
Abstract
To investigate further the pharmacological mechanism of an anti-migraine drug, sumatriptan, a 5-HT1B/1D receptor agonist, we studied its effect on the cerebral circulation in seven anaesthetized rats, particularly during hypercapnia. After injection of 0.6 or 6.0 μg/kg sumatriptan succinate, no significant change in cerebral blood flow (CBF) was observed either in the striatum or in the parietal cortex. The increase in CBF both in the parietal cortex and the striatum during 5% CO2 inhalation was significantly less when sumatriptan succinate 6.0 μg/kg was injected. Sumatriptan appeared to have a vasoconstrictor effect on the relaxed vessels by CO2 inhalation. This mechanism might be attributable to vasoconstriction through activation of 5-HT1B receptors located in the vascular smooth muscle rather than 5-HT1B receptors in the vascular adventitia.
Introduction
While migraine is a relatively common disorder and causes significant disability in sufferers, its pathophysiology remains uncertain. Much research on the pathogenesis of migraine has been directed towards new pharmacological treatment. Vascular, neural and trigemino-vascular theories have been proposed to explain the pathogenesis of migraine (1–3). It is speculated that migrainous pain results from vasodilation of intracranial vessels, particularly those in the dura mater, and/or perivascular neurogenic oedema caused by the release of vasoactive neuropeptides from perivascular trigeminal terminals following activation of the trigemino-vascular system.
Cerebral blood flow (CBF) regulation in migraine has also been studied in patients with migraine. Sakai et al. reported abnormal responsiveness of CBF in both hemispheres to CO2 and blood pressure changes in patients with migraine during and between attacks, indicating a functional abnormality in cerebrovascular reactivity (4). Others reported no abnormalities of CBF or its regulation between attacks, while regulation was abnormal within the hypoperfused region during the attack (5).
A highly potent and selective 5-HT1B/1D receptor agonist, sumatriptan, is currently used as an effective acute treatment for migraine (6–14). Despite detailed clinical and experimental investigation, the precise mechanism of action of sumatriptan remains obscure (15–18).
We explored the effect of sumatriptan on the cerebral circulation, particularly when CBF was augmented by hypercapnia.
Materials and methods
Seven male Sprague-Dawley rats (Shizuoka Laboratory Corp., Inc. Hamamatsu, Japan) weighing 350–410 g were anaesthetized by intraperitoneal injection of α-chloralose (50 mg/kg) and urethane (500 mg/kg). The head was fixed by means of a stereotaxic frame. After performing endotracheal intubation, the rats were ventilated with a mixture of room air and oxygen. The right femoral artery was cannulated for measurement of blood pressure; heart rate was derived from the pulse pressure signal. A sample for blood gas analysis was also taken from the cannula. Another cannula was inserted into the right internal carotid artery via the right external carotid artery retrogradely to administer sumatriptan and saline. The pterygopalatine artery was ligated with a thin suture. Arterial blood pH and gases were measured with a pH/blood gas analyser (ABL505 Radiometer, Copenhagen, Denmark). Rectal temperature was maintained at 37.0°C.
Regional CBF in the right parietal cortex supplied by the right middle cerebral artery (4 mm posterior to the bregma and 4 mm lateral to the sagittal suture) was recorded by laser-Doppler flowmetry (ALF21; Advance, Tokyo, Japan) through a thinned bone layer. Regional CBF in the right striatum (1 mm posterior to the bregma and 4 mm lateral to the sagittal suture and 4 mm in depth from the brain surface) was measured by the hydrogen clearance method. The CBF data measured by these two different methods were jointly evaluated in the present study based on the report by Skarphedinsson (19) that there is a linear relation between two methods as to the relative changes in CBF.
The entire experimental protocol is shown in Fig. 1. First, for the normocapnic study, CBF in both regions was measured in the steady state. Then, CBF was measured after carotid infusion of sumatriptan succinate at 0.6 µg/kg per 0.2 ml saline, followed by 6.0 µg/kg per 0.2 ml saline in 2 min using an infusion pump. Second, in six rats, for the hypercapnic study, CBF in the steady state was measured again, and it was measured repeatedly during 5% CO2 inhalation. Finally, CBF was measured during inhalation of 5% CO2 with or without preceding administration of sumatriptan succinate 6.0 µg/kg injection. There was at least a 30-min interval between each CBF measurement. In order to evaluate if the cerebrovascular responsiveness was maintained throughout the study, we examined CO2 reactivity just before sumatriptan administration. Blood gas analysis was performed when each hydrogen clearance curve for the rat brain reached the baseline value on the record.

Entire experimental protocol. The experiment consisted of normocapnic and hypercapnic studies. For detailed explanation, see the text. ST, Sumatriptan; sal, saline.
Statistical analysis was performed by one-way
Sumatriptan succinate (GR43175C) was kindly supplied by Glaxo-Welcome, Research and Development, Stevenage, UK.
Results
Measurement of CBF during normocapnia
Table 1 shows physiological parameters including mean arterial blood pressure (MABP), heart rate (HR), rectal temperature (RT), pH, PO2, and PCO2, during normocapnia. There was no statistical difference in these parameters between steady state and after the infusion of different doses of sumatriptan succinate.
Physiological parameters during normocapnia (n=7)

MABP, Mean arterial blood pressure; HR, heart rate; RT, rectal temperature. Mean±SEM.
In the parietal cortex CBF revealed no significant change after the injection of sumatriptan succinate of either dose. In the striatum, steady-state CBF was 41.3±3.0 ml/100 g brain per min. Following the injection of sumatriptan succinate of two different doses, CBF did not change significantly (Table 2).
Effect of sumatriptan succinate (sumatriptan) on cerebral blood flow (CBF) during normocapnia (n=7)
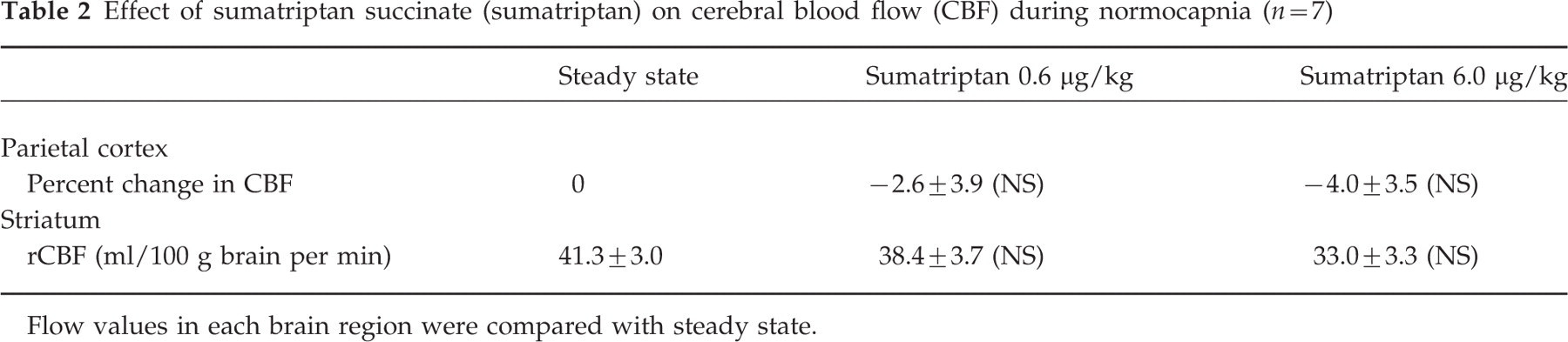
Flow values in each brain region were compared with steady state.
Measurement of CBF during 5% CO2 inhalation
Table 3 shows physiological parameters during hypercapnia. There was no statistical difference in these parameters between the measurements before and after injection of sumatriptan succinate.
Physiological parameters during 5% CO2 inhalation (n=6)

MABP, Mean arterial blood pressure; HR, heart rate; RT, rectal temperature. Mean±SEM.
In the parietal cortex, CBF measured by laser-Doppler flowmetry increased by 37.8±3.4% during 5% CO2 inhalation. When sumatriptan succinate 6.0 µg/kg was continuously injected during 5% CO2 inhalation, the increase in CBF was reduced to 18.2±5.7%, which was significantly less than the increase during the inhalation of 5% CO2 alone (P<0.01). On the other hand, when vehicle (saline) was injected during 5% CO2 inhalation, the increase in CBF was 32.5±4.1%, which was not significantly different from the flow increase without saline (Fig. 2). Since there was no significant effect of sumatriptan succinate at a dose of 0.6 µg/kg in the study of normocapnia (Table 2), the higher dose (6.0 µg/kg) was applied in this hypercapnic study.

Effect of saline and sumatriptan succinate (sumatriptan) on cerebral blood flow (CBF) in the parietal cortex, during inhalation of CO2 in rats. In the parietal cortex, CBF increased by 37.8±3.4% measured by laser-Doppler flowmetry during 5% CO2 inhalation. When sumatriptan 6.0 µg/kg was injected during 5% CO2 inhalation, the increase in CBF was 18.2±5.7%, which was significantly less than the data during only inhalation of 5% CO2 (P<0.01). On the other hand, when saline was injected during 5% CO2 inhalation, the increase of CBF was 32.5±4.1%, which was not significantly different from the flow increase without saline. Values shown are mean and SE from six rats in each group. ∗P<0.01 vs. steady state. †Not significantly different vs. CO2 inhalation. ‡P<0.01 vs. CO2 inhalation. §P<0.05 vs. CO2− saline.
In the striatum, steady-state CBF (46.3±4.9 ml/100 g brain per min) increased to 124.5±11.8 ml/100 g brain per min during 5% CO2 inhalation measured by the hydrogen clearance method. When 6.0 µg/kg sumatriptan succinate was continuously injected during 5% CO2 inhalation, blood flow increase was reduced to 72.6±7.9 ml/100 g brain per min (P<0.01), while it increased to 109.1±8.8 ml/100 g brain per min when vehicle (saline) was injected during 5% CO2 inhalation, which was not significantly different from the flow increase without saline (Fig. 3).

Effect of sumatriptan succinate (sumatriptan) compared with time-matched saline on cerebral blood flow (CBF) in striatum, during inhalation of CO2 in rats. In the striatum, steady-state CBF (46.3±4.9 ml/100 g brain per min) increased to 124.5±11.8 ml/100 g brain per min measured by the hydrogen clearance method during 5% CO2 inhalation. Blood flow only increased to 72.6±7.9 ml/100 g brain per min when sumatriptan 6.0 µg/kg was injected during 5% CO2 inhalation (P<0.01), while it increased to 109.1±8.8 ml/100 g brain per min when saline was injected during 5% CO2 inhalation, which was not significantly different from the flow increase without saline. Values shown are mean and SE from six rats in each group. ∗P<0.01 vs. steady state. †P<0.05 vs. steady state. ‡Not significantly different vs. CO2 inhalation. §P<0.01 vs. CO2 inhalation. ¶P<0.01 vs. CO2− saline.
Discussion
Cerebral and dural vessels consist of three layers: endothelium, smooth muscle and adventitia with nerve fibres and nerve endings. Each structure has receptors for several neurotransmitters, which has been confirmed by physiological, pharmacological or molecular approaches. Serotonin is one of the major neurotransmitters innervating the vessels, and its receptor subtypes have been extensively investigated and disputed. Ullmer et al. (20) reported that 5-HT1B and 5-HT2B receptors, related to vascular relaxation via nitric oxide release, are located in the endothelium. They also reported that 5-HT2A and 5-HT1B receptors, responsible for vasoconstriction, were located in the smooth muscle. On the other hand, Cohen et al. (21) reported that the endothelium contains 5-HT1D and 5-HT7 receptors and that the smooth muscle contains 5-HT1B, 5-HT1D and 5-HT7 receptors. The adventitia contains 5-HT1D receptors in humans and 5-HT1B receptors in the rat, both of which inhibit neurotransmitter release including substance P, calcitonin gene-related peptide, and neurokinin A (22).
In the present study, intracarotid injection of sumatriptan succinate did not affect CBF in either the parietal cortex or striatum. However, this agent appeared to have a vasoconstrictor effect on CBF during the vasodilatory state under hypercapnia.
Previous investigators (23–25) reported that sumatriptan did not alter CBF in the steady state. Perren et al. (23) have shown that sumatriptan has a highly selective vasoconstrictor action on arteriovenous anastomoses within the cranial circulation of anaesthetized cats, but it does not modify CBF. Connor et al. (24) demonstrated that sumatriptan caused a decrease in pial artery diameter in anaesthetized cats when applied perivascularly by microinjection method, but did not constrict pial arteries when administered systemically in the clinically relevant dose. Kobari et al. (25), using a cat model, reported that a high dose of sumatriptan (500 µg/kg) exhibited direct vasoconstrictor actions on the cerebral vessels, but low doses in the therapeutic range elicited no vasoconstriction.
The doses of sumatriptan succinate used in the present study (0.6 and 6.0 µg/kg) were almost equivalent to a clinically effective dose, 6 mg s.c., in terms of Cmax (95.5±20.3 ng/ml) (26), although they were lower than those used in the previous experimental studies. In humans, a single oral dose of 100 or 200 mg (2–4 mg/kg) produced complete or almost complete relief of headache in 50–73% of attacks within 2 h of treatment (8–10). Subcutaneous sumatriptan of 6 mg relieved headache in 70–77% of patients within 1 h of treatment (12, 13). The difference between our data and previous reports regarding sumatriptan-induced changes in CBF could be attributable to the difference in animal species or to the difference in the route of administration. While Connor et al. (24) reported that sumatriptan did not readily penetrate the blood–brain barrier, it is controversial whether this agent can pass through the barrier or not, because it is apparently effective for the acute treatment of migraine and cluster headache. Another speculation is that sumatriptan penetrates regions of the brain devoid of a blood–brain barrier, such as the pineal body, neurohypophysis, area postrema, subfornical organ, organum vasculosum of the lamina terminalis, and the median eminence of the hypothalamus (27).
One of the mechanisms of the beneficial effects of sumatriptan on migraine is vasoconstriction through either 5-HT1D receptor activation in the trigeminal nerves located in the vascular adventitia or activation of 5-HT1B receptor in vascular smooth muscle. In this study, sumatriptan seemed to contract vascular smooth muscle not in the normocapnic state, but in the hypercapnic state. This implies the target of sumatriptan in such conditions as hypercapnic vasodilation may be 5-HT1B receptors in the smooth muscle rather than 5-HT1D receptors in the adventitia.
Recently, Goadsby et al. (28) presented further evidence that serotonin is related to the inhibition of trigeminal nucleus activity, using a combination of the sagittal sinus stimulation model and a potent 5-HT1B/1D antagonist, GR127935. Moreover, Hoskin et al. (29) indicated that the effect of zolmitriptan, another 5-HT1B/1D receptor agonist which is more lipophilic than sumatriptan, is also mediated through this mechanism. These novel findings suggest that the targets of triptans are not confined to the peripheral nervous system, i.e. trigeminal nerve terminals or vascular smooth muscles.
There is no evidence for the relationship between the serotonergic or trigeminal system and cerebrovascular CO2 reactivity. The vascular smooth muscles are responsible for cerebral vasodilatation under hypercapnia. Since 5-HT1B receptors have been demonstrated in the vascular smooth muscles, the vasoconstrictor effect of sumatriptan may well be attributable to the activation of 5-HT1B receptor located in the vascular smooth muscle cells. In an experiment using single photon emission computed tomography in baboons, Oliver et al. (30) reported that sumatriptan could reverse the increased CBF elicited by thiopental. Their results seem to be in accordance with the results of the present study. Sumatriptan may constrict vascular smooth muscles through 5-HT1B receptors only when the vessels are dilated by such mechanisms as CO2 inhalation on thiopental administration. Taken all facts together, sumatriptan seems to counteract the cerebral vasodilation induced by increased PCO2 not only in deep structures, but also in the cortex.
A recent study demonstrated that various cellular compartments in the microvascular bed of the human cerebral cortex express distinct populations of 5-HT receptors in different species, including humans (21). These recent observations may imply that such non-neuronal cells in the brain parenchyma may also participate in the brain serotonergic neurotransmission. The regional difference in the effect of sumatriptan succinate on cerebrovascular CO2 reactivity could be attributed not only to vascular 5-HT receptors but also extravascular 5-HT receptors such as those on glial cells.
In conclusion, the vasoconstrictor effect of sumatriptan through 5-HT1B receptors on vascular smooth muscle rather than those on trigeminal nerve endings in the adventitia might overcome such vasodilation induced by hypercapnia.
Footnotes
Acknowledgements
We thank Yoshihiko Masaki, Department of Laboratory Animal Science, for his technical assistance, and Dr Katsumi Irikura, Department of Neurosurgery, Kitasato University, Sagamihara, for valuable comments on this study. This study was supported in part by a grant from the Mitsui Life Social Welfare Foundation, Japan.