
Abstract
This study investigates the associations between migraine on the one hand and lifetime major depression, lifetime panic disorder, and neuroticism evaluated using the Swedish universities Scales of Personality on the other. A neurologist clinically assessed 728 women aged 40-74 years attending a population-based mammography screening programme. The associations between lifetime migraine and personality traits and psychiatric disorders were insignificant in multivariable analysis. However, in old women (60-74 years) the risk for active migraine was strongly associated with a history of major depression and high levels of stress susceptibility and somatic trait anxiety. Furthermore, in old women, high levels of stress susceptibility and somatic trait anxiety were associated with low ratings of migraine pain intensity and lower levels of these traits with high ratings after controlling for disability during migraines, whereas there were only small differences in middle-aged women. The results suggest that certain aspects of neuroticism are important mental correlates of the ability of old women to endure migraine pain.
Introduction
Migraine, major depression, and panic disorder pose a public health problem. These disorders are characterized by their episodic occurrence. Drugs used to treat them usually affect the serotoninergic system. There is evidence from some cross-sectional and longitudinal studies (1–4) in the general population that depression and anxiety disorders are associated with migraine, but there are other studies that do not support this (5, 6) or show inconsistencies between cross-sectional and longitudinal findings (7). A relationship between migraine and neuroticism has been suggested, but the literature is conflicting (6, 8–10). Few studies have focused on middle-aged and older women.
There is substantial evidence from cross-sectional studies that the prevalence of migraine decreases with age (11–14). According to a meta-analysis (15), the peak prevalence is found at around the age of 40 years. Based on the same population as in this study, we recently reported that the prevalence of active migraine headache declines by 50% by an increase in age of 10 years (16). There was evidence to suggest that the decline in prevalence of migraine headache is caused by a decrease in migraine pain intensity. In women with active migraine, the pain intensity and the proportion of women experiencing nausea declined with age, but not the proportion of women experiencing severe disability during attacks. Such an apparent discrepancy could be explained by age-related factors with the potential to reduce the ability to cope with migraine pain. We hypothesized that these factors could be psychiatric disorders or certain personality traits related to neuroticism.
This study has two major goals. First, we test if there is an association between a history of migraine at any time during life on the one hand and major depression, panic disorder, and neuroticism on the other. Second, we test if lifetime major depression, panic disorder, and neuroticism have age-specific effects on the prevalence and pain intensity of active migraine.
Study population and methods
Study population
The study population has been described in greater detail previously (16). All women aged 40–74 years in Östhammar, a small community in Sweden, are invited regularly to a mammography screening programme (MSP). The MSP is characterized by a high attendance rate; approximately 79% of all invited women attend the local mammography unit (MUT), 7% attend the central MUT, and 14% do not respond to the invitation (16).
We asked 838 women who attended the local MUT to participate in our study. Of the 996 invited women, 158 did not attend the MUT. Of the 838 attending women, 686 women agreed to participate in the present study at the local MUT and 42 women later agreed to participate in the present study in their homes. Thus, 728 women (86.9% of 838) participated in our investigation. In this study, women aged 60–74 years are referred to as old women.
Interview, measures, and definitions
Participants were interviewed by a board-certified neurologist with experience in clinical psychiatry (P.M.). Physical and neurological examinations were not performed. If there was insufficient time for the interview, it was completed over the telephone (n=92). The interview was semi-structured and focused on migraine, major depression, and panic disorder.
The interview structure was based on the headache criteria proposed by the International Headache Society (IHS) (17). Migraine headache is referred to as migraine. The criteria for migraine corresponded to the headache phase of migraine without aura, irrespective of whether the participant experienced a visual aura in conjunction with a migraine headache attack or not. Participants were considered to have active migraine if they fulfilled all criteria in at least one attack of migraine during the previous year.
Participants were asked about the headache characteristics and related symptoms of the most painful parts of their typical untreated or unsuccessfully treated attacks. All women with migraine experienced inhibition (moderate disability) or prohibition (severe disability) of daily activities during migraine attacks.
We used a verbal analogue scale to measure pain intensity. Women were given the extreme values of this numerical scale, which ranged from 0 (‘no migraine pain’) to 10 (‘migraine pain as intense as you can imagine’). Then they were asked to rate the average pain intensity of the most painful part of their typical untreated or unsuccessfully treated attacks experienced in the previous year. Pain intensity measured in this way is not a criterion for migraine. Frequency was measured in 10 predetermined categories as the number of days in the previous year during which the women had headache. Duration of migraine attacks was measured in 10 predetermined categories as the number of hours during which an attack lasted.
The Primary Care Evaluation of Mental Disorders (PRIME-MD) was used to assess the presence or absence of DSM-III-R major depression or panic disorder (18). The screening questions and clinician evaluation guide in the PRIME-MD were modified to obtain lifetime and 1-year data on major depression and panic disorder. Only lifetime data on major depression and panic disorder were used for pre-planned analyses in this study. We did not ask about bipolar disease.
Personality traits were evaluated using the Swedish universities Scales of Personality (SSP) (19). The SSP are based on the Karolinska Scales of Personality (KSP), which were developed for the purpose of measuring theoretical constructs defining vulnerability to different forms of psychopathology (20, 21). The inventory comprises 91 items grouped in 13 scales with seven items in each scale. Each item is presented as a statement with a four-point response format, ranging from ‘does not apply at all’ (=1) to ‘applies completely’ (=4). The values were summarized for each personality trait.
A factor analysis of the correlations of scales in this study was equivalent to the factor analysis in a normative sample (19). We decided to select five scales reflecting different aspects of neuroticism as they were related to the hypothesis in the present study. These were Embitterment (E; unsatisfied, blaming and envying others); Lack of assertiveness (LA; lacks ability to speak up and to be self-assertive in social situations); Psychic trait anxiety (PsTA; worrying, anticipating, lacking self-confidence); Somatic trait anxiety (STA; autonomic disturbances, restless, tense); and finally Stress susceptibility (SS; easily fatigued, feeling uneasy when urged to speed up).
The quartile corresponding to the lowest levels of a particular trait was given the suffix ‘1’ and the highest levels ‘4’. For example, the quartile corresponding to the highest levels of embitterment was referred to as ‘E4’.
All women gave their informed consent for participation, and the Ethics Committee of the Medical Faculty, University of Uppsala approved the study (No. 97307).
Statistical analysis
The statistical program package JMP (version 4.0) was used. Ninety-five percent confidence intervals (CIs) in logistic regression were calculated via maximum likelihood estimates. P-values <0.05 were considered significant. All tests were two-sided.
According to the second major goal of this study we were interested in differences in age-specific effects of two psychiatric disorders and several personality traits. The number of comparisons that could have been made was more than 100. The problem of multiple comparisons can be handled either by selecting as few variables as possible or by making changes in the significance level. We decided to select few variables and keep an unadjusted significance level. Since a recent study indicated that the risk of migraine was significantly increased in women scoring in the upper quartile of the neuroticism scales (6), we decided to analyse our data in a similar way. The distributions of the personality traits were divided into quartiles. We looked for ‘large’ differences in migraine prevalence between the highest quartile and the other quartiles and between the lowest quartile and the other quartiles of each personality trait scale. Large was not defined in terms of a predetermined difference in percentage, but was rather a decision that we made after visual inspection of the data. In order to investigate the relationship between vulnerability to major depression and migraine, lifetime prevalences were used.
Educational levels were combined into two classes (elementary, comprehensive, or secondary school vs. any higher educational level) in all analyses. Age was divided into three classes (40–49, 50–59, and 60–74 years).
The choice of a particular statistical method was based mainly on the type of outcome data that were to be analysed. The odds ratio (OR) for migraine by lifetime major depression and panic disorder was estimated by logistic regression (22, 23) after adjustments for age and education. The risk for lifetime migraine by personality traits was adjusted by lifetime major depression and panic disorders, since there is evidence that major depression and anxiety disorders may change this risk estimate (6). Ordinal logistic regression analysis was used to test for associations between psychiatric disorders and personality traits on the one hand and the ordinal variables pain intensity, frequency, and duration of attacks on the other.
The correlations among the scales of the personality traits were subjected to a factor analysis. Principal axis factoring was used to identify factors with an eigenvalue >1. The preliminary factor structure was rotated using the Varimax method. The reliability of the scales was measured by Cronbach's alpha.
Results
In five women it was not possible to obtain sufficient details concerning psychiatric symptoms because of language difficulties. This left 723 women for psychiatric evaluation. The 40 women who participated in their homes did not receive the personality questionnaire. Thirty women did not return the questionnaire. Four women were excluded because their questionnaires contained too many missing values. This left 649 women for the analysis of the personality traits. The mean age of the 649 women whose data were used in the analysis of personality traits was 53.7 (SD 9.7) years. The mean age of the original study population (n=728) was 54.1 (SD 9.8) years.
Prevalences
The 1-year and lifetime prevalences of migraine were 17.8% (95% CI 15.1–20.6) and 31.3% (95% CI 27.9–34.6), respectively. Among the 286 women aged 40–49 years there were 108 women (37.8%) with a history of migraine at any time during their lives. Among the 215 women aged 50–59 years there were 64 women (29.8%) with a history of migraine at any time during their lives. Among the 222 women aged 60–74 years there were 54 women (24.3%) with a history of migraine at any time during their lives. Among the 528 women with low educational levels there were 155 women (29.4%) with a history of migraine at any time during their lives. Among the 195 women with high educational levels there were 71 women (36.4%) with a history of migraine at any time during their lives.
The lifetime prevalences of major depression and panic disorder were 29.2% (95% CI 25.9–32.5) and 4.8% (95% CI 3.3–6.4), respectively. The proportion of women with lifetime migraine, lifetime panic disorder and LA1 decreased significantly with age (χ2=10.9, 2 DF, P=0.004, χ2=9.1, 2 DF, P=0.01 and χ2=11.0, 2 DF, P=0.004, respectively). The proportion of women with lifetime major depression, E4, PsTA4, SS4, and STA4 did not vary significantly with age.
Factor analysis and reliability of scales
Similar to the factor analysis of the normative data (19), the correlations of the 13 scales yielded a three-factor model. Mainly STA (factor loading 0.70), PsTA (factor loading 0.90), SS (factor loading 0.74), E (factor loading 0.69), and LA (factor loading 0.78) loaded on factor 1 (eigenvalue=4.87). The reliability of these five scales related to neuroticism was 0.85 (Cronbach's alpha). The individual scales ranged from 0.77 to 0.84.
Associations between lifetime migraine and psychiatric disorders and personality traits
Lifetime migraine was not associated with lifetime major depression (OR=1.23, 95% CI 0.87–1.73) or panic disorder (OR=1.17, 95% CI 0.56–2.36). Interaction terms between lifetime major depression and age and between lifetime panic disorder and age were not statistically significant.
The lifetime prevalence of migraine was calculated for each quartile of the personality traits (see Table 1). After visual inspection of the distribution of total migraine in each quartile, we decided not to make inferences about embitterment, lack of assertiveness, and psychic trait anxiety, but to test for the simultaneous effect of stress susceptibility (SS1–3 vs. SS4) and somatic trait anxiety (STA1–3 vs. STA4) on migraine, while controlling for age, education, panic disorder, and major depression. In this model there was no significant increase in risk for migraine in women scoring in SS4 (OR=1.50, 95% CI 1.00–2.24, P=0.051) in comparison with women scoring in SS1–3. STA was not a risk factor for migraine (P=0.11). Interaction terms between STA and age and between SS and age were not statistically significant.
Prevalence of migraine stratified by quartiles of five personality traits

Associations between active migraine and psychiatric disorders and personality traits
After visual inspection of the distribution of active migraine in each quartile, we decided not to make inferences about psychic trait anxiety, but to analyse the effect of lack of assertiveness (LA1 vs. LA2–4), embitterment (E1–3 vs. E4), stress susceptibility (SS1–3 vs. SS4), and somatic trait anxiety (STA1–3 vs. STA4; see Table 2), and major depression and panic disorder on active migraine. The prevalence of active migraine was plotted against age (three age classes) for women scoring in LA1 and LA2–4, E1–3 and E4, SS1–3 and SS4, STA1–3 and STA4, and for women with and without the psychiatric disorders, which is exemplified in Fig. 1. On visual inspection there was no large difference between the age-specific prevalence of active migraine in women scoring in LA1 in comparison with women scoring in LA2–4 or between E1–3 and E4. For this reason we did not perform statistical tests regarding the effects of LA and E.
Active migraine by major depression, stress susceptibility, somatic trait anxiety, and age

∗Degrees of freedom and LR χ2 value of models 1–3 in addition to the degrees of freedom and LR χ2 value of the reference model. The P-value corresponds to the change in χ2 value. Age was divided into three classes (40–49, 50–59, and 60–74 years). Education was divided into two classes. MDD, Major depression; SS4, the upper quartile of the stress susceptibility scale; STA4, the upper quartile of the somatic trait anxiety scale. The P-values of the interaction terms were 0.009, 0.009, 0.04 in models 1, 2, and 3, respectively.
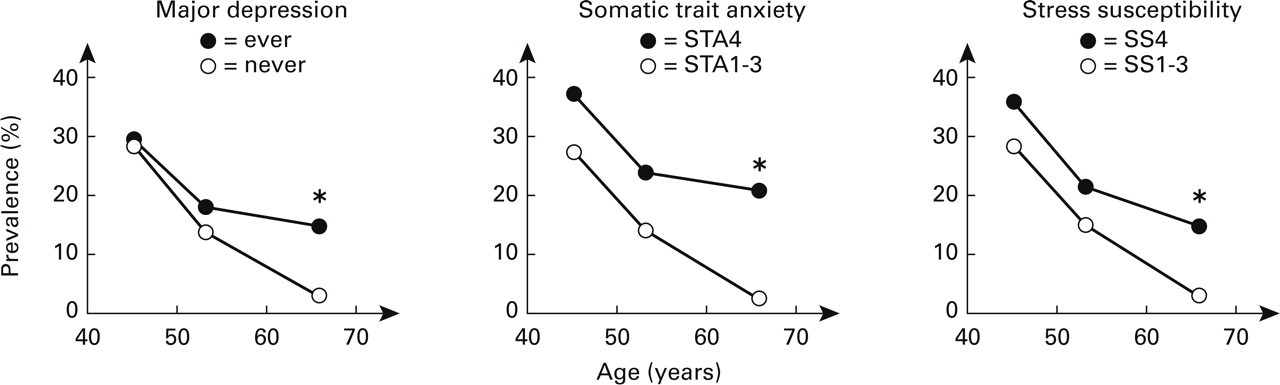
The age-specific prevalence of active migraine stratified by lifetime major depression, level of stress susceptibility, and level of somatic trait anxiety. Women scoring in the fourth quartiles (STA4 or SS4) had high levels of somatic trait anxiety or stress susceptibility. Significant interactions (∗P<0.05) indicate that the differences in the prevalence of active migraine between old women with and without major depression, old women scoring in STA4 and STA1–3, or old women scoring in SS4 and STA1–3, are larger than the corresponding differences in middle-aged women.
After controlling for differences in educational levels, there were significant differences in the prevalence of active migraine between STA1–3 and STA4, SS1–3 and SS4, lifetime major depression and no lifetime major depression in women aged 60–74 years (P=0.0002, 0.003, and 0.002, respectively), but there were no significant differences in women aged 40–49 or 50–59 years. Lifetime panic disorder had no significant effects on active migraine in any single age class or in the whole population. The effects of STA4, SS4, and lifetime major depression on active migraine were tested one-by-one in three models. The reference model contained age and education (n=623, 3 DF, χ2=48.99 for major depression and n=649, 3 DF, χ2=47.33 for SS4 and STA4). We included interaction terms, since the differences in prevalence of active migraine appeared larger in old than in middle-aged women. The final models are presented in Table 2. The addition of lifetime major depression and an interaction term between lifetime major depression and age (60–74) (Model 1, 5 DF, χ2=58.62) increased the explained variance significantly. The addition of STA4 and an interaction term between STA4 and age (60–74) (Model 2, 5 DF, χ2=65.70) increased the explained variance significantly. The addition of SS4 and an interaction term between SS4 and age (60–74) (Model 3, 5 DF, χ2=58.11) increased the explained variance significantly The P-values of the three interaction terms (between age (60–74) and lifetime major depression, age (60–74) and STA, and age (60–74) and SS) were 0.009, 0.009, and 0.04, respectively. The significant interaction terms indicate that the difference in the prevalence of active migraine between old women with lifetime major depression, scoring in STA4, or SS4 and old women without lifetime major depression, scoring in STA1–3 or SS1–3, respectively, is larger than the corresponding differences in middle-aged women. The simultaneous effect of lifetime major depression, STA, SS and the corresponding interaction terms was not tested due to small numbers.
In the 82 women aged 40–49 years with active migraine there were four women (4.9%) with major depression in the previous year. In the 33 women aged 50–59 years with active migraine there were five women (15.1%) with major depression in the previous year.
In the 14 women aged 60–74 years with active migraine there was no woman (0.0%) with major depression in the previous year.
Associations between the pain intensity of active migraine and psychiatric disorders and personality traits, controlling for disability
Our next goal included an analysis of whether there were age-specific differences in pain ratings between women with and without lifetime major depression, women scoring in STA1–3 and STA4, and women scoring in SS1–3 and SS4. These analyses and the analyses of the age-specific differences in prevalences were done in a similar way. There were 129 women eligible for the analysis of major depression and 123 women eligible for the analyses of STA and SS. After plotting the mean pain intensity scores of migraine for three age classes (40–49, 50–59, and 60–74 years) against the median age of the age classes (45, 53, and 63.5 years) (Fig. 2), we observed that the differences were larger among old women than in middle-aged women, i.e. the patterns were similar to those for differences in prevalences. Therefore, we fitted three models (Table 3) to analyse age-specific effects of major depression, somatic trait anxiety, and stress susceptibility on the intensity of migraine pain. In our previous study (16) we found that the pain intensity declined with age, but not the proportion of women experiencing severe disability during attacks. In the present study there was a high correlation between high pain intensity and severe disability (1 DF, χ2=12.0, P=0.0005). Disability was included in the final models because we wanted to analyse if there were age-specific differences in pain intensity ratings when this factor was held constant.
Pain intensity ratings of migraine by major depression, stress susceptibility, somatic trait anxiety, and age while controlling for disability during migraine attacks

∗Degrees of freedom and LR χ2 value of models 1–3 in addition to the degree of freedom and LR χ2 value of the reference model. The P-value corresponds to the change in χ2 value. Age was divided into three classes (40–49, 50–59, and 60–74 years). Disability was divided into two classes. MDD, Major depression; SS4, the upper quartile of the stress susceptibility scale; STA4, the upper quartile of the somatic trait anxiety scale. The P-values of the interaction terms were 0.69, 0.01, and 0.003 in models 1, 2, and 3, respectively.
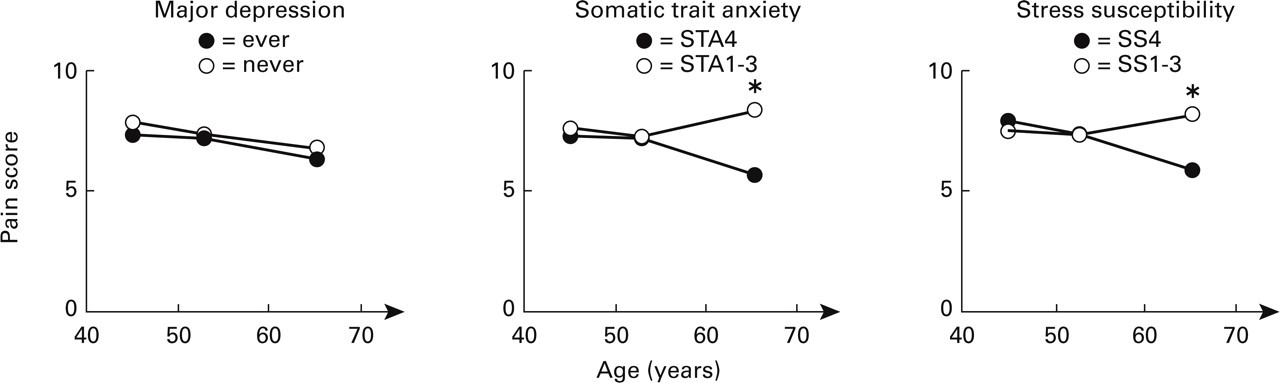
The age-specific mean rating of migraine pain intensity stratified by major depression, level of stress susceptibility, and level of somatic trait anxiety. Women scoring in the fourth quartiles (STA4 or SS4) had high levels of somatic trait anxiety or stress susceptibility. Pain intensity was measured on a verbal analogue scale, ranging from ‘No migraine pain’ (=0) to ‘Migraine pain as intense as you can imagine’ (=10). Significant interactions (∗P<0.05) indicate that the differences in pain intensity ratings between old women with high levels and lower levels of stress susceptibility and somatic trait anxiety are significantly larger than the corresponding differences in middle-aged women.
Continuous data (means) are shown in Fig. 2, but we used ordinal logistic regression to make inferences. The reference model (n=129, 3 DF, χ2=17.68 for major depression and n=123, 3 DF, χ2=14.96 for SS and STA) contained age and education. The addition of lifetime major depression and an interaction term between lifetime major depression and age (60–74) (Model 1, 5 DF, χ2=18.81) did not increase the explained variance significantly. The addition of SS4 and an interaction term between SS4 and age (60–74) (Model 2, 5 DF, χ2=23.98) increased the explained variance significantly. The addition of STA4 and an interaction term between STA4 and age (60–74) (Model 3, 5 DF, χ2=23.20) increased the explained variance significantly. The P-values of the interaction terms were 0.69, 0.01, and 0.003 in Models 1, 2, and 3, respectively. The estimates of the interaction terms were larger than zero. These results indicate that the difference in pain intensity ratings between old women with high levels (scoring low in pain intensity ratings) and lower levels (scoring high in pain intensity ratings) of stress susceptibility and somatic trait anxiety is significantly larger than in middle-aged women, when differences in disability during migraines are held constant.
Seventy-seven (62.6%) of 123 women experienced moderate disability and 46 women (37.4%) experienced severe disability during migraine attacks. Among old women scoring in STA4, 38% (three of eight) experienced severe disability during migraines. Among old women scoring in STA1–3, 25% (one of four) experienced severe disability during migraines. Among old women scoring in SS4, 50% (four of eight) experienced severe disability during migraines. None of the four old women scoring in SS1–3 experienced severe disability during a migraine attack.
Post hoc analyses
Since the discussion of the direction of causes may include the argument that neuroticism is a response to recurrent severe headaches, we tested whether pain intensity, disability, duration, or frequency of attacks were associated with STA or SS in post hoc analyses in the whole population of women with active migraine (n=123). In women scoring in STA1–3, the median pain intensity rating was 8, the median number of days with migraine was 7–9, the median duration was 19–24 h, and 38.8% experienced severe disability. In women scoring in STA4, the median pain intensity rating was 7, the median number of days with migraine was 10–12, the median duration was 13–18 h, and 34.9% experienced severe disability. In women scoring in SS1–3, the median pain intensity rating was 8, the median number of days with migraine was 7–9, the median duration was 19–24 h, and 35.7% experienced severe disability. In women scoring in SS1–3, the median pain intensity rating was 8, the median number of days with migraine was 7–9, the median duration was 13–18 h, and 40.1% experienced severe disability. The pain intensity, disability, frequency, and duration of migraine attacks in women with active migraine did not differ between women scoring in STA1–3 and STA4 or between women scoring in SS1–3 and SS4 (nominal and ordinal logistic regression analysis).
Discussion
Main findings
To the best of our knowledge, this is the first population-based study focusing on migraine and psychiatric disorders in which a neurologist has clinically assessed the participants. In this study of middle-aged and older women we found no association between lifetime migraine on the one hand and lifetime major depression, panic disorder, or personality traits related to neuroticism on the other. The most interesting findings were that high levels of stress susceptibility and somatic trait anxiety had effects on the prevalence of active migraine, and the pain intensity ratings of recent migraine attacks were more pronounced in old women than they were in middle-aged women. The differences related to pain intensity were significant after adjustments for differences in disability during attacks. We believe that these findings are important.
The criteria for migraine in this study corresponded to the headache phase of migraine without aura of the IHS classification, irrespective of whether or not the participant experienced a visual aura in conjunction with a migraine headache attack or not. The IHS classification does not require that subjects with migraine without aura experience any reduction in their abilities during migraines, but all women with migraine in this study experienced disability during their migraines. Migraines not associated with disability during attacks have been shown to be very rare (24). In a clinical situation, and particularly in an epidemiological setting, headaches without concomitant disability are very difficult to recognize as migraines.
In a previous study of this cohort (16) the pain intensity of migraine declined with age, but not the proportion of women experiencing severe disability. These results indicated that there might be a threshold of pain intensity measured by means of a verbal analogue scale for IHS-defined migraine headache. Our interpretation of the present findings is that migrainous women with high levels of certain neuroticism-related personality traits continue to have migraine attacks when they grow older because they already experience moderate to severe disability at low levels of migraine pain intensity. As a consequence of this, they are more likely to fulfil the disability criterion and thereby also the criteria for migraine. Changes in the incidence of migraine are probably not important. In fact, no old woman with a history of migraine experienced her first migraine attack after the age of 40 years (data not shown).
The theoretical construct of neuroticism includes the assumption that persons with a high degree of neuroticism are sensitive and vulnerable to various stimuli, including pain. Because old women with high levels of stress susceptibility and somatic trait anxiety experienced disability during attacks at low levels of migraine pain intensity, we hypothesize that they are vulnerable to migraine pain. Ageing is characterized by a reduced ability to cope with challenges (25). We believe that old women with high levels of certain neuroticism-related personality traits have difficulties in enduring migraine pain, and possibly a reduced ability to cope with the challenge of migraine pain, including pain of mild intensity.
Another interpretation of the data, similar to that in the previous paragraph, would be that high levels of somatic trait anxiety and stress susceptibility in old women lower the intensity-based threshold of severe disability. This is consistent with our prior hypothesis that there is a threshold of pain intensity for IHS-defined migraine headache. Due to the criteria for migraine applied in this study, we cannot answer the question of whether women without disability during migraines have difficulties in enduring migraine pain or a poor ability to cope with that pain. Whether high levels of stress susceptibility and somatic trait anxiety in old women lower the threshold of moderate disability remains unanswered, but we believe they do.
A history of major depression at any time during life had an age-specific effect on the prevalence of active migraine, but not on the pain intensity ratings. The mechanism underlying the age-specific differences in the prevalence of migraine between these two categories is unclear. It has been recognized previously that it is difficult to separate depression and neuroticism in epidemiological research (26).
The relationship between migraine and panic disorder has been studied mainly in young people (1, 4, 5). These studies favour a significant association. In the present study we did not find any significant association. A recent study (7) focused on adults older than 30 years at follow-up. The cross-sectional association between migraine headache and panic disorder was significant, whereas the longitudinal association was not. Future longitudinal studies will show if these disorders are associated also later in life.
Limitations and potential biases
Recall difficulties are a problem in cross-sectional studies (27). The lower prevalence of diseases with advancing age, i.e. lifetime migraine and lifetime panic disorder in this study, may be explained, at least partially, by differential recall between middle-aged and older women.
Evidence of a bi-directional relationship between migraine and major depression has been found in some studies (2, 28), but not in all (7). We conclude from this study that it is unlikely that recent migraine attacks in old women are caused by recent major depression. In fact, there was no woman with major depression during the previous year among the 14 women aged 60–74 years with active migraine. It may be argued that high levels of somatic trait anxiety and stress susceptibility in women with active migraine are a pure psychological response to recurrent severe headaches. This is unlikely, however, because the pain intensity, disability, frequency, and duration of migraine attacks in the whole group of women with active migraine did not differ according to level of somatic trait anxiety or stress susceptibility. Our interpretation of the data is that major depression, stress susceptibility, and somatic trait anxiety have significant age-specific effects on migraine. We plan to conduct a follow-up study of this cohort to analyse these issues and possible secular trends.
The main strength of this study is that the study population is well characterized with regard to migraine and psychiatric disorders. The same neurologist interviewed all participants, which eliminates inter-rater variability. We used a validated diagnostic instrument for psychiatric disorders.
Generalizability
The study population (n=728) was representative of the corresponding sex and age segment of the Östhammar population with regard to age (16). Because of the high participation rates in the MSP and in this study, we believe that the study results are generalizable to all women aged 40–74 years living in Östhammar (n=4398). Personality traits were analysed from data for 649 women. They were on average 0.4 years younger than the women in the original study population. This difference is unlikely to threaten the generalizability of the study. Non-participation is more likely to affect prevalences than associations. However, the estimates of the lifetime prevalence of migraine, 31%, major depression, 29%, and panic disorder, 5%, were similar to the findings of other studies (11–14, 29, 30).
Conclusions
This population-based study of middle-aged and older women adds new information to the extensive literature on the co-morbidity of migraine and psychiatric disorders, and on associations between migraine and personality traits related to neuroticism. The overall impression is that lifetime associations are weak and generally insignificant. However, in old women the risk for active migraine was strongly associated with a history of major depression at any time during life, high levels of stress susceptibility, and high levels of somatic trait anxiety. We suggest that women with these factors continue to have migraine attacks when they grow old. We have previously shown that older women rate the pain intensity of active migraine lower than middle-aged women, but they experience the same degree of disability. The present study indicates that high levels of stress susceptibility and somatic trait anxiety explain this discrepancy by causing old women, but not those who are middle-aged, to be more vulnerable and less able to endure migraine pain, and, possibly, less able to cope with that pain.
Footnotes
Acknowledgements
This research was supported by the Swedish Medical Research Council (grants no. 9523, 12260, and 13245), the Nicke and Märta Nasvell Foundation, and the Foundation for Psychiatric and Neurological Research of Uppsala University.