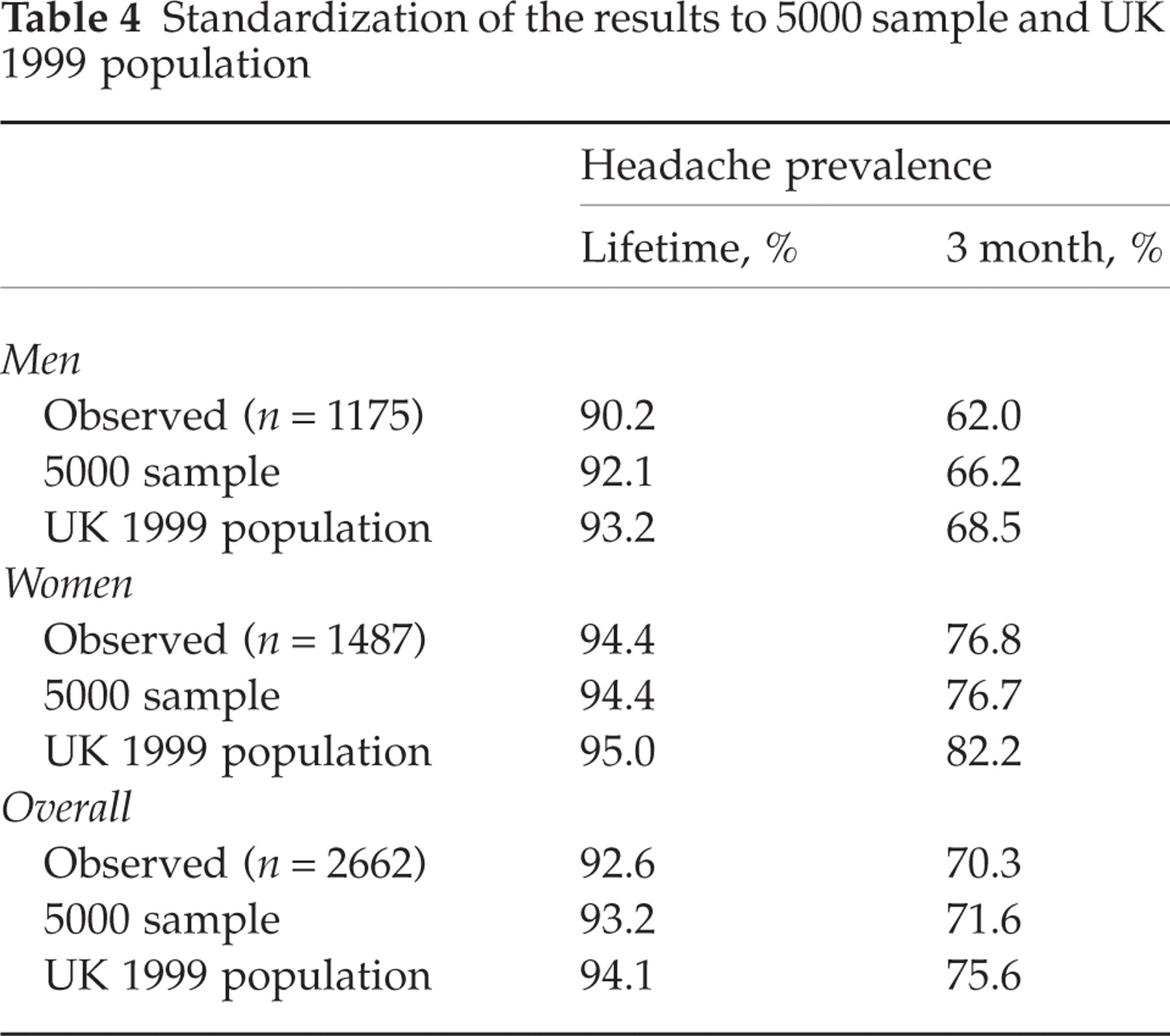
Standardized estimates of headache prevalences to the original 5000 sample and to an estimate of the UK 1999 population were generally higher than the observed prevalences (Table 4). There was no association between speed of response and headache prevalence, lifetime or 3 month (Table 5).
Standardization of the results to 5000 sample and UK 1999 population
Headache prevalence of early and late responders (n = 2662)
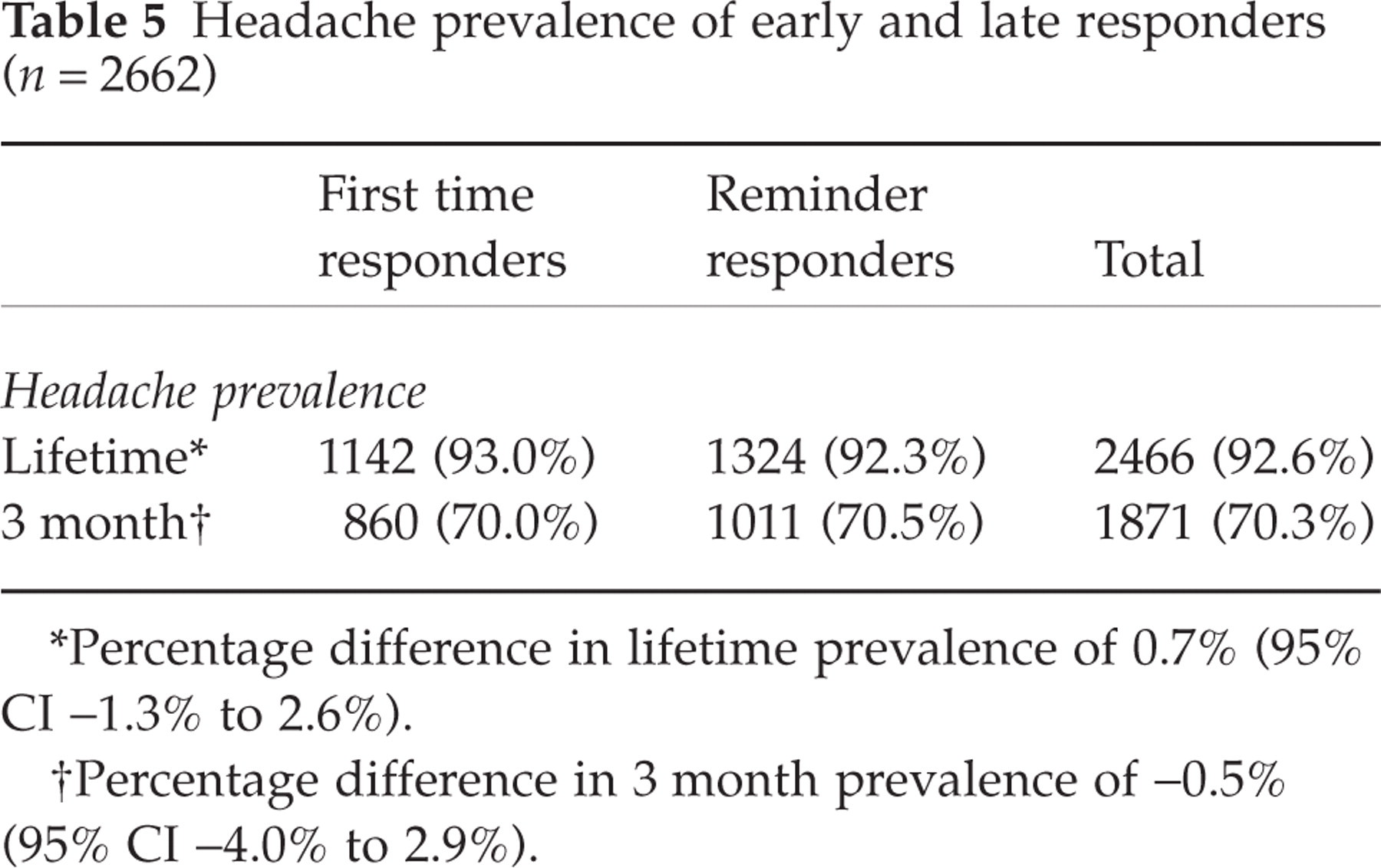
∗Percentage difference in lifetime prevalence of 0.7% (95% CI −1.3% to 2.6%).
†Percentage difference in 3 month prevalence of −0.5% (95% CI −4.0% to 2.9%).
Headache characteristics in the previous 3 months
Three-quarters of headache sufferers reported headache affected them less than once a week in the previous 3 months (Table 6). Most of the remainder experienced headaches one to three times a week and only a small number (5.7%) reported headache more than three times a week. For most, headaches lasted on average less than 4 h whether untreated or treated. However, for a few, headaches lasted more than 24 h. Of the 1124 respondents who reported duration both for untreated and treated headaches, the majority (687, 61.1%) reported shorter duration headaches when treated, one-third (372, 33.1%) that headache duration remained the same, and a small number (65, 5.8%) reported longer duration for treated headaches. One-sixth of headache sufferers rated the pain from their headaches in the previous 3 months as ‘severe’ or ‘extremely severe’, but for most it was described as ‘mild’ or ‘moderate’. When extrapolating to all the survey respondents, these results suggest that 16% of adults experience a headache at least once a week and 11% experience headaches of at least severe pain, but only a small number experience headaches lasting more than 1 day (5% untreated and 3% treated).
Headache characteristics in the previous 3 months

∗These groupings do not total 1871 due to missing data.
Respondents were asked whether they had experienced a number of symptoms with some, most or all their headaches in the previous 3 months (Table 6). One-quarter of sufferers reported experiencing five or more of those symptoms with at least some of their headaches, representing almost one-fifth of all respondents (18.2%).
Most headache sufferers (1313, 70.2%) reported waking with a headache at least one morning in the previous 3 months and 12.6% (235) woke with a headache on more than six mornings. However, a substantial number (514) of these reported that they thought at least some of their headaches were due to drinking alcohol.
Impact of headaches in the previous 3 months
More than 40% (796) of headache sufferers reported at least 1 day in the last 3 months affected by missed or reduced ability in work, home or social activities. Headaches had affected work in 388 (20.7%) headache sufferers with 400 missed and 1571 reduced ability work days in 3 months. These effects expressed in terms of all respondents in employment, irrespective of headache status, were estimated as follows. A total of 1390 respondents reported they were in employment (1021 full-time and 369 part-time) and if we assign part-time workers to half of full-time work this represents 1205.5 workers. Expressed in yearly terms, this is a total of 6540 work days affected per 1000 workers per year (1327 missed and 5213 reduced ability days). Missed or reduced ability household work days due to headache were reported by 610 (32.6%) headache sufferers, totalling 2189 missed and 2084 reduced ability household work days. A total of 1292 days missed social, family or leisure activities due to headache in the last 3 months were reported by 358 (19.1%) headache sufferers. Headache-related disability (MIDAS) was determined based on these reports of missed and reduced ability, and 366 (19.5%) of headache sufferers reported at least moderate level disability during the last 3 months, which represents 13.7% of the total respondents (Table 7).
MIDAS grade and impact of headaches in the previous 3 months (n = 1871)

∗Includes 1075 (57.5%) who reported no disability due to headache (MIDAS score = 0).
More than half of headache sufferers reported that headaches resulted in them needing to lie down and rest, for 10.7% (116) this was every headache and for 89.3% (969) some of their headaches. When asked specifically about the previous 3 months, 50.5% (944) of headache sufferers reported lying down and resting for an hour or more due to headache on at least 1 day.
Respondents with a headache at work are most likely to take a headache or pain killing medicine and continue as normal (821, 66.4%), most of the rest would ignore their headache (403, 32.6%) and only a very small number would stop and rest (13, 1.0%). However, if they had a headache at home more would stop and rest (261, 15.2%), a similar number treat their headache and continue (1140, 66.3%), and fewer would ignore their headache (319, 18.5%). For the 1207 (64.5%) headache sufferers who reported both their work and home strategies, more than two-thirds (825, 68.4%) would follow the same course of action at work or home. Most of the rest (337, 27.9%) reported that they would do more when they had a headache at home, e.g. take pain-killing medicine at home, whereas at work they would ignore the headache and continue as normal.
Associations with headache reports
Women differed from men in their headache characteristics (Table 6). They were more likely to report headache one or more times a week compared with men (25.3% vs. 20.7%). They had longer lasting headaches in all age groups, were more likely to rate their headache pain as severe or extremely severe (20.6% compared with 12.1%), and were more likely to report other symptoms with their headaches, e.g. almost twice as likely to report experiencing vomiting with their headaches.
Measures of severity tended to correlate with each other. Respondents reporting at least one headache a week were three times more likely to report ‘severe’ or ‘extremely severe’ pain compared with those reporting less frequent headaches, 36.0% compared with 11.5%. Those reporting headaches lasting>24 h were about four times more likely to report their headache pain as at least ‘severe’, 57.6% compared with 12.6% for untreated headaches. Headache sufferers with severe or very severe disability reported more frequent headaches, 63.2% reported headaches at least once per week compared with 18.9% of those reporting mild or moderate disability, and longer duration headaches with 30.1% reporting untreated headaches>24 h compared with 7.3% of those reporting mild or moderate disability. Higher levels of disability were also associated with higher levels of pain – almost four times as many respondents with severe or very severe disability reported severe or extremely severe pain, 60.8% compared with 12.6% of those reporting mild or moderate disability. Conversely, over 40% of those reporting severe or extremely severe pain reported only mild disability.
Discussion
Headache had a high prevalence in this population survey, with over two-thirds reporting headache in the previous 3 months and>90% ever having had a headache. Headache was found to be more common in women and younger respondents. In the previous 3 months, one in six respondents had experienced at least one headache per week and one in 10 at least severe headache pain. Women reported more frequent, longer lasting and more painful headaches compared with men. They were also more likely to have experienced other symptoms with their headaches.
Nearly one-third of respondents reported that headaches had resulted in at least one missed or significantly reduced ability work or household work day, or missed social, family or leisure activities day in the last 3 months. Headache-related disability of at least a moderate level affected 13.7% of the respondents’ lives in the 3 months prior to the survey.
The study asked respondents for information about all their headaches in the past 3 months, no matter what type. This has the advantage of being able to assess the impact of headache generally but means that the information cannot be related to individual headache diagnoses. The study also assessed headache for all ages of adult and is therefore particularly useful in having data for older adults.
Non-response bias occurs where the responders differ from the non-responders to a survey in the disease occurrence and characteristics. We investigated this in two ways. First, there was no difference in headache prevalence between early and late responders, suggesting no major response bias. Second, we standardized our estimates to the target and UK populations, because of age and gender differences in responders. This suggested our sample prevalence was a slight underestimate (Table 4).
The numbers from non-white ethnic groups were very small (n = 19) and they were also not an ethnically homogeneous group, and so inferences cannot be made with respect to ethnic group effects. The data relating to these 19 respondents was not removed as the numbers were too small to affect overall findings.
Headache prevalence in our study was similar to that in other UK and European studies (2–7, 22–25). The current study had a shorter prevalence period than these other studies (3 months compared with 1 year), in order to reduce recall problems, and the prevalence estimate was in the lower range of previous headache prevalence estimates. The headache prevalences from our study also demonstrate the lower prevalence in males and older age groups as found in those studies.
Compared with an Italian study of headache clinic attenders (26), respondents in our study were more likely to take medication and continue what they were doing in reaction to headache, 66% at both work and home compared with 52% and 38%, respectively, in the Italian study. They were less likely to stop and rest when they have a headache, 1% would do so at home and 15% at work compared with 13% and 44%, respectively, in the Italian study. The differences are likely to be due to the more severe headaches in the Italian clinic attenders, but similar percentages in both studies would continue what they were doing without taking medication, approximately one-third at work and one-fifth at home.
Information gathered on other symptoms associated with headache were designed to reflect the International Headache Society (IHS) migraine criteria (27). Although we cannot say that all accompanying symptoms reported were experienced in the same headache episode, respondents reporting five or more of these symptoms could be described as ‘likely migraineurs’. This group represents 18.2% of the survey respondents, 13.1% males and 22.3% females. Recent European studies using IHS criteria have estimated the prevalence of migraine as 10–13% overall and 6–8% in men and 15–18% in women (1, 22, 23, 25, 28). The ratio of males to females in our group was 1:2.15 compared with an expected ratio of 1:3 in migraine sufferers (1), and as expected most (72.8%) were aged ≤ 50 years. Thus, our method would slightly overestimate the migraine prevalence and, although it is likely that it is sensitive in detecting migraine sufferers, it is not specific enough to exclude non-migraineurs.
An estimated 1.8% of responders reported headaches with untreated duration of>4 h per day occurring more than three times per week. This definition parallels IHS criteria for chronic daily headache (CDH) (29, 30) of>15 days of headache per month with a duration of>4 h per day untreated or unsuccessfully treated. However, 34 respondents with headache more than three times per week did not report untreated headache duration, suggesting that CDH in our population may be between 2% and 3%. Compared with recent studies of CDH in the general population, our result was similar to a questionnaire study (23) which found prevalence was 1.5% but rather lower than recent studies in which clinical interviews were used and which had estimates of between 3% and 5%(31–33).
The relationship between disability and pain reflects that seen in other studies both of headache and other painful conditions (34, 35) where, although there is an increase in disability associated with increased pain, not all respondents reporting severe pain reported disability with their headaches. The increasing disability with both increasing headache frequency and duration will be, in part, due to the disability measure reflecting the number and duration of headaches in its count of missed and reduced ability days.
The implication of the effects of headaches for employers is demonstrated by a crude estimate of the percentage of work days affected by headache. The reported missed work days represent an approximate 0.5% of working days for all employed respondents, irrespective of headache status, and reported reduced ability days represent 2.0% of working days; thus, a total of 2.5% of working days in the adult population were affected by headaches.
The decline in headache prevalence with age is, at present, unexplained. One possibility would be that headache prevalence is increasing over time and there is a cohort effect. However, the prevalences obtained in studies more than 20 years ago indicate that headache prevalences were similar in the same age groups in our study (2–7). Thus, headache prevalence appears to have a genuine decline with increasing age. Possible explanations for this are recall problems in older people (whilst this may affect lifetime reports, it is less likely to affect 3 month reports), the presence of other diseases which may mean that headaches go unnoticed, concomitant use of analgesics may disguise any headaches and, finally, headache sufferers may die younger. However, these possible explanations would have to have a large combined effect to explain the differences observed. Further research may help to determine if any of these factors contribute to the observed decline in headache prevalence with increasing age.
Our study demonstrates the high prevalence of headache and its effects, with more than two-thirds of the adult population experiencing a headache in a 3-month period and 14% of all adults reporting at least moderate headache-related disability. This is a considerable burden to society not only in terms of individual pain and disability but also the societal effects of missed and reduced capacity in work and home activities.
Footnotes
Acknowledgements
We would like to thank the North Staffordshire GP Research Network for their assistance with the study. We would also like to thank the network team and administrative staff from the Primary Care Sciences Research Centre and administrative staff from the Department of Medicines Management, Keele University for their help and support with the study. Survey costs were funded by the Proprietary Association of Great Britain.