
Abstract
Hemicrania continua is an uncommon primary headache disorder. This study of nine patients compares two different classification systems, proposed by Pareja et al. and Goadsby and Lipton. Although it seems logical to position the nosologic status of hemicrania continua under group 3 of the International Headache Society Classification, as proposed by Pareja et al., the Goadsby and Lipton classification is more clinically useful and should be included in future International Headache Society reclassification.
Introduction
Hemicrania continua (HC) is an uncommon primary headache disorder first described as a syndrome in 1984 by Sjaastad and Spierings (1). It is a unilateral headache absolutely responsive to indomethacin, thus being one of the indomethacin-responsive headache syndromes (2). During the next 5 years of its description, the number of HC cases reported increased to 18 (3). This relatively small number of cases reported in the literature at that time may have been one reason for not including HC in the International Headache Society (IHS) classification system (4, 5). This disorder is expected to be addressed in the upcoming revision (6). A clinical description of HC was included in the International Association for the Study of Pain classification (7).
The relative rarity of HC has made it difficult to study its pathophysiology and nosologic status. At present two different classifications do exist, one being a revision of the criteria first described (4), the other being a more recently proposed classification (8).
The aim of this study is to compare both classifications regarding their operational criteria.
Methods
Clinical records and the headache diaries of 9 patients with HC seen between 1990 and 2001 at the New England Center for Headache, a tertiary referral centre, were included after being randomly selected and reviewed. All patients have been followed for at least 2 consecutive years. During the entire time period reviewed, the centre had utilized a uniform clinical intake form and patient headache calendars. The clinical intake form contains information regarding:
intensity of pain (pain is graded on a three-point scale as severe, moderate or mild);
frequency of pain;
location of pain;
quality of pain;
duration of pain;
presence or absence of aura and associated symptoms; and
behaviour during attacks.
After analysis of records, spreadsheets and headache calendars, relevant data were transferred to a standardized form that included operational criteria for both proposed classificatory systems, namely the criteria proposed by Pareja et al. (4) and by Goadsby and Lipton (8). We then reviewed the classification using both sets of criteria.
Results
Our sample consisted of nine patients, seven (77.7%) females, with age ranging from 34 to 61 years (mean=46.2 years). The mean follow-up period was 29.2 months.
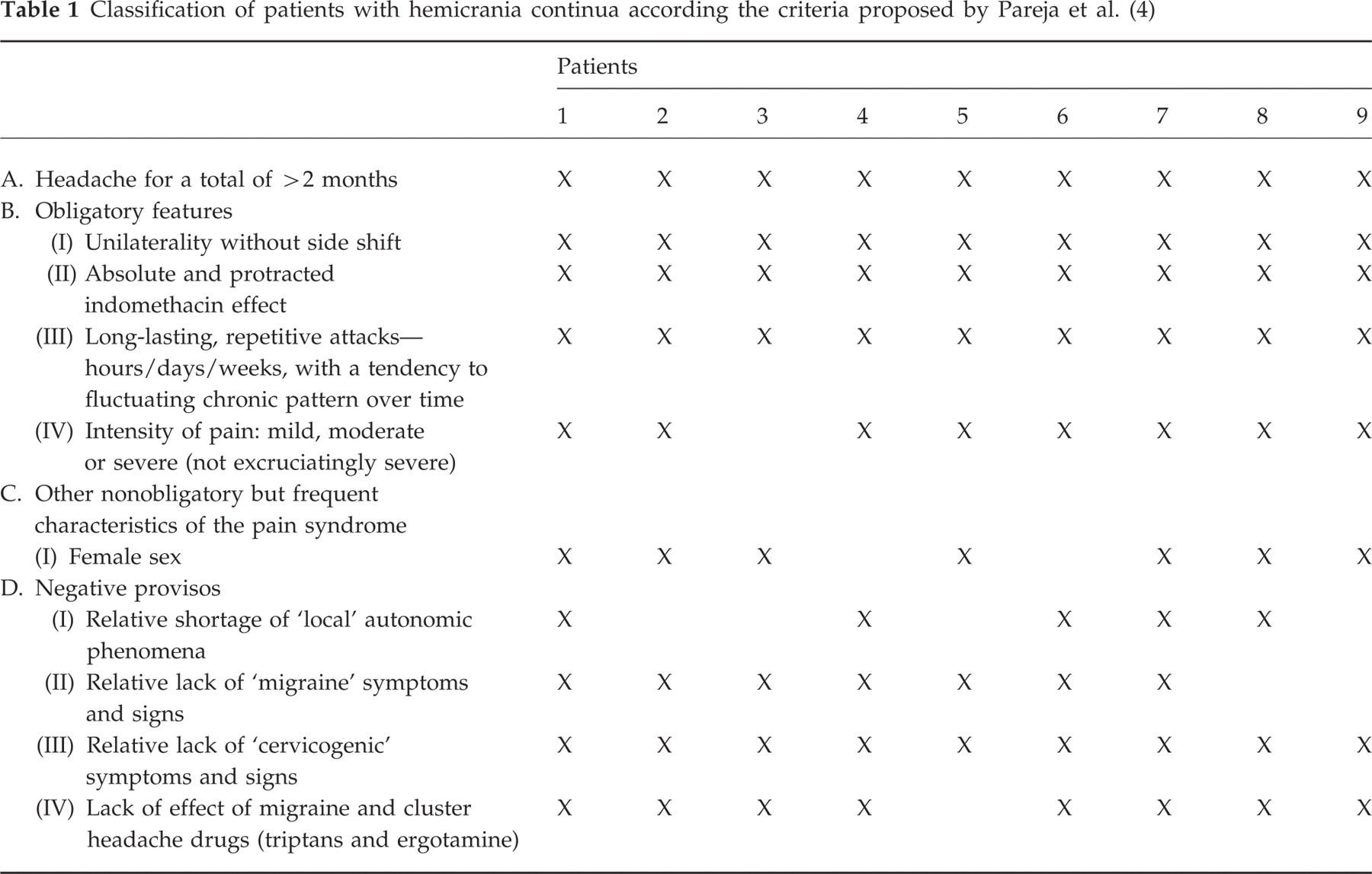
Table 1 shows the diagnoses utilizing proposed criteria as set forth by Pareja et al. (4). All patients had side-locked unilateral headache and absolute responsiveness to indomethacin. One patient (number 3) did not fulfil all obligatory criteria, the reason being the intensity of ‘excruciatingly’ severe pain on occasion. Two patients did not fulfil item C (non-obligatory) criteria. Four patients (44.4%) demonstrated, especially in pain exacerbations, autonomic phenomena (described in Table 2), consequently not fulfilling item DI. Similarly, two patients demonstrated migraine features during the exacerbation, not fulfilling criteria DII. One patient (number 9) reported partial relief with ergotamine (negative proviso IV).
Classification of patients with hemicrania continua according the criteria proposed by Pareja et al. (4)
Classification of patients with hemicrania continua according the criteria proposed by Goadsby and Lipton (8)
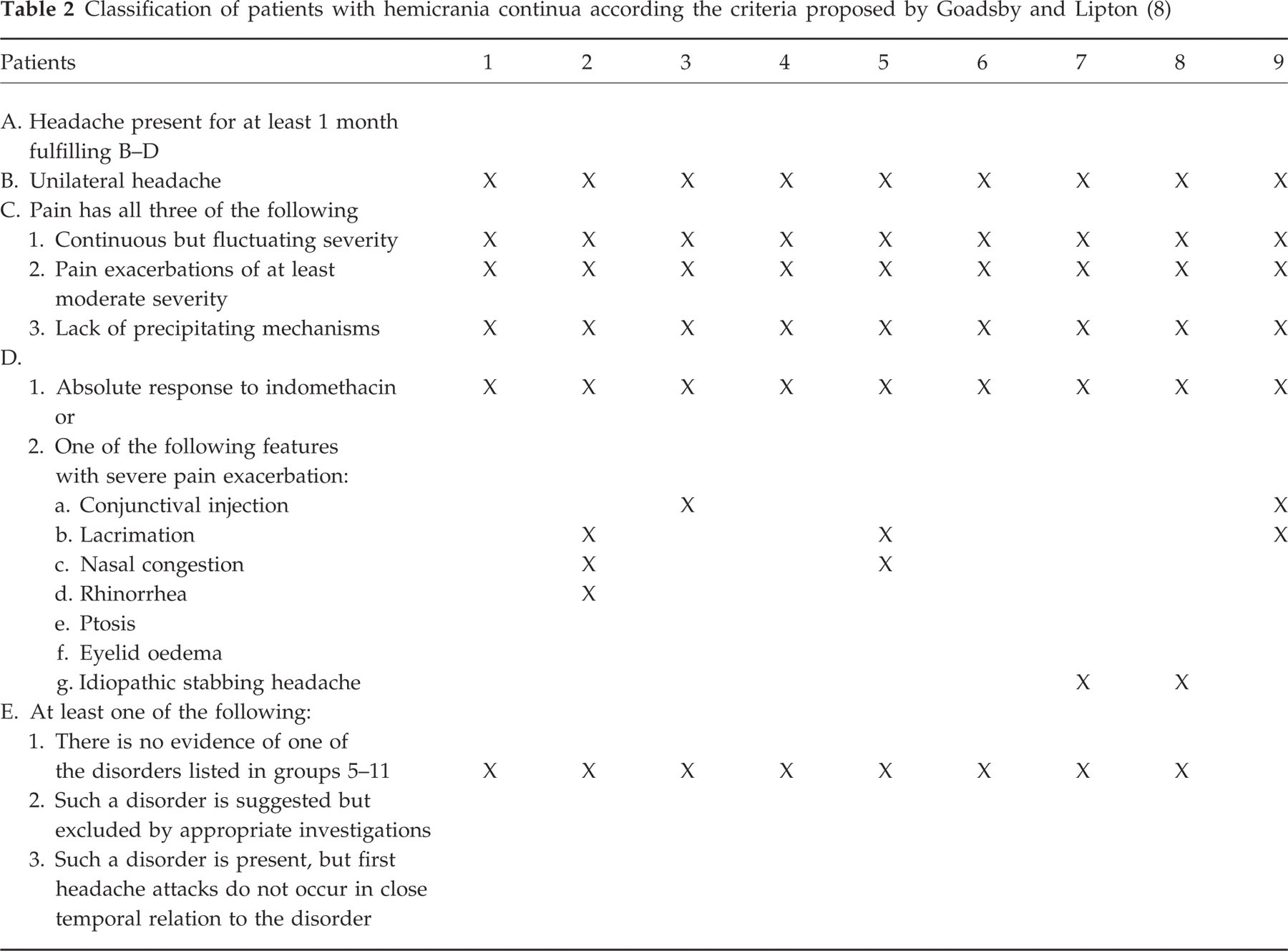
Table 2 displays the diagnoses according to the criteria proposed by Goadsby and Lipton (8). All patients fulfilled criteria B–D, necessary for the diagnosis. As this system does not exclude excruciatingly severe exacerbations, patient 3 also fulfilled the criteria. As all of them had absolute response to indomethacin, all fulfilled criteria D1, six (66.7%) also fulfilling criterion D2.
Discussion
Operational diagnostic criteria for HC were not incorporated into the IHS classification (5), but are expected to appear in the future revision (6). The changes in nosologic status of HC will be of great and immediate interest.
Both current systems allowed the classification of most patients with HC. Important differences, however, do exist between them.
The criteria proposed by Pareja et al. (4) consist of obligatory features, as well as non-obligatory but frequent and negative features. By this system, HC is considered a strictly unilateral headache, without side shift, absolutely responsive to indomethacin, chronic and not excruciatingly painful. Eight of our nine patients fulfilled all these criteria.
Both systems consider some obligatory features, with two main differences: Pareja et al. (4) require: (i) absolute responsiveness to indomethacin; and (ii) the intensity of pain can not be excruciatingly severe.
Some criticism has been raised with regard to the criterion of absolute response to indomethacin, especially considering that a variety of medications have been reported to be effective in patients with HC (9–11). As this criterion does not allow for responsiveness to medications other than indomethacin, this is the main difference between the two systems. According to this classification, indomethacin responsiveness is an essential test, required to make the diagnosis. The patients who do not respond to indomethacin should be classified as hemicrania generic incerti, a clinically similar disorder. In contrast, the criteria proposed by Goadsby and Lipton, addressing patients who do not respond to indomethacin, include all patients under the HC classification. Their classification also emphasizes the clinical features of HC and considers the autonomic symptoms as well.
Pareja et al. require an intensity of pain from mild to severe, but do not permit excruciatingly severe. This seems quite subjective. One of our patients did not fulfil this criterion. In a series of 18 patients with HC, two attempted suicide because of the severity of the headache (3). A patient with a classic picture of HC, as presented by patient number 3, should not be excluded if her subjective experience of pain was reported as very severe (6).
A second and important difference between both systems regards the ‘frequent feature’ and the ‘negative provisos’.
Pareja et al. (4) propose to include the female sex as ‘non-obligatory but frequent characteristic’ of HC. Two of our patients were male and a review of published cases showed a female to male ratio of 2.2 : 1 (6), very similar to the migraine ratio. It does not seem to be reasonable to include this feature, as it is potentially misleading.
Four of our patients presented autonomic features, two had migrainous features and one showed partial response to ergotamine. All these findings are considered as negative criteria (but non-obligatory) according to Pareja et al. (4). Although the intensity of cranial autonomic features associated with HC is less than that seen in chronic paroxysmal hemicrania and cluster headache, their presence in a significant number of patients has been clearly demonstrated (6) and this is probably one of the reasons that led the authors to propose the inclusion of HC within group 3 of the IHS (cluster headache and chronic paroxysmal hemicrania), dealing with other headaches with prominent autonomic features. Similarly, migrainous features occur commonly in this disorder (11) and response to ergotamine has been described (12). These negative provisos are therefore non-discriminative and confusing.
Diagnostic criteria for any disease must be clinically useful, intuitive, comprehensive, reliable and validated. Hierarchical classification is recommended, contrasting with diagnostic overlap. Although it seems logical and intuitive to position the nosologic status of HC under group 3 of the IHS classification, as proposed by Pareja et al., the Goadsby and Lipton classification provides a more sophisticated and clearer approach to HC.