
Abstract
Platelet 3H ketanserin binding was studied in 33 patients of migraine and 30 healthy controls. The binding characteristics: equilibrium dissociation constant (Kd) and maximal number of binding sites (Bmax) determined by Scatchard analysis revealed a significant decrease in Kd and no change in Bmax in migraine cases. No correlation was observed between the Kd and Bmax with the clinical features of migraine. The findings of the present study show that there is a decreased affinity of platelet 5-HT2 receptors in migraine.
Introduction
The possibility that serotonin (5-hydroxytryptamine, 5-HT) might be an important endogenous factor responsible for the pain of migraine was first proposed by Wolff et al. in the late 1950s (1). Supporting evidence for a role of 5-HT in migraine was provided by changes in circulating levels of 5-HT and its metabolites during the phases of a migraine attack and the ability of serotonin releasing agents to induce migraine like symptoms (2–5). The development of serotonin receptor agonists which are effective in the alleviation of migraine pain further implicated serotonin as a key molecule in migraine (6).
It has been proposed that there is an increase in 5-HT function which leads to activation of 5-HT1C receptors leading to initiation of a migraine attack. The source of this 5-HT that triggers the attack remains to be defined as also the reason for its periodic mobilization (7). 5-HT2B receptors located on the endothelial cells of meningeal blood vessels trigger migraine headache through the formation of nitric oxide. The endothelial 5-HT2B receptor couples to nitric oxide synthases (NOS), promoting the local release of NO. In cerebral vessels NO liberated in this way might be expected to excite and sensitize perivascular trigeminal afferents because NO donors activate trigeminovascular fibres to cause release of sensory neuropeptides (8).
The circulating platelets in the peripheral blood constitute an important dynamic reservoir of 5-HT and are able to rapidly accumulate and secrete serotonin and thus they have aroused considerable interest on their possible involvement in migraine (9, 10). The biogenic amine functions of the platelets closely resemble those of serotonergic neurones (11, 12). As the platelets can be easily obtained by a simple venepuncture so they form a readily available tool to study the various serotonergic mechanisms. The circulating 5-HT stored within the blood platelets can under certain circumstances interact with the different compartments of the vascular wall via serotonergic receptors. The currently accepted classification of 5-HT receptors includes seven classes known as 5-HT1 through 5-HT7 and the class most implicated in migraine is 5-HT1 (which consists of the A, B, D, E, and F subtypes) and 5-HT2B. The most commonly used radioligand for 5-HT2 receptors is 3H-ketanserin which labels both the 5-HT2A and 5-HT2B subtypes (13). A decrease in the [3H] imipramine binding to platelet membrane of patients with classical migraine has been reported (14).
The involvement of 5-HT2 receptors in migraine has been investigated by following the binding of 3H-ketanserin in blood platelets of migraine patients in the present study.
Patients and methods
Thirty-three patients of migraine attending the Headache Clinic in the Neurology Outpatients Department of the King George's Medical College were included. The diagnosis of migraine was based on the criteria given by the International Headache Society (15). A detailed history was taken according to a predesigned proforma and complete physical examination was done. The severity of headache was measured by calculating the Headache Index (Number of attacks per month × Severity of pain × Duration of pain in hours}. The severity of pain in the attacks was graded on a three point scale: 1=Mild headache, does not interfere with the patient's daily routine; 2=Moderate headache, interferes with the daily routine but patient can continue his work; 3=Severe headache, patient has to take bed rest. Thirty healthy controls comprising of paramedical staff and relatives of the patients were also included. The patient characteristics of the subjects included in the study are given in Table 1.
Patient characteristics

None of the subjects included in the study were suffering from hypertension, diabetes mellitus, ischaemic heart disease or any psychiatric illness which may affect 5-HT metabolism. Food items (banana, chocolates, nuts etc.) containing 5-HT were forbidden for at least 14 days and drugs like aspirin, psychotropics, antidepressants were not allowed for at least 7 days prior to collection of blood samples.
Collection of blood samples
Nine ml of blood was collected by venepuncture from the antecubital vein using a disposible plastic syringe with a 20 gauge needle, between 09.00 and 10.00, and immediately transferred to plastic tubes containing one ml of 3.8% sodium citrate. It was transported to the Industrial Toxicological Research Centre within 30 min of collection for biochemical analysis.
Preparation of platelet membrane
The method of Khanna et al. (16) was followed for preparation of platelet rich plasma (PRP) and platelet membrane
Platelet counts
Platelet counts were done in a Naebeur haemocytometer in duplicate. For platelet counts 0.1 ml of PRP was taken out in plastic tubes and added to 1.9 ml of formyl citrate.
Receptor binding assay
Binding assay of 3H-ketanserin to platelet membrane was carried out as described by Oshuka et al. (17). Briefly, binding tubes containing assay buffer (50 m
Assay of protein content
Protein was determined following the method of Lowry et al. (18) using bovine serum albumin as reference standard.
Chemicals and source
3H-ketanserin (61.5 Ci/mmole) and cinanserin were procured from M/s NEN, USA and M/s RBI, USA. All other chemicals used in the assay were of analytical grade and obtained from the local source.
Data analysis
The data were analysed by the method of Scatchard (19), plotting bound/free (B/F) vs. bound (B) and finally analysed by the non linear regression analysis and the equilibrium dissociation constant (Kd) and the maximal number of binding sites (Bmax) were obtained. The values of Kd and Bmax are expressed as mean±SEM.
Statistical analysis
The student's t-test was used to compare the mean values between migraine and controls. A univariate analysis of the various clinical features with the binding characteristics (Kd, Bmax) was done. The value of correlation coefficient (r) was also calculated for the binding characteristics with age, duration of disease, time since last attack and severity of headache (determined by headache index). A P-value less than 0.05 was considered significant.
Results
The platelet count in PRP in migraine (2.74 ± 0.04 cells/108 mm3) and controls (2.75 ± 0.04 cells/108 mm3) did not show any significant difference. The binding data of 5-HT2A receptors in control group was analysed with respect to sex and age. There was no significant change both in the Kd and Bmax between males (Kd 1.61 ± 0.21 n

Scattergram showing the binding characteristics, (a) Kd and (b) Bmax of 3H-ketanserin to platelet membrane in migraine (•) and controls (○). A significant increase was observed in the Kd in migraineurs (P < 0.05).
Correlation coefficient of platelet 3H-ketanserin binding with various clinical features of migraine
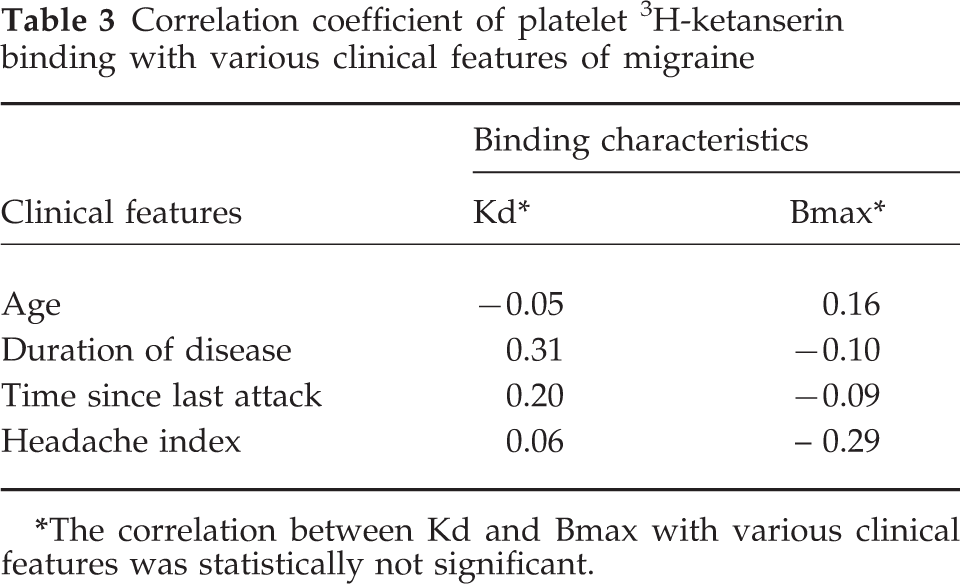
The correlation between Kd and Bmax with various clinical features was statistically not significant.
Univariate analysis of platelet 3H-ketanserin binding in relation to various clinical features of migraine

Values are Mean±SEM;
The P-value for Kd and Bmax in various subgroups are statistically not significant.
Discussion
Recent advances in the receptor biochemistry of serotonin have given important insight into the mechanisms of migraine pain and treatment. Neurogenic inflammation resulting from antidromic stimulation of trigeminal fibres has been proposed as a possible pathogenetic mechanism for migraine. The neurogenic anti-inflammatory activity is mediated by activation of 5-HT auto-receptors present in sensory fibres innervating blood vessels in dura mater (20). Experimental observations have shown that 5-HT inhibits evoked trigeminal nucleus firing via the 5-HT1B/1D receptor (21).
The present findings of a significant decrease in the equilibrium constant (Kd) in migraine cases without any change in the maximal number of binding sites (Bmax) is in contrast to the two previous reports of decreased Bmax in migraine (22, 23) The reasons for this difference could be the time of sampling after the migraine attack or the radioligand used. In the present study 3H-ketanserin (which is more specific for labelling 5-HT2A receptors) was used as compared to the earlier studies in which 3H-spiperone was used. The decrease in Kd did not have any significant correlation with the clinical features of migraine like age, duration of disease, time since last attack and severity of disease as determined by headache index. The reported decrease of platelet serotonin receptors in patients with migraine could be due to an autoimmune reaction, however, no statistically significant differences were found in the frequency of platelet antibodies of known or unknown specificity in patients with migraine with/without aura as compared to controls (24).
A reduced 5-HT uptake has been reported in platelets obtained from migraine subjects during and within 5 days of migraine attack (25). This reduced uptake could be due to either a decrease in number of receptors or the affinity of the 5-HT receptors. The findings of the present study provide supportive evidence for the second mechanism. An earlier study has reported that the Michaelis Menten constant (Km) was significantly increased, as compared with control subjects, in attack free patients of migraine without aura and tension headache but not in those suffering from migraine with aura (26). This finding was independent of age, sex, presence of anxiety or depression and drug intake during the previous week. The difference however, appeared greater in the morning than in the afternoon. It was concluded that the 5-HT uptake sites of platelets of patients having migraine without aura or with tension headache have reduced affinity for 5-HT.
A progressive increase in 5-HT expression on monocytes has been demonstrated during headache induced by isosorbide dinitrate in patients of migraine without aura before and after administration of sumatriptan. This increase may be due to the activation of 5-HT turnover and to the increased availability of 5-HT displaced by sumatriptan from cerebrovascular receptors during head pain (27). 5-HT2 binding sites are highly concentrated in the middle layers of frontal cortex and are bound avidly to methysergide, pizotifen and cyproheptadine (28). However, measurement of the brain radioactivity, by positron emission tomography, after intravenous injection of 18F-fluorosetoperone (a 5-HT2 specific radioligand) has demonstrated no change in the age adjusted specific distribution volumes of the ligand in migraineurs as compared to controls (29). Alteration of serotonin receptor function is one of the possible mechanisms of analgesic induced headache (AIH). A greater density of receptor number has been reported in patients with AIH and control as compared to migraine patients while the Kd was unchanged. Thus up-regulation of 5-HT2 serotonin receptor may be a possible mechanism of headache transformation in patients with AIH (30). The up-regulation of serotonin receptors observed in patients of chronic daily headache (so called transformed migraine) provides support to the serotonergic hypofunction ‘theory of migraine pathogenesis’ and may explain the unusual loss of episodicity seen in the transformed migraine patients. Further suppression of an already abnormal antinociceptive system with up-regulation of post synaptic receptors is one of the explanations of transformation of episodic migraine to chronic daily headache (31). The decrease in 5-HT2 receptors that occurs with ageing may account for the tendency of migraine to improve or disappear with increasing age (32).
In terms of migraine pathogenesis, the evidence regarding involvement of serotonin receptors remains ambiguous. On the one hand there is a long standing implied role for serotonin mobilization and depletion during a migraine attack, suggesting that a tonic activation of serotonin receptors is in some way crucial to a normal modulation of cranial nociception. On the other hand, drugs that activate specific serotonin receptor subtypes are clearly effective in the symptomatic treatment of an attack of migraine. Many of the most effective prophylactic drugs, including propranolol, block 5-HT2B receptors with a potency that matches the drug dose. Furthermore the functional affinity of serotonin for this receptor subtype is high, so that activation can be anticipated at serotonin concentrations as low as 1 nmole/l (33). Perhaps such a dichotomy is not unreasonable given that as many as 14 distinct 5-HT receptors have now been identified. Although understandably circumstantial, this body of accumulated information continues to encourage the view that serotonin and serotonin receptors are somehow implicated in migraine pathogenesis (7). One theoretical model envisages 5-HT as a link between the neural and vascular systems, with global alteration of serotonergic neurotransmission affecting not only these systems, but the gastrointestinal tract as well, with incidental reverberations on platelet function. Such altered serotonergic transmission might originate from altered 5-HT receptor dynamics, a molecular change in turn produced by genetic mechanisms.
The findings of the present study suggest alteration of platelet 5-HT2 receptors in the cases of migraine and further strengthen the usefulness of platelets as a peripheral model. However, further experiments along these lines, correlating the levels of 5-HT and its metabolites in platelets and plasma with the alterations of the affinity of receptors at the precise stages of the disease are still required.
Footnotes
Acknowledgements
This multicentre study was supported by a grant from the Department of Biotechnology, New Delhi, India.