
Abstract
The International Headache Society (IHS) has been criticized for its approach to classification of chronic daily headache (CDH); Silberstein and Lipton criteria provide an alternative to this approach. The aim of this study is to apply the alternative diagnostic approaches to a sample of CDH patients consulting in specialty care. Our sample consisted of 638 patients with CDH. Patients were classified according to both classification systems. Patients were predominantly female (65.0%), with ages ranging from 11 to 88 years. According to the Silberstein and Lipton classification, we found eight different diagnoses. The most common diagnosis was chronic migraine (87.4%), followed by new daily persistent headache (10.8%). Just six patients had chronic tension- type headache (CTTH). Applying the IHS criteria we found 14 different diagnoses. Migraine was found in 576 (90.2%) patients. CTTH occurred in 621 (97.3%), with only 10 (1.57%) having this as the sole diagnosis. We conclude that both systems allow for the classification of most patients with CDH when daily headache diaries are available. The main difference is that the IHS classification is cumbersome and requires multiple diagnoses. The Silberstein and Lipton system is easier to apply, and more parsimonious. These findings support revision of the IHS classification system to include chronic migraine.
Introduction
Chronic daily headache (CDH) is one of the more frequently seen headache syndromes at major tertiary care headache centres, characterized by primary headaches lasting more than 4 h per day on 15 or more days per month (1–3). The prevalence of this group of disorders is 5% in studies of the general population (4–6). The costs and burden of CDH are significant. A study that considered patients with chronic tension-type headache (CTTH) alone found that 11.8% of the sufferers reported lost workdays and 46.5% reported reduced-effectiveness days (7). Patients with CDH have demonstrable and remarkable impairment in most of their activities (8). Mathew et al. (5) reported that patients with CDH who evolved from initially episodic migraine differed from patients with episodic headaches alone regarding abnormal personality profile, elevated depression scores, identifiable stress, medication overuse and hypertension. Most patients with CDH report their role functioning and well-being as frequently and severely impaired (9), highlighting the importance of this group of headaches on quality of life (10).
The classification of daily or near-daily headache remains controversial. Some authors have criticized the International Headache Society (HIS) for not adequately addressing the classification of a very frequent primary headache disorder (while the IHS criteria include both episodic and chronic forms of cluster and tension-type headache, there is no classification for ‘chronic’ migraine) (11, 12). Others believe that the IHS criteria are sufficient and complete and that critiques are based on one or more methodological shortcomings (13).
The aim of this study is to use a large clinical series from The New England Center for Headache (NECH) to review classification issues in CDH. We use our large group of assessed patients and a group of structured medical records to apply both diagnostic systems, the IHS (14) and the criteria proposed by Silberstein and Lipton (12, 15).
Methods
Clinical records and the headache diaries of 638 patients seen between 1980 and 2001 at The New England Center for Headache, P.C., a tertiary referral centre, were reviewed. All patients had daily or near-daily headache lasting >4 h if not treated, for >15 days/month, fulfilling the Proposed Headache Classification for Chronic Daily Headache described by Silberstein and Lipton (12). A small number of patients with incomplete records were contacted directly by one author (M.E.B.) to complete the information. Incomplete records were not included.
During the entire time period reviewed, the Center has been utilizing a uniform clinical intake form and standardized headache calendars (diaries). Before the patient comes to the initial evaluation, they receive a questionnaire in the mail to be completed and returned at the time of the visit. It is then reviewed by a nurse and a headache specialist. This form contains several multiple-choice and fill-in-the-blank items. The following information is systematically collected (16):
All current medications, information about each drug, including dose, schedule, duration of use, degree of relief and side-effects.
All previous headache medication the patient has taken, including preventive and acute care medications for the same parameters described above.
Headache triggers: with 22 specific options, including alcohol, menses, weather, etc.
Relevant past medical history: including accidents, head trauma, loss of consciousness, hospitalizations, etc.
Previous diagnostic tests for the headache disorders and their results.
Prior treatment.
Caffeine, tobacco, and alcohol intake.
Sleep profile.
Self-assessment of the behaviour, mood and anxiety.
At the time of the first visit another spreadsheet is completed by a nurse and subsequently checked by the headache specialist containing information regarding: 1, intensity of pain: pain is graded on a 4-point scale as severe, moderate, mild or no pain.
For all reported intensities of pain the patients present, we record: frequency of pain at the time of the first visit (current) and at onset; location of pain (unilateral, bilateral, alternating sides); quality of pain (throbbing, squeezing, steady, knife-like or other); duration of pain; premonitory features; aura (description and frequency), as well as associated symptoms (nausea, anorexia, vomiting, photophobia, phonophobia, worsening with exertion, osmophobia, dizziness, red eyes, ptosis, tearing, and other).
After analysis of records, the questionnaire and headache calendars, relevant information was transferred to a standardized form that included operational criteria for IHS as well as the proposed Silberstein–Lipton diagnostic criteria. We then reviewed the classification using both sets of criteria. Headache associated with medication overuse or analgesic rebound headache (ARH) was classified according to the IHS criteria in two different ways: (i) strictly applying the IHS criteria, which require the withdrawal of the drug in overuse to make the diagnosis (14); (ii) considering the drug consumption and drug-seeking behaviour to make the diagnosis, using alternative definitions that consider that overuse occurs when patients take three or more simple analgesics a day more often than 5 days a week; triptans or combination analgesic containing barbiturates, sedative or caffeine more often than 3 days a week; opioids or ergotamine tartrate more often than 2 days a week (12, 17–20).
Data were summarized using frequency counts and descriptive statistics.
Results
Our sample consisted of 638 patients, with 415 (65.0%) females, with age ranging from 11 to 88 years. The mean duration of treatment at NECH was 49.2 months.
Table 1 shows the diagnosis according to the Silberstein–Lipton criteria. By far the most common diagnosis in our sample was chronic migraine (formerly termed transformed migraine—87.4%), followed by new daily persistent headache (NDPH—10.8%). Just six (0.9%) patients had pure CTTH. The vast majority of patients were overusing medication (81.7%, Fig. 1). We excluded hemicrania continua from the definition of analgesic overuse, since all patients with this diagnosis received indomethacin on a daily basis.
Classification of patients with chronic daily headache according to Silberstein–Lipton's Proposed 2001 classification (12)


Relative frequency of analgesic overuse in patients with chronic daily headache classified using Silberstein and Lipton proposed 2001 system (12). ▪, With overuse; □, without overuse.
Table 2 shows the diagnosis according to the IHS classification, not considering the needs of withdrawal to make the diagnosis of ARH. With this definition of ARH we were able to classify 631 (99.8%) patients. More than half of them had the concomitant diagnosis of migraine without aura (MO), CTTH and ARH. We used 14 different diagnoses using the IHS system, against eight for the Silberstein–Lipton criteria. Migraine was found in 576 (90.2%) patients. CTTH occurred in 621 (97.3%), with only 10 (1.57%) having this as the sole diagnosis.
Classification of chronic daily headache according to the International Headache Society Classification, without requiring withdrawal to make the diagnosis of analgesic rebound headache

MO, Migraine without aura; MA, migraine with aura; ETTH, episodic tension-type headache; CTTH, chronic tension-type headache; ARH, analgesic rebound headache.
Figure 2 shows the number of concomitant diagnoses when we used IHS criteria, not including the requirement for withdrawal to make the diagnosis of ARH.
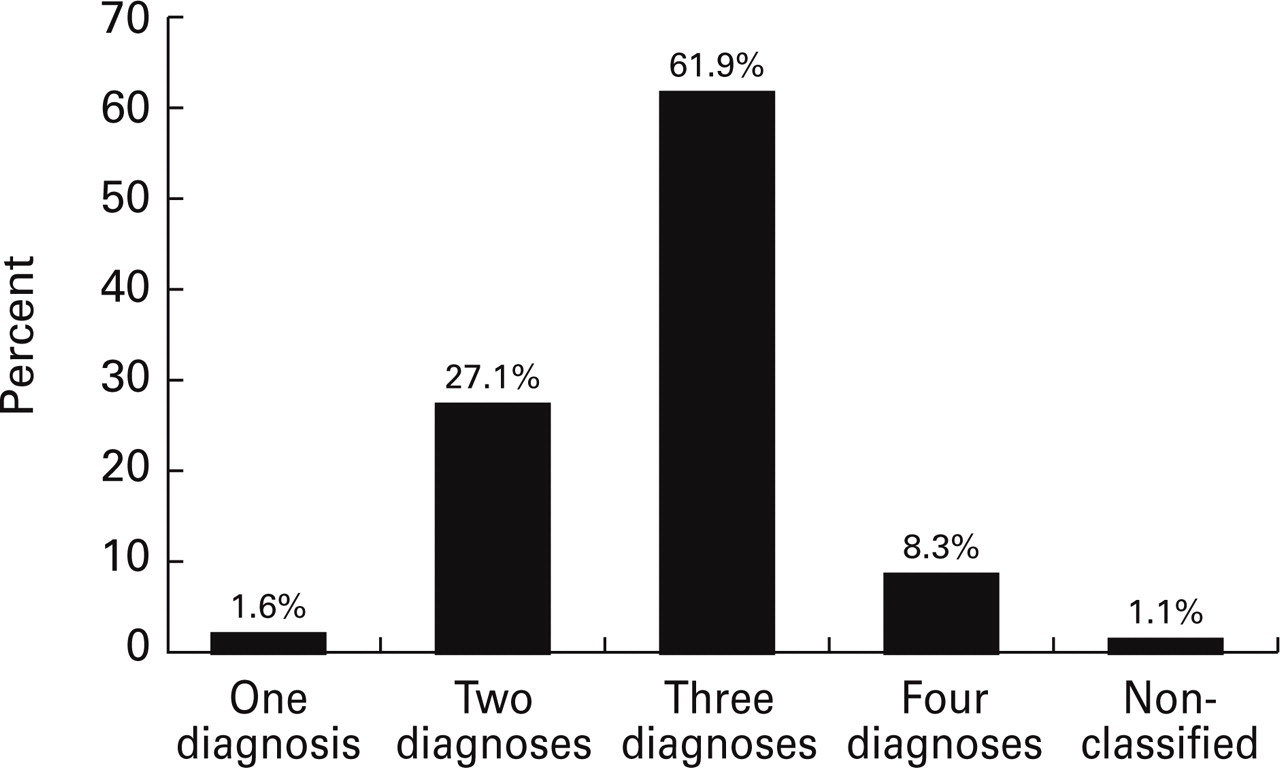
Number of different diagnoses required to classify patients with chronic daily headache using the International Headache Society system.
Table 3 shows the diagnoses when we did include the requirement for withdrawal to make the diagnosis of ARH. Using this set of criteria we were able to classify 625 (97.9%) patients. Migraine was found in 573 (89.8%) and CTTH in 618 (96.8%) patients. We observed an increase in the frequency of the combination of MO and CTTH and a proportional decrease in the combination of MO, CTH and ARH when we required the withdrawal for the diagnosis of ARH.
Classification of chronic daily headache according to the International Headache Society classification, requiring withdrawal to make the diagnosis of analgesic rebound headache

MO, Migraine without aura; MA, migraine with aura; ETTH, episodic tension-type headache; CTTH, chronic tension-type headache; ARH, analgesic rebound headache.
Chronic migraine (CM) and NDPH, the most common diagnoses using the Silberstein–Lipton classification, are not included in the IHS classification. The correlation between both systems in classifying these headaches is presented in Table 4. We found that we had to use six different diagnostic groups using IHS criteria to classify CM and NDPH without overuse and five diagnostic groups to classify CM and NDPH with overuse.
Classification of patients with chronic migraine and new daily persistent headache using the International Headache Society system

Discussion
The classification of daily or near-daily primary headaches remains controversial (21). Although not recognized by the IHS, many authors and clinicians use the term chronic daily headache to define this syndromic group of headache disorders (22, 23).
When designing our study, we tried to follow the criteria of both classification systems strictly, in order to avoid bias. One strength of the present study was the availability of structured clinical records, questionnaires and patients diaries used at NECH over the last two decades. With this amount of clinical information we were able to classify all patients using the Silberstein–Lipton system (Table 1). By far the most frequent diagnosis we found was CM (87.4%), the relative frequency being higher than others reported in the literature. Mathew et al. found that 77% of patients with CDH had what they called transformed migraine (19). Sandrini et al. reported 75% with this diagnosis (24), using the original 1994 Silberstein et al. criteria (15). Probably the reason for the higher relative frequency we are reporting is the fact we used the revised 2001 criteria for transformed migraine (now labelled chronic migraine) (12), which provide for three alternative diagnostic links to migraine: (i) a prior history of IHS migraine; (ii) a clear period of escalating headache frequency with decreasing severity of migrainous features (which were both required in the 1994 criteria); and (iii) current superimposed attacks of headaches that meet all of the IHS criteria for migraine except duration. With these revisions, Silberstein and Lipton reported being able to classify virtually all primary CDH patients and the number of CM diagnoses increased dramatically with a proportional decrease of pure CTTH (12). This increase in the sensitivity brought up possible limitations in the criteria, especially concerning patients that have coincidental migraine and CTTH.
The majority (71.5%) of our patients with CM were overusing medication (Fig. 1), similar to other reports (25). About 80% of CDH patients seen in subspecialty clinics overuse symptomatic medication (20).
NDPH was the second most frequent diagnosis in our data (10.8%). Castillo et al. reported that 2.1% of the CDH in the general population of Spain, not in a specialty clinic, were NDPH (2). With the revised 2001 Silberstein and Lipton criteria we used, virtually every patient not classified as CM or CTTH meet the criteria for NDPH or hemicrania continua (HC) (12).
Interestingly, we classified just six (0.9%) patients with pure CTTH, almost the same prevalence of hemicrania continua. Silberstein and Silberstein, studying 300 patients with CDH, found that just 2% had CTTH (26). It seems that CTTH is not as common as previously thought, especially in tertiary care, as pointed out by Sanin et al. (27). The revised criteria, moreover, tend to be very sensitive to the diagnosis of chronic migraine, which supersedes the diagnosis of CTTH.
We were also able to classify almost all patients using IHS criteria with both definitions of analgesic overuse we used, that is, with or without the requirement for withdrawal (Tables 2 and 3), unlike in some published data (24, 28, 29). The possible explanation is the availability of a wealth of clinical information in the structured spreadsheets and calendars used at NECH, that dramatically reduced the information loss. Thus a frequent drawback of retrospective studies on CDH, missing data, was avoided. The most frequent diagnosis, when we did not require withdrawal to make the diagnosis of ARH, was the combination of MO, CTTH and ARH (50.1%), followed by MO and CTTH (22.1%). This is in agreement with Olesen and Rasmussen (13), who have said that ‘the majority of patients with daily or near-daily headache either have chronic tension-type headache alone or they have attacks which fulfil criteria for migraine without aura in addition to episodic or daily headaches which fulfil criteria for episodic or chronic tension-type headache. Moreover, if they have drug overuse, a diagnosis of “headache induced by chronic substance” use should be added’. The main difference in comparing Silberstein and Lipton's criteria with those of the IHS was the significantly larger number of different diagnoses required when using the IHS system. Just 1.6% of our patients were classified with one diagnosis, the vast majority required three diagnoses (61.9%), and 8.3% required four diagnoses. This reflects, in our opinion, the major problem with the IHS system—in not considering the evolutive history of the patient, it ends up with a vertical stack of multiple diagnoses.
Several studies reported difficulties using the IHS system. Solomon et al. (28) pointed out that the IHS does not take into account the historical features of CDH before it becomes daily. Sanin et al. (27), randomly selecting the clinical records of 400 patients and classifying them using the IHS criteria, concluded that most of their patients had more than one IHS diagnosis, that CTTH occurring alone is rare and that chronic headache classification needs revision. Based on similar studies, some authors concluded that the IHS classification was not comprehensive enough to be used for CDH patients. As a consequence, a few proposals for the classification of these patients have been made (29). Of these proposals, the Silberstein and Lipton criteria (30), recently reviewed (12), have been the most frequently used. The main features of this system are that it is easy to apply and that it considers the evolutive history of the headaches.
Alternatively, Olesen et al. (13) argue that ‘patients with headaches presenting for more than 15 days a month or 180 days a year frequently have several different types of headaches, and the IHS criteria imply that these patients should have a diagnosis of each type of headache. Thus several clinical studies have miscredited the IHS criteria … based on incorrect use of the classification’. These authors also state that the introduction of a classification based on the evolutive history would be hazardous and that the ability of the patients to remember the beginning of their headaches would be a major problem. They claim that almost all the chronic headaches in samples from the general population as well as from clinic populations can actually be diagnosed according to the current criteria using different combinations of diagnoses as required (31).
Symmetry in science is often useful in considering validity of a system. When Albert Einstein revised the Special Theory of Relativity into the General Theory of Relativity, he was moved to do so to correct asymmetries in his overall matrix. The current IHS system is also asymmetric, having episodic and chronic cluster, and episodic and chronic tension-type headache, but not episodic and chronic migraine, episodic and chronic paroxysmal hemicrania, or episodic and chronic hemicrania continua.
The need for an excessive number of diagnoses when applying the IHS system is corroborated by analysis of Table 4. We required six different combinations of diagnoses to classify using the IHS system, when these patients were classified into one diagnosis with the Silberstein and Lipton criteria.
Another important difference is that by not considering the natural history of the headache syndrome, the IHS system fails to describe adequately the group of patients with NDPH. The most frequent IHS diagnosis for these patients, when they were not overusing analgesics, was the combination of MO and CTTH, the same combination observed when we classified CM patients using the IHS. Clinically, we feel that these patients present differently, have differing responses to medication, and often have different outcomes.
We conclude that both systems allow for the classification of most patients with CDH when daily headache diaries are available. The main difference is that the IHS classification is cumbersome and requires multiple diagnoses. The Silberstein and Lipton system is easier to apply, being more parsimonious (one diagnosis instead of many). The revisions consider the natural history of patients in arriving at a diagnosis, and are reassuringly symmetric. These features, simplicity, symmetry, and consideration of natural history, lead us to suggest that the Silberstein and Lipton criteria for chronic migraine and new daily persistent headache should be adopted in the new IHS classification system to improve diagnosis and research.
Footnotes
Acknowledgement
Financial support for this study was provided by AstraZeneca.