
Abstract
Migraine is a common, disabling form of primary headache that has been linked by functional imaging studies to activation in the rostral brainstem. In specialty clinics migraine is most commonly seen in association with frequent less feature full headache that has been called transformed migraine or more recently termed chronic migraine. A patient is described with frequent migraine, 3 days per week, and less feature full headaches on other days. The patient has a cavernoma in the midbrain that has bled. She was previously headache free and now has contralateral daily headache. The patient supports the functional imaging observations from positron emission tomography (PET) that the rostral brainstem is pivotal in migraine pathophysiology, particularly the contralateral midbrain periaqueductal grey matter. Moreover, the patient's lesion provides biologically plausible support that a single entity causes her clinical presentation: chronic migraine, not two-disorders, migraine and tension-type headache.
Introduction
Migraine is an inherited, episodic disorder of the central nervous system (1) that is both common (2) and, when severe, very disabling (3). Of migraine's clinical features – sensitivity to movement, light (photophobia) and sound (phonophobia) – it is the pain that is best correlated with disability (4). Over much of the last 25 years the basic neuroscience of migraine has focused on cranial vasodilatation as a source of pain (5). Most recently, the mechanisms of peripheral trigeminal activation (6), the localization and physiology of second order trigeminovascular neurones (7) and the mechanisms of cortical spreading depression (8) have been studied in detail. Functional imaging in acute migraine has revealed activation in the rostral brainstem (9, 10) to be pivotal in the pathophysiology of the disorder. Of the clinical presentations of primary headache, the most controversial is that of daily or near daily headache (11) and its relationship to migraine.
While it is not novel to suggest on clinical grounds that migraine can occur on a daily or near daily basis (12), the current International Headache Society (IHS) classification system (13) does not include the concept of chronic migraine. The problem must be addressed as about 1 in 20 patients in North America (14) and western Europe (15) have daily or near daily headache. It has been argued that patients with daily headache have two clinical problems: migraine and tension-type headache. However, emerging evidence, including the epidemiology of daily headache (14), its clinical presentation (11), therapeutic responses (16) and some sharing of neuropeptide markers (17), suggest that migraine can have a frequent form: chronic migraine. A recent clinical case reinforces the emerging consensus that upper brainstem structures are pivotal to migraine. Moreover, the case presented has chronic daily headache of the chronic migraine variety, and provides a plausible biology to perhaps the most pressing current problem in primary headache classification.
Case report
A 45-year-old woman was referred for review of her headache. In 1997 she had a sudden onset of diplopia, which involved the range of movements, and right facial numbness. Both persisted for 3 months. A brain computerized tomography (CT) scan and magnetic resonance imaging (MRI) were performed and a left-sided brainstem vascular malformation was demonstrated, which was considered to have bled (Fig. 1).
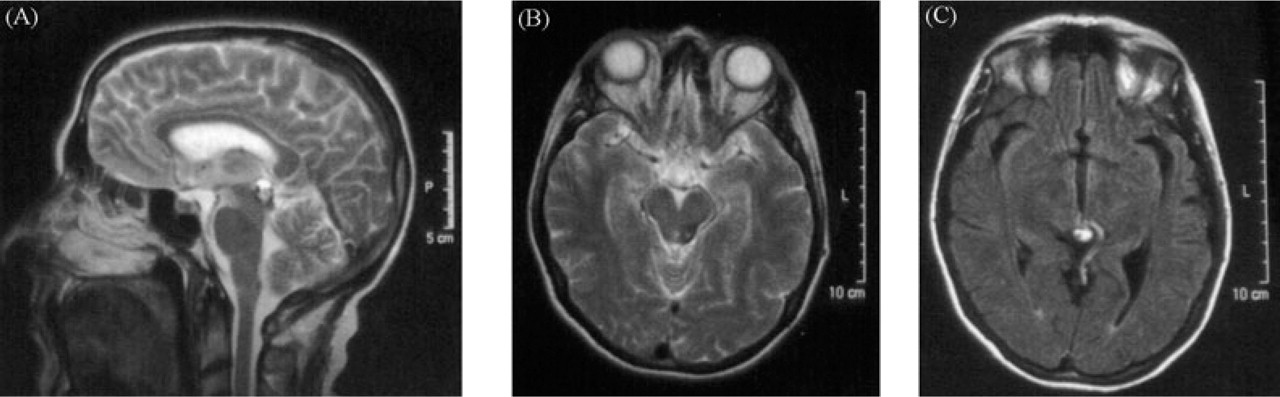
MRI demonstrating a left-sided cavernoma (a and b) with an associated developmental venous anomaly (c) in the dorsal midbrain region adjacent to the periaqueductal grey matter.
From the time of onset of the diplopia the patient reported persistent right-sided temporal headache, contralateral to the MRI lesion. The persistent pain was punctuated two to three times a week by a severe right-sided throbbing headache with some added features of pressure. The more severe headache was associated with nausea, photophobia and phonophobia, as well as aggravation with movement. There were no cranial autonomic features. During the majority of attacks and lasting for most of the attack, but not preceding it, there was right-sided facial numbness that did not move. At varying points in her clinical course she had used both codeine- and paracetamol (acetaminophen)-containing compounds. These were largely unhelpful for the severe pain and their withdrawal did not alter the headache phenotype.
Her past history was remarkable for a mild head injury without loss of consciousness in 1993. She had never been treated with migraine preventatives. She had been otherwise relatively well until initial presentation, with no significant history of headache. She had not considered herself headache prone. She had no typical migraine triggers for her attacks, including no triggering from alcohol consumption. There was no family history of headache.
On examination her cranial nerves were intact, including normal eye movements, with the exception of a right-sided reduction in facial light touch and pin-prick. Her limb examination, co-ordination and gait were normal.
Discussion
The patient essentially presents with episodes of severe right-sided throbbing headache with nausea, photophobia, phonophobia and aggravation with movement that would easily fulfil the IHS criteria for migraine (13). She has a continuous component to the pain, which is rather less feature-full, and would fulfil the criteria for chronic tension-type headache (13). Alternatively, one might simply classify the problem as chronic migraine (11). Remarkably, the patient has a left-sided, contralateral, dorsal midbrain vascular malformation that is likely to have bled at the onset of this problem. Her lesion is in the same region reported to be associated with migraine on positron emission tomography (PET) (9). She could thus be said to have secondary chronic migraine due to the lesion that involves the midbrain periaqueductal grey (PAG) matter. The case provides broad support for the notion that midbrain dysfunction may be important in the basic pathophysiology of migraine. Moreover, the case provides a plausible biological explanation and support for the existence of the clinical syndrome of chronic migraine as a neurobiological entity.
The first evidence in humans to indicate a central source for the pain of migraine arose from the work of Raskin (18), who reported a group of non-migraine patients developing migraine-like headache after implantation of a stimulating electrode into the PAG. These observations were confirmed in a subsequent report of a larger number of patients (19). A plaque of multiple sclerosis in the PAG has also been reported to produce a migraine-like headache (20), adding to the body of evidence that implicates the brainstem, perhaps the PAG specifically, in migraine pathophysiology. The first direct functional evidence of a role for the PAG in migraineurs was provided by the results of a PET study in spontaneous attacks of migraine without aura (9). This is now further supported by observations of excess iron deposition in the PAG in both episodic and chronic migraine (21).
In the PET study patients were studied during the migraine attack and increases in regional blood flow were observed in the cingulate cortex, and the auditory and visual association cortices. In addition, contralateral increases in brainstem blood flow were seen (9). The specific brainstem loci involved could not be resolved with PET but the regions activated were the dorsal midbrain, which would have included the PAG, and the dorsolateral pontine tegmentum, which would have covered the locus coeruleus (22). It is important that after headache relief by pharmacological intervention only the brainstem activation persisted, suggesting more than a reactive-to-pain role in the attack (9, 10). Activation in these brainstem regions seems specific for migraine, given that they have not been observed in experimentally induced facial pain (23), or atypical facial pain (24). Indeed brainstem activation is not observed in acute cluster headache (25), which is a relatively closely related primary neurovascular headache in terms of pain expression (26), nor in SUNCT syndrome (short-lasting unilateral neuralgiform pain with conjunctival injection and tearing) (27). In a recently studied patient with both migraine and cluster headache, a PET scan during a migraine attack, while he was in an active cluster period, demonstrated brainstem activation (10). Taken together the data suggest that brainstem activation is particular to migraine, certainly amongst forms of headache.
The finding of a contralateral lesion here is completely consistent with Weiller and colleagues PET study (9). In an animal study that examined modulatory effects of the PAG on trigeminal neurones activated by stimulation of the superior saggital sinus 74% of the cells received contralateral inhibitory PAG input, whereas 41% received an ipsilateral input (28). These findings contrast with anatomical studies that show that direct projections from the PAG to the spinal cord dorsal horn are predominantly ipsilateral (29). However, other animal studies that demonstrate PAG inhibition also conflict over the ipsilateral vs. contralateral functional preference (30–32). Moreover, it is possible that the innervation is not direct but polysynaptic and involving other brain systems.
An equally plausible hypothesis would be that the pivotal effect of PAG modulation of the trigeminovascular system is ascending at the level of the thalamus (33), as the quintothalamic tract decussates in the brainstem. Such a construction would easily account for the ipsilateral and contralateral head and arm sensitivity that has recently been carefully documented to occur during migraine (34). Centrally mediated pain hypersensitivity is a well-established concept (35) and PAG dysfunction in migraine would explain the clinical observation that abnormal sensation is often reported in non-trigeminal regions of the body (1).
What might be the lesion in migraine, as contrasted with this patient? It has been shown that missense mutations in the gene encoding the α1A subunit of the P/Q type voltage-gated calcium channel (36) account for about 55% of families with familial hemiplegic migraine (37). Injection of agatoxin-IVA, a P/Q channel blocker, into the PAG facilitates responses of trigeminal neurones to stimulation of the superior saggital sinus (38). If an inherited defect in calcium channels were to be manifested in the PAG in humans it would be predicted to facilitate trigeminovascular nociceptive transmission, perhaps resulting in episodic throbbing pain. Moreover, by considering such an increased trigeminovascular activation one could explain the susceptibility of migraineurs to medication misuse headache (39). Patients with migraine have raised inter-ictal calcitonin gene-related peptide (CGRP) levels (40), which is a key marker peptide for migraine and cluster headache (41). It has recently been shown that CGRP facilitates morphine tolerance (42), and CGRP blocker suitable for clinical use is now available (43).
In summary, a case of chronic daily headache of the chronic migraine type is presented in a patient who had a bleed from a vascular malformation in the dorsal midbrain. The lesion is contralateral to the side of pain. The lesion reinforces the view that brainstem, especially periaqueductal grey matter, modulation of trigeminovascular nociception is pivotal in migraine. Moreover, the case provides a plausible neurobiology with which to begin to understand the most disabled of the primary headache sufferers, those with persistent headache and an underlying migrainous diathesis: chronic migraine. Moreover, the case supports the Classification Committee's suggestion to incorporate the concept in the next revision of the IHS criteria (44).
Footnotes
Acknowledgement
Peter Goadsby is a Wellcome Senior Research Fellow.