
Abstract
Chronic daily headache (CDH) represents a group of non-paroxysmal headache disorders that occur on a daily or near-daily basis, for longer than 6 months. Even though it is a common problem, affecting 30–70% of the patients attending specialized headache clinics, it is not a well-defined and classified disorder, resulting in controversies regarding its description and approach. The aim of this study was to evaluate the clinical presentation of CDH due to transformed migraine and possibly compare the differences among male and female patients. Two hundred and seventy-one patients, 217 women and 54 men, ages 16–83 (mean 37.5 years for women and 41.4 for men), fulfilling the proposed criteria for transformed migraine and selected from a group of 300 consecutive CDH patients attending a subspecialty headache centre, were studied retrospectively. The most observed clinical presentation was pressure or tightening, bilateral fronto-temporal, moderate non-continuous headache, with a progressive onset. The association with nausea and phonophobia was demonstrated in 60% and 32% of the patients, respectively. The association with photophobia (29.6% male, 44.2% female, P = 0.05) sleep (77.7% male, 49.8% female, P = 0.0002) and emotional (87% male, 64.1% female, P = 0.001) disturbances, as well as the occurrence of intermittent full-blown migraine attacks (81.5% male, 95.4% female, P = 0.001) was significantly different among male and female patients. Overuse of symptomatic medications (SM) was observed in 87% of the male and in 83.8% of the female patients, with a significant difference concerning the use of more than one type of SM (male 68% compared with female 91.7%; P = 0.006). We concluded that TM patients have a clinical presentation compatible with previous descriptions but suggesting, even though limited by the restricted number of male patients, different aspects among male and female patients.
Introduction
Chronic daily headache refers to a group of non-paroxysmal headaches, including those associated with overuse of symptomatic medications, that present on a daily or near-daily basis, with a duration greater than 4 h a day and lasting longer than 6 months (1, 2, 3).
Its prevalence in the general population varies from 0.5 to 6% (4, 5), affecting more women than men (6) and representing 40% or more of all patients attending specialized headache clinics (7). Even though it is a frequent disorder, its systematic study is recent and the lack of well-defined diagnostic criteria has been generating controversies with regard to its presence in the current IHS classification (2, 4).
Most patients with CDH have had episodic migraine in the past, and with the time, revealed a progressive modification or loss of specific migraine characteristics, therefore presenting with a daily or near-daily headache, with mixed clinical features of migraine and tension-type headache (3, 8). This daily or near-daily headache, evolving from episodic migraine and presenting clinical features of migraine and tension-type headache, has been called transformed migraine (1, 2, 8, 9). These patients commonly present with episodic migraine that started in the second or third decades, and at around 30–40 years of age the headaches become progressively more frequent with the typical migraine features of nausea, vomiting, photophobia, phonophobia and osmophobia occurring less and/or with less intensity (1, 6). Some patients start with episodic migraine with aura and transform into migraine without aura and daily headache occur subsequently (6, 8). Other migraine characteristics such as menstrual aggravation, identifiable migraine triggers and unilateral headache may be present (8). Most of these patients present with a positive family history for migraine and have intermittent typical migraine attacks, of greater severity than the daily headache (6, 8).
The patients with TM frequently overuse symptomatic medications and present sleep and psychological disturbances that may contribute to the development or perpetuation of the chronic daily headache syndrome (3, 4, 6, 8).
The objectives of this study were to describe the clinical presentation of CDH patients due to transformed migraine and compare the features presented by male and female patients.
Materials and methods
During the period from January 1996 to January 1998, 300 consecutive chronic daily headache patients attending a private subspecialty headache centre were studied retrospectively. Among them, 271 patients, 217 women and 54 men, ages 16–83 years (mean 37.5 years for women and 41.4 years for men) fulfilled the proposed criteria for TM (1, 2), 26 patients, 16 women and 11 men, fulfilled the proposed criteria for chronic tension-type headache (1, 2) (CTTC) and three male patients fulfilled the proposed criteria for new daily persistent headache (1, 2) (NDPH). Only patients with headache for more than 6 days a week of greater than 6 months duration were included. All patients were evaluated by the first author in initial consultations not shorter than 1 hour and answered a questionnaire with details concerning the headache initiation, evolution and characteristics, as well as factors involved in its worsening, progression and their habits of symptomatic medication consumption. All the patients included in this study had normal physical and neurological examinations and no diagnostic studies were necessary. The data obtained were submitted to statistical analysis utilizing tables, frequency distribution, standard deviations and non-parametric chi-square tests, comparing the male and female patient's presentation. The significance level considered for this study was P < or = 0.05. The criteria used to define symptomatic medication overuse were the consumption of at least one of the following for at least 1 month, as proposed by Silberstein et al.: (i) simple analgesic use (> 1000 mg ASA/acetaminophen) > 5 days/week; (ii) combination analgesics (caffeine, barbiturate-containing medications) (> 3 tablets/day) > 3 days/week; (iii) narcotics (> 1 tablet/day) > 2 days/week; and (iv) ergotamine use (1 mg PO or 0.5 mg PR) > 2 days/week.
Results
Among the TM patients, the chronology of the primary and the daily headache evolution as well as the perception of frequency increase among female and male patients are listed in Tables 1, 2 and 3.
Transformed migraine (TM)—female patients

Transformed migraine (TM)—male patients

Distribution of frequencies and percentages related to the temporal characteristics of migraine patients evolution

The characteristics of the headache itself are described as follows. With regard to the headache location, the patients reported the following sites: bilateral fronto-temporal (n = 118, 54.3% among the women and n = 28, 51.8% among the men); diffuse (n = 62, 28.5% of women and n = 11, 20.3% of men); alternating hemicranial pain (n = 12, 5.5% of women and n = 7, 12% of men) and unilateral fronto-temporal alternating sides (n = 25, 11.5% among the women and n = 8, 14.8% among the men) (P = 0.11) (Table 4).
Distribution of frequencies and percentages related to the clinical characteristics of transformed migraine patients (TM)

The severity of the headache was described as: mild (n = 55, 25.3% of the women and n = 20, 37% of the men), moderate (n = 115, 53% of the women and n = 22, 40.7% of the men) and moderate to severe or severe (n = 47, 21.6% of the women and n = 12, 22% of the men) (P = 0.18) (Table 4).
Regarding the headache quality, the patients reported: dull or pressure (n = 158, 72.8% of the women and n = 32, 59.2% of the men), pulsatile (n = 44, 20.2% of the women and n = 17, 31.5% of the men), pressure and pulsatile (n = 8, 3.7% of the women and n = 3, 5.5% of the men) and burning (n = 7, 3.2% of the women and n = 2, 3.7% of the men) (P = 0.26) (Table 4).
The initiation and progression of the headache attack among those patients with non-continuous pain (considering continuous pain the absence of a headache-free interval longer than 1 h each 24 h) and the duration of pain on a daily basis are also shown in Table 4.
The relationship between the headache and sleep was described in two ways: being present upon waking up in the morning (n = 38, 17.5% among female patients and n = 11, 20.3% among male patients) (P = 0.64) and interrupting sleep during the night (not having been asked the time of occurrence) (n = 151, 69.5% female and n = 8, 14.8% male patients) (P = 0.0001) (Table 5).
Distribution of frequencies and percentages of the relationship between transformed migraine patients (TM) and sleep

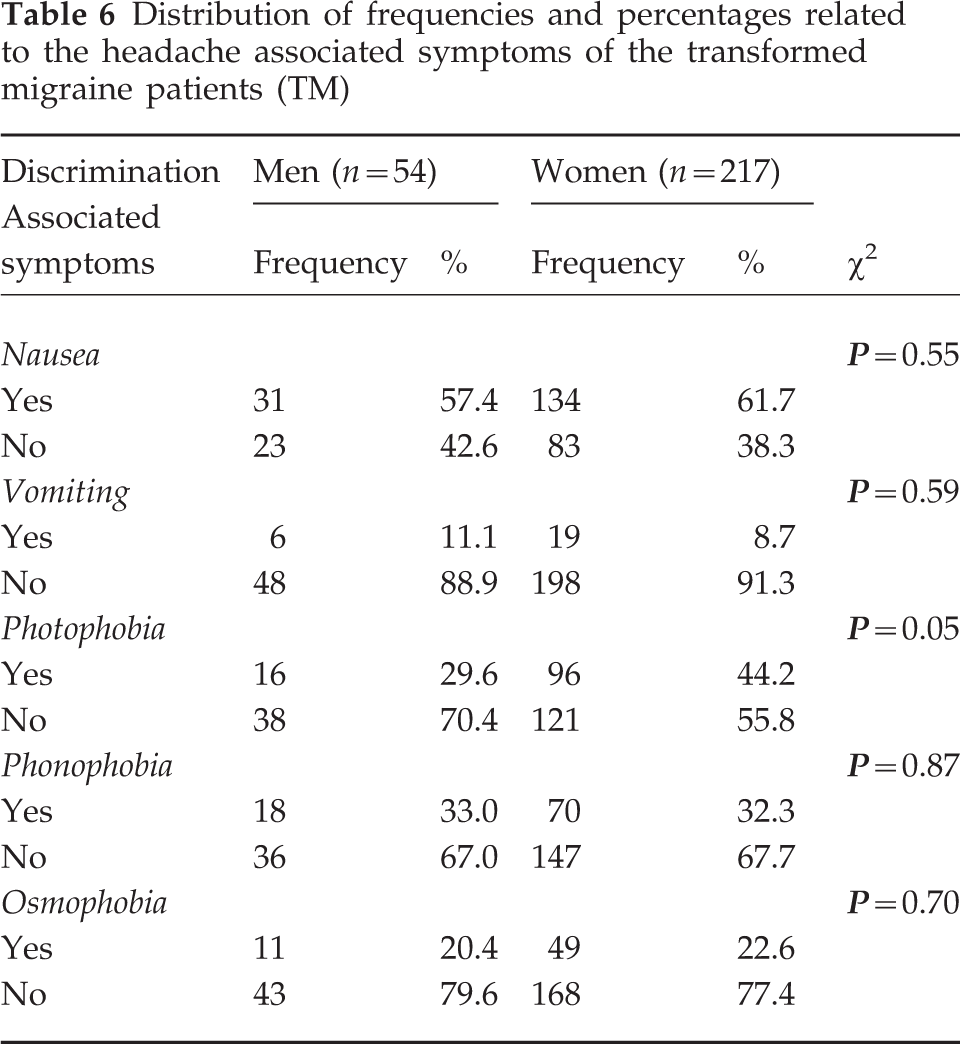
Headache-associated symptoms reported by the patients were: nausea (n = 134, 61.7% of the women and n = 31, 57.4% of the men) (P = 0.55), vomiting (n = 19, 8.7% and n = 6, 11.1%) (P = 0.59), photophobia (n = 96, 44.2% and n = 16, 29.6%) (P = 0.05), phonophobia (n = 70, 32.3% and n = 18, 33%) (P = 0.87) and osmophobia (n = 49, 22.6% and n = 11, 20.4%) (P = 0.70) (Table 6).
Distribution of frequencies and percentages related to the headache associated symptoms of the transformed migraine patients (TM)
The occurrence of sleep disturbances, considered when the patients reported frequent insomnia and/or interrupted sleep, was present in 108 female patients (49.8%) and in 42 male patients (77.7%) (P = 0.0002) (Table 7).
Distribution of frequencies and percentages related to the presence of sleep and emotional disturbances of transformed migraine patients (TM)

Emotional disturbances were considered when the patients answered yes to the following question: ‘Do you feel depression, anxiety or nervousness [being explained the meaning of these words] frequently in your life?’ The answer was yes in 139 female patients (64.1%) and in 47 male patients (87%) (P = 0.001) (Table 7).
Full-blown intermittent migraine attacks were observed in 95.4% (n = 207) of the female patients and in 81.5% (n = 44) of the male patients (P = 0.001) (Table 8). The clinical features, frequency and duration of the intermittent attacks are listed in Tables 9 and 10.
Distribution of frequency and percentages related to the presence of intermittent attacks with typical migraine features in patients with TM

Distribution of frequency and percentages related to the features of intermittent attacks with typical migraine features in patients with TM

Distribution of frequency and percentages related to the frequency and duration of intermittent attacks with typical migraine features in patients with TM

Regarding the trigger factors of the intermittent migraine attacks, the patients reported: menstruation (n = 128, 61.8%), alcohol (n = 23, 11.1% female patients and n = 7, 15.9% male patients), chocolate (n = 27, 13% and n = 3, 6.8%), fatigue (n = 65, 31.4% and n = 10, 22.7%), sleeping longer than usual (n = 38, 18.4% and n = 6, 13.6%), sleep deprivation (n = 96, 46.4% and n = 23, 52.3%), fasting or skipping a meal (n = 100, 48.3% and n = 18, 41%) and stressful events (n = 164, 79.2% and n = 32, 73%). It has to be emphasized that 186 female patients (89.8%) and 39 male patients (88.6%) reported more than one trigger factor.
The excessive consumption of symptomatic medications (SM), according to the criteria proposed by Silberstein et al. (1), was observed in 182 female patients (83.8%) and in 47 male patients (87%) (P = 0.68) (Table 11). Among the female patients, 167 (91.7%) used more than one kind of SM while among the male patients, it was observed in 32 (68%) (P = 0.006) (Table 11).
Distribution of frequency and percentages related to the consumption of symptomatic medications (SM) in patients with TM

Criteria proposed by Silberstein et al. (1994) (1).
Discussion
The scope of this study was to analyse the clinical presentation of TM patients and not to compare it with the presentation of other groups of CDH. However, as a curiosity, the majority of the 26 CTTH patients also presented fronto-temporal bilateral (16 patients) non continuous pressure-type (21 patients) headache. The striking difference refers to the absence of intermittent typical migraine attacks and associated symptoms (with the exception of photophobia presented by two female patients and phonophobia presented by three female and one male patient).
The most observed headache location among the TM patients was bilateral and fronto-temporal, both in female and male patients. Solomon et al. (3) and Spierings et al. (4) observed similar findings, describing 50% of their series as presenting with bilateral headache. However, Mathew et al. (9) found unilateral headache in 58% of his patients, not emphasizing differences between males and females. This discrepancy between Mathew's and our findings may have been due to the fact that patients usually refer to the characteristics of their most intense headache, which is generally presented during the intermittent migraine attacks that may assume a unilateral location. The headache intensity was predominantly mild or moderate, similar to the observations of Solomon et al. (3) who described mild to moderate headache in 88% of his patients. Dull or pressure-type headache was the main characteristic in 72.8% of the female patients and in 59.2% of male patients (P = 0.26), again similar to the findings of Solomon et al. (3), who demonstrated the same feature in 87% of their series.
The duration of the daily headache was continuous for 21.7% of the women and for 25.9% of the men, which is different from the findings of Srikiatkhachorn & Phanthumchinda (10) that observed continuous headache in 46.7% of their patients. We might speculate that this difference may be due to the fact that most of our patients were overusing SM and therefore obtaining headache relief during part of the day.
An interesting point noticed in our series, was the fact that most of the non-continuous headache patients (n = 170, 78.3% of the females and n = 40, 74.1% of the males) presented a progressive onset of their daily headache, which may be justified by the wearing off of the symptomatic medications excessively consumed by most of our patients (83.8% of women and 88% of men), as described by Rapoport (11).
With regard to sleep, there were significant differences between female and male patients. While the majority of patients did not awaken in the morning with headache, 69.5% (n = 151) of the female patients and 14.8% (n = 8) of the males (P = 0.0001) had frequent awakening during the night with headache. Mathew et al. (12) described similar behaviour among 46% of 200 patients studied, even though he didn't differentiate male and female patients. Spierings et al. (4) demonstrated different numbers, with 79% of his patients having headache in the morning, but he also included patients with headache onset during the morning, possibly justifying this way, the differences between his and our percentages. In 36% of his series, patients were awakened during the night with headache at least once a week.
The presence of insomnia and/or interrupted sleep in CDH patients was noted by Mathew et al. (12) in 71% of his patients. It was also observed in our patients but with different figures regarding male and female. While 49.8% (n = 108) of our women patients had it, 77.7% (n = 42) (P = 0.0002) of the men did, which is a significant difference not cited by other authors.
The associated symptoms were described as nausea, vomiting, photophobia, phonophobia and osmophobia (intolerance to strong smells). In the present study female and male patients presented a significant difference with regard to the occurrence of photophobia (n = 96, 44.2% women and n = 16, 29.6% men) (P = 0.05). Nausea was present in 60% of the patients, vomiting in 10%, phonophobia in 33% and osmophobia in approximately 21% of the patients considering both males and females. These numbers are different from those of Solomon et al. (3) who reported nausea in 24%, photophobia in 37%, phonophobia in 42% and osmophobia in 24% of their patients, and from those encountered by Srikiatkhachorn & Phanthumchinda (10) who described the presence of photophobia in 70%, phonophobia in 56.7% and nausea in 43.3% of their patients. Again, we may postulate that such a difference might be due to the fact that patients tend to report the associated symptoms of their severe attacks rather than the characteristics of the daily and not so intense headache. None of these authors mentioned differences between male and female patients.
One might raise the important question of the percentage of patients that persisted with the same features when the headache became daily and determine whether some migrainous symptoms were lost or retained as the frequency of attacks increased. This aspect may be required as crucial by some researchers to differentiate the real TM group or simply chronic tension-type headache+migraine patients, but it has to be emphasized that we strictly used, as inclusion criteria, the proposal of Silberstein et al. (2) that required the history of episodic migraine and/or increasing frequency with decreasing migraine features over at least 3 months and/or current headache meeting IHS criteria for migraine other than duration, despite the fact that there is criticism with regard to the validity of such criteria (13).
Emotional disturbances such as anxiety, depression and nervousness occurring frequently in the patients' lives were reported by more male than female patients (n = 47, 87% male and n = 139, 64.1% female, P = 0001). These findings are similar to those of Solomon et al. (3) that observed depression in 39%, anxiety in 36% and nervousness in 35% of their patients, and to those of Mathew et al. (9, 12) who observed emotional disturbances and altered psychological tests in 61% of their patients, even though none of these authors compared male and female patients. A possible explanation for such unexpected male predominance of emotional disturbances in our study, is the fact that in Brazil, men culturally have the responsibility of supporting their families, which has been deeply impaired and frustrating by the economic circumstances.
Episodic superimposed bouts of full-blown migraine occur in transformed migraine patients (9, 14). In our study they did so in a majority of the patients with a significant predominance in female patients (n = 207, 95.4% women and n = 44, 81.5% men, P = 0.001), which was not mentioned by other authors and may be speculated as being caused by the women's oestrogen monthly oscillations representing a strong trigger factor. With regard to the characteristics of these intermittent attacks, male and female patients revealed different clinical presentations. More male patients presented intense and pulsatile headache (23.2% women and 63.6% men, P < 0.001) and more female patients presented with unilateral headache with associated symptoms (17.4% women and 6.8% men, P < 0.008). Spierings et al. (4) observed that 94% of their patients reported attacks of severe head pain superimposed on the daily headache presenting as unilateral in 43% of their patients, which is different from our findings that revealed this feature in 50.8% of the females and 70.4% of the males. These authors and others consulted made no comments concerning differences among male and female patients.
Trigger factors of the intermittent attacks were clearly identified in our patients. Stressful events were pointed to by 79.2% of the women and by 73% of the men; menstruation by 61.8% of the women; sleep deprivation by 46.4% of the women and by 52.3% of the men; missing a meal by 48.3% of the women and by 41% of the men; fatigue by 31.4% of the women and by 22.7% of the men; alcohol by 11.1% of the women and by 15.9% of the women; and the ingestion of specific foods such as chocolate by 13% of the women and by 6.8% of the men. Mathew et al. (9) observed that 88% of their patients reported trigger factors for severe attacks. Spierings et al. (4) reported different numbers. These authors revealed menstruation as a trigger factor for 28% of the women, stressful events in 29%, alcohol in 20% and sleep deprivation in 12%. The numbers encountered by Srikiatkhachorn & Phanthumchinda (10) were 56.7% for stressful events, 13.7% for menstruation, 11.7% for sleep deprivation and 3.3% for alcohol ingestion.
The overuse of SM was demonstrated in 83.8% (n = 182) of the female patients and 87% (n = 47) of the male patients (P = 0.68). These numbers are higher than those observed by Mathew et al. (15), who reported overuse of SM in 52.4% of their patients, but similar to the number (87.2%) they observed in 1987 with more patients (9). Solomon et al. (3) also reported excessive use of SM in 47% of their patients, while Srikiatkhachorn & Phanthumchinda (10) observed it in 58.3% of their patients. On the other hand, Castillo et al. (16) encountered excessive use of SM in 31.1% of their patients with TM, emphasizing the differences found in populations of headache clinics and of patients with CDH not under treatment in specialized centres. The overuse of SM has been also reported by Sandrini et al. (17), Manzoni et al. (18) and Mathew (19), who observed numbers varying from 24% to 76.1%. The different findings of these authors and our patients may be due to the specific sample of patients we studied, mostly ‘end-of-line’ headache patients, who have seen numerous doctors and treatments, with a sometimes progressive overuse of symptomatic medications.
However, there was a significant difference with regard to the consumption of more than one type of SM (n = 167, 91.7% women and n = 32, 68% men, P = 0.006) which may be related to different resistance to pain among genders and was not found in citations of other authors.
The mechanisms by which the transformation into daily headache occurred in our patients were not intended to be addressed in this study but since the majority of our patients were overusing SM and had emotional disturbances, it may have represented important factors, as already suggested (14, 15).
Conclusions
The clinical characteristics of TM are similar in some aspects to that of the chronic tension-type headache. Steady, moderate, bilateral pressure-type fronto-temporal headache, with mild associated symptoms such as nausea and/or photophobia, phonophobia and osmophobia with duration longer than 4 h a day was the most frequent presentation. There were differences concerning headache features and association with sleep and emotional disturbances among male and female patients, even though it has to be seen with caution since females clearly outweighed males, therefore impairing valid claims despite the fact that it was considered during the statistical analysis. Female patients presented significantly more photophobia and less sleep (insomnia and/or interrupted sleep) and emotional disturbances (anxiety and/or depression and/or nervousness) than male patients. Among these patients, the occurrence of intermittent attacks with typical migraine features was common and significantly more prevalent in women than men. The presentation of those attacks was varied and revealed different patterns among male and female patients. The overuse of SM was frequent among TM patients. However, male and female patients were significantly different with regard to the consumption of more than one kind of such medications. At this point we can only speculate about the significance of these possible differences among genders and further studies analysing the importance, among male and female migraine patients, of the mechanisms involved in such transformation are necessary to clarify these observations.