
Abstract
Objective of the investigation: In a 6-month prospective study of 141 consecutive acute whiplash-injured participants, and 40 acute, ankle-injured controls, pain and tenderness in the neck/head, and at a distant control site, were measured.
Basic procedures: Muscle palpation and pressure algometry in five head/neck muscle-pairs were performed after 1 week and 1, 3 and 6 months after injury. Algometry was performed at a distant control site.
Main findings: Whiplash-injured patients had lowered pressure-pain-detection thresholds and higher palpation-score initially in the neck/head, but the groups were similar after 6 months, and the control site was not sensitized.
Principal conclusion: Focal, but not generalized, sensitization to musculoskeletal structure is present until 3 months, but not 6 months, after whiplash injury, and probably does not play a major role in the development of late whiplash syndrome. Pressure algometry and palpation are useful clinical tools in the evaluation of neck and jaw pain in acute whiplash injury.
Introduction
Subjects exposed to a whiplash injury of the neck may develop a chronic pain condition (a so-called late whiplash syndrome) without detectable, pathological lesions at physical examination or using imaging techniques, such as X-ray, CT or MRI scan (1–4). The incidence rates of whiplash injury differ considerably amongst various countries, and even amongst regions in countries. In Canada, for example, Quebec had 70 compensated whiplash insurance claims per 100000 inhabitants in 1987 (no-fault system: person receives immediately after injury an amount of money for pain and suffering), whereas Saskatchewan (tort system: person can sue for pain and suffering) had 700 compensated claims in the same time-span (5). The no-fault system seems superior to the tort system as shown in a large study from Saskatchewan, changing from tort system to no-fault system in 1995 with subsequent decline in whiplash incidence rate and reduced pain and other symptoms after injury (6). A Dutch study finds a 10-fold increase during a 25-year period of neck sprain following car collision (7) from 3.4 in 1970 to 40.2/100000 in 1994.
An unknown proportion of whiplash-injured people will develop late whiplash syndrome. The proportion with chronic symptoms is reported differently in various prospective studies. In a questionnaire-based study from Lithuania, none of 201 whiplash-injured subjects became chronic whiplash patients, and all recovered from symptoms, including neck pain and headache, within the first 20 days (8). In contrast, a UK study reported that 76% of 50 whiplash-injured patients took legal action after 2 years (9), and 70% of 40 available from the cohort complained of symptoms related to whiplash injury 15 years later (10).
Neck pain and headache are more consistently reported symptoms in both early and late whiplash injury. Recent prospective whiplash studies from Switzerland and Sweden have shown a high frequency of neck pain after acute whiplash injury. Immediately after injury, neck pain occurs in 90% of whiplash-injured patients (11–13), and 2 years after injury, neck pain is present in 20–25% of subjects. The Swiss study finds that initial high pain intensity predicts a bad outcome, and the prognosis is worsened when the subject has pre-traumatic neck pain, tension type headache or migraine (13–15).
While pain and strain of soft-tissue of the neck have been proposed as causative factors for the immediate pain, the mechanisms underlying the more prolonged pain complaints are less clear. An extensive literature has provided evidence for sensitization of the nervous system, and for the development and persistence of experimental and clinical musculoskeletal pains (16). One aspect of such hyperexcitability is a lowering of thresholds to pain following different stimuli. For example, subjects with chronic tension-type headache, fibromyalgia and rheumatoid arthritis display a lowering of pressure-pain-detection thresholds (17–21), and one study has demonstrated hypersensitivity in chronic whiplash patients (22). Palpometry (23, 24) and pressure algometry are simple methods for assessing tenderness and pain from deep structures.
To our knowledge, pressure algometry has not previously been used in assessment of muscle pain in a longitudinal study of acute whiplash-injured persons. In the present study, we tested the hypothesis that soft tissue injury due to a whiplash injury sensitizes nociceptors, and that this sensitization may involve peripheral as well as central mechanisms. The hypothesis of sensitization in deep structures in subjects exposed to whiplash injury was tested by means of pain assessment in the neck and jaw muscles, and at a distant control site in acute whiplash-injured patients compared with acute ankle-distortion subjects. Both groups were expected to have initial pain, but of different origin.
Methods
Patient flow, age- and sex-matching have been described previously (25).
From January 1997 to January 1998, all whiplash-exposed persons in the Aarhus area, covering 284000 inhabitants, were invited to participate, if they met following criteria:
had been exposed to a rear-end car collision;
had preserved full consciousness during collision;
had shown no sign of amnesia after the injury;
had contacted the local emergency unit within 48 h after collision with whiplash-related complaints, such as neck pain, headache and neck stiffness at the unit; and
were aged between 18 and 70 years.
Exclusion criteria were the following:
previously known considerable neck or back disorder or head injury complaints;
previously known severe headache, migraine or widespread pain;
previously known record of severe, psychiatric disease; and
previously known abuse of drugs or alcohol.
Approval from the local ethical committee was obtained, and the study was conducted in accordance with the Helsinki II declaration. Subjects and control subjects gave informed written consent at their first visit.
The control group consisted of persons sustaining acute non-sport, ankle distortion, where X-ray had ruled out fracture, and who otherwise fulfilled the same criteria as whiplash-injured subjects. One hundred and twenty-one consecutive ankle distortion subjects seen at the Emergency Unit of the Department of Orthopaedic Surgery, Aarhus University Hospital, constituted a possible control sample. From this group 40 age- and sex-matched subjects gave their consent to participate.
Selecting a control group with another acute traumatic pain condition allowed us to balance the design of the study, regarding possible influence of post-traumatic stress on pain.
At all visits, participants underwent semistructured interviews, the McGill Pain Questionnaire, and data considering medical/physical/pharmacological treatment, as well as other treatment not subscribed by medical doctors, were obtained. Whiplash-injured patients and controls rated their pain in the neck, head, shoulder/arm and low back with a visual analogue scale (VAS0−100) with 0 = no pain and 100=worst imaginable pain. All measurements were carried out by the same examiner (HK) in a quiet room at room temperature with the subject comfortably seated in a supine position. Deep pain was measured by means of a pressure algometer (SOMEDIC AB, Algometer Type 1). Subjects were instructed to push a button, when the sensation changed from one of pressure alone to a sensation of both pressure and pain. Pressure algometry was performed in triplicate at each of 10 neck- and jaw-muscle spots, and three times at a reference point. Briefly, the algometer was placed at a right-angle on the muscle. The probe area was 1 cm2, and the slope control was set to a desired rate of change, in a pressure of 20 kPa/s (Fig. 1a). A test of the algometer showed that the slope at this setting actually was 33.3 kPa/s (± 4.2%). Since the same algometer was applied throughout the study, it was anticipated that the insecurity in slope setting of the algometer equally influenced the measurements on whiplash-injured persons and controls. Calibration of the algometer was performed at regular intervals, and internal error in the machine was 0.0 ± 0.062%.

(a) Examined points using pressure algometry: (1) m. temporalis; (2) m. masseter; (3) m. sternocleidomastoideus; (4) m. trapezius, upper trapezius fibres; (5) m. infraspinatus. (b) Examined points using palpation: (1) m. temporalis posterior; (2) m. temporalis anterior; (3) m. masseter; (4) m. pterygoideus lateralis; (5) m. sternocleidomastoideus, insertion at processus mastoideus; (6) m. sternocleidomastoideus pars medius∗; (7) superior and inferior nuchal lines; (8) m. trapezius, upper trapezius fibres∗. ∗Dig. I opposed to dig. II and III, other muscles palpated using firm pressure with dig. II and III.
On the left and right side of the neck and the head, five homologous spots were examined in the following order (Fig. 1a): (i) the superficial mid-belly of the masseter muscle (1.5 cm from the mandibular angle); (ii) the temporal muscle at the intermediate portion (TP2); (iii) the sternocleid muscle at the mastoid attachment site; (iv) the trapezius muscle, upper trapezius fibres (TP1) at the insertion site of the clavicle; and (v) the infraspinatus muscle 1.5 cm below the medial part of the scapular crest (26). Firstly, measurements were done on the left, and secondly on the right side. The left, dorsal, proximal interphalangeal joint was chosen as a control site for determination of distant pressure pain detection threshold (distant PPDT).
Eight pericranial muscles were examined by manual palpation (Fig. 1b). Muscles were palpated on both sides as described by Langemark & Olesen (27) with the second and third fingers performing small rotatory movements, while firmly pressing the fingers against the examined muscle. From each of 16 examined sites, a tenderness score was given. Points were scored as described by Langemark & Olesen (27): 0 = no visible reaction, and denial of tenderness; 1=visible reaction, but no verbal report of discomfort or mild pain; 2=verbal report of painful tenderness with facial expression of discomfort; 3=marked grimacing or withdrawal, verbal report of marked, painful tenderness and pain. Total tenderness score (TTS) was calculated (maximum possible score=48).
The following examination order was used (Fig. 1b): (i) posterior temporal muscle; (ii) anterior temporal muscle; (iii) masseter muscle; (iv) lateral pterygoid muscle (the subject slightly opens his mouth during this procedure); (v) sternocleid muscle at the mastoid process; (vi) sternocleid muscle at the medial part, muscles inserting on superior and inferior nuchal lines; and (vii) trapezius muscle.
Statistics
Sample size was calculated with an estimated standard deviation in total pressure pain detection threshold at 500 kPa. We expected a difference in means between whiplash and ankle distortion subjects of 300 kPa (an average of 30 kPa lowered PPDT in all measured point), giving a power of 0.90 at α= 0.05 with a sample size of 120 whiplash-injured persons and 40 controls.
To achieve most information, we computed regression lines for each participant using the following data pairs: x=number of days after trauma, y=measured value on exact day of examination. A line was fitted through obtained values after each examination day for every participant. Participants were represented by a point on their individual line, and the computed value on this line at day 90 was chosen to describe each participant. Individual regression lines were expected to have greatest variation at endpoints (0 days and 180 days after trauma), and least variation at the midpoint. We also used day 0 (alpha) as a parameter, supposing data density would be highest at the start of the observation time. Individual regression lines were computed with Excel for Windows software. To be included in these calculations, participants needed to attend at least twice during follow-up. One hundred and twenty-three whiplash-injured and 36 ankle-injured patients fulfilled these criteria.
Total pressure pain detection threshold (total PPDT), distant pressure pain detection threshold (distant PPDT), Total tenderness score (TTS) and mean VAS pain at day 0 and day 90 were calculated according to the above notions. Data were transformed by means of either natural logarithm transformation (pressure pain detection threshold data) or square root transformation (total tenderness score and mean VAS day 90) in order to achieve normally distributed data sets. A general linear model (GLM) was applied post-hoc to analyse covariation due to gender, subject type and age. GLM was further applied to evaluate the relationship between reported pain and measured total tenderness score and pressure pain detection threshold.
Results
The whiplash and ankle distortion groups were similar with respect to age, gender and body mass index. Symptom frequency is presented in Table 1.
Frequency of painful and non-painful complaints with 95% confidence interval in whiplash and ankle injured patients after 1 week and 1, 3 and 6 months

Eighty-seven per cent of participating whiplash-injured patients had returned to work or usual activity within 6 months, 10% had not recovered, 3% did not respond to enquiries. Ankle-injured controls had all recovered within 6 months.
Whiplash-injured patients had a significantly lower total pressure pain detection threshold than ankle distortion subjects at day 0 (P < 0.01) and day 90 (P = 0.01) (Table 2 and Fig. 2a). Post-hoc analysis, however, revealed no difference in raw data after 6 months observation time (P = 0.06). These findings were in accordance with a significantly higher total tenderness score in the whiplash group immediately after (day 0: P < 0.01), 3 months (day 90: P < 0.01) later, but not 6 months after trauma (day 180, raw data: P = 0.23) (Table 2 and Fig. 2b). For details on each muscle spot, refer to Fig. 3(a–f). Measurement on the left proximal interphalangeal joint of the third finger showed pressure pain thresholds in whiplash-injured persons to be similar to ankle distortion subjects at all examination days after trauma (day 0: P = 0.12; day 90: P = 0.15, day 180 (raw data): P = 0.46) (Table 2 and Fig. 4).

(a) Pressure pain detection thresholds of muscles in whiplash and ankle distortion assessed with pressure algometry. Data are log-transformed. Solid square=whiplash, and open square=ankle distortion. Parenthesized numbers refer to number of subjects examined on the particular examination day. (b) Muscle tenderness in head and neck. Each muscle score graded from 0 to 3, maximal score is 48. Data are square root transformed. Solid square=whiplash and open square=ankle distortion. Parenthesized numbers refer to number of subjects examined on the particular examination day.

(a-f) Pressure algometry of specific muscles at day 0 and day 90. Data are log-transformed. Solid square=whiplash and open square=ankle distortion.
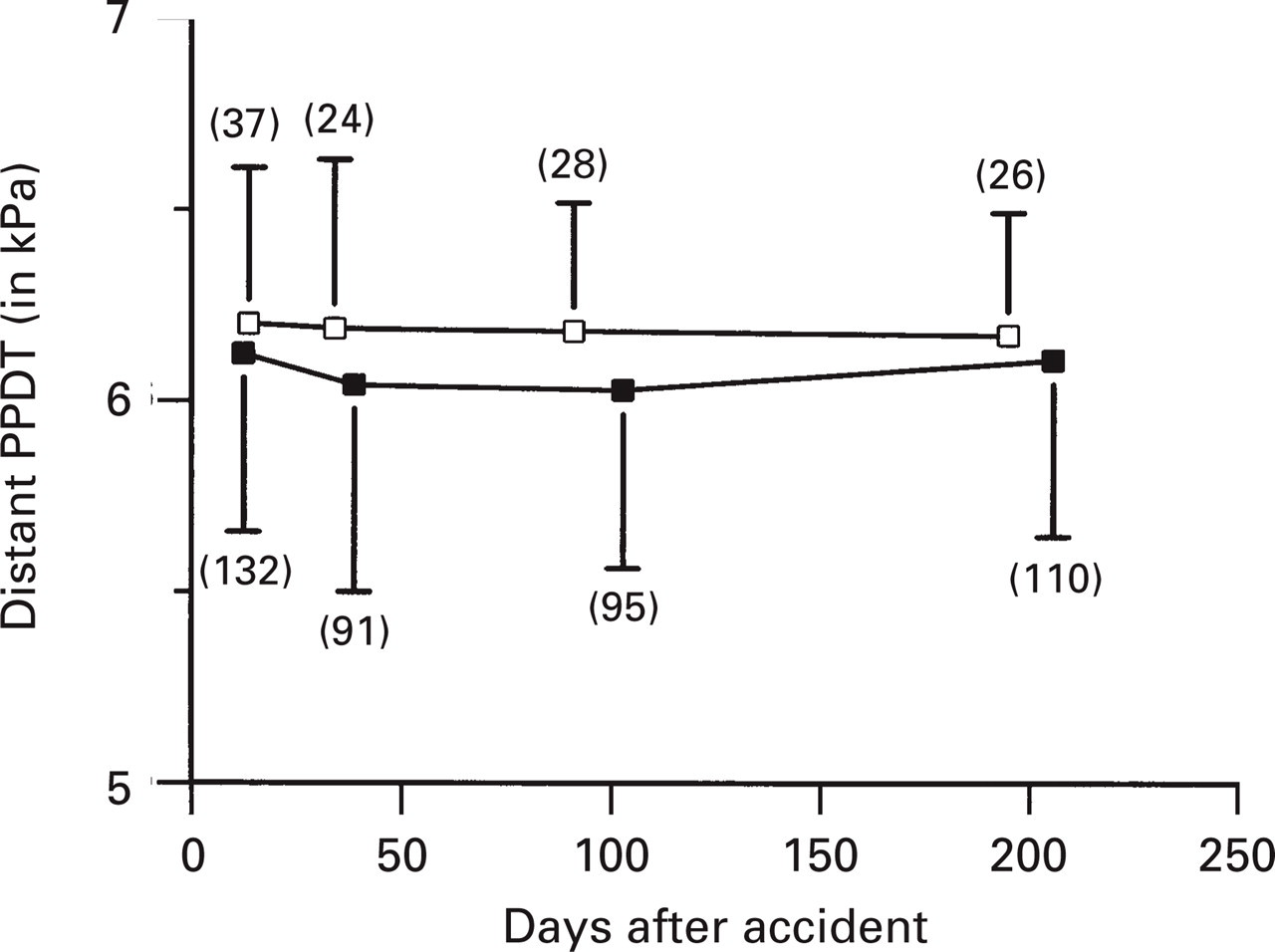
Distant pressure pain detection threshold, mean±
Pressure pain in whiplash and ankle distortion

PPDT=pressure pain detection threshold, TTS=total tenderness score. Ln=logarithmic transformation, Sqrt=square root transformation. Values for day 0 and 90 are computed as described in statistics. Mean values±standard deviations are shown. The mean difference between whiplash and ankle injured with 95% confidence intervals is shown.
In the whiplash group, there was a marked sex difference in total pressure pain detection threshold (day 0: P < 0.01, day 90: P < 0.01). Distant pressure pain detection threshold was also lowered in women (day 0: P < 0.01, day 90: P < 0.01). Total tenderness score did not reveal sex differences in this study.
To further analyse the observed sex difference, when using pressure algometry, we applied a statistical general linear model to estimate covariation due to gender, subject type, age and body mass index (BMI) in all subjects.
Total pressure pain detection threshold at day 0 showed a significant gender-effect of 19.1% (P < 0.01) and type of subjects only accounted for 1.9% (P = 0.04) of variation at day 0, age accounted for 9.0% (P < 0.01) and BMI for 4.7% (P = 0.001) of variation in total pressure pain detection threshold. General linear model analysis of total pressure pain detection threshold at day 90 revealed a significant gender-effect=17.7% of variation (P < 0.01). The type of subject was responsible for 3.0% of data variation (P = 0.01). Age accounted for 4.3% (P < 0.01) and BMI for 2.8% (0, 02). To further study possible effect on local vs. general sensitization, GLM analyses on distant pressure pain detection thresholds on day 0 and day 90 were performed. At day 0 gender accounted for 12.7% (P < 0.01), and at day 90 for 7.0% (P < 0.01) of variation. Gender-dependent variation, in pressure pain detection threshold was present in both local and remote area.
Pain and tenderness
Correlation analysis and linear regression was performed on mean VAS pain at day 90 (compound mean of: neck pain, headache, shoulder-arm pain, low back pain) and total pressure pain detection threshold, distant pressure pain detection threshold and total tenderness score at day 90. For pressure algometry, whiplash-injured persons had a significantly inverse linear relationship between mean VAS pain at day 90 and total pressure pain detection threshold 90 (R =− 0.36, P = 3.9∗10−5) (Table 3). This inverse relationship was also seen in ankle distortion subjects (R =− 0.59, P = 1.9∗10−4). The slope was significantly steeper in ankle distortion subjects (P < 1.0∗10−8) than in whiplash. At distant control sites, the slope for mean VAS and pressure pain detection threshold was not significantly different from 0 in whiplash (P = 0.29) and in ankle distortion (0, 13), and there was no significant relationship in whiplash-injured persons (R =− 0.25, P = 0.06) (Table 3). Palpation data showed a significant linear relationship between mean VAS pain day 90 and total tenderness score day 90 in whiplash-injured persons (Table 3) (R = 0.57, P = 3.2∗10−12).
Pain and tenderness in whiplash and ankle injury
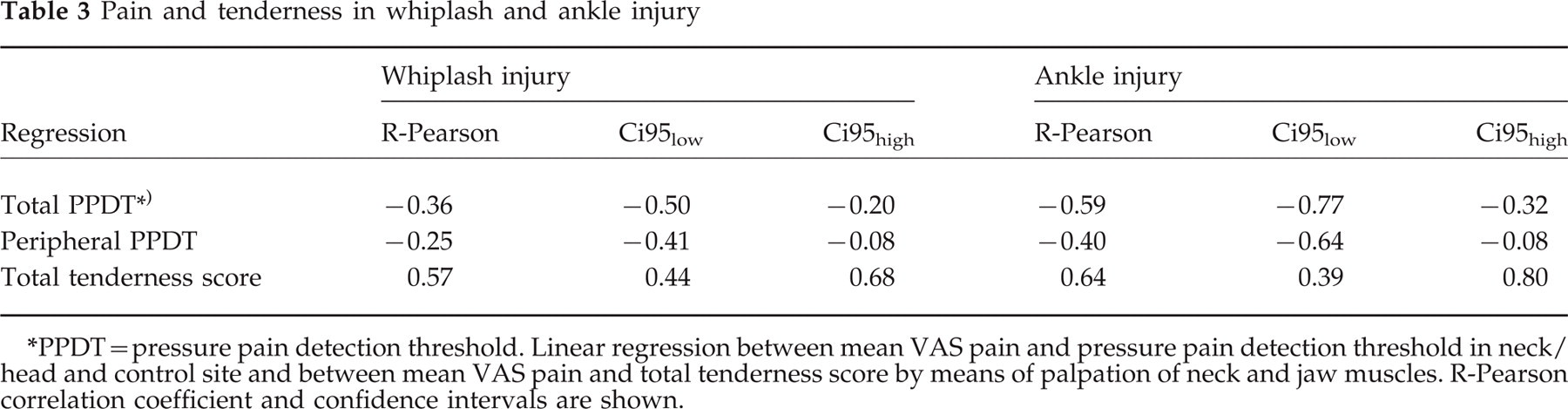
PPDT=pressure pain detection threshold. Linear regression between mean VAS pain and pressure pain detection threshold in neck/head and control site and between mean VAS pain and total tenderness score by means of palpation of neck and jaw muscles. R-Pearson correlation coefficient and confidence intervals are shown.
Discussion
The main finding of this study is a lowered pain threshold to pressure in the neck and head in the first 3 months, but not 6 months after whiplash injury as compared with a sex- and age-matched control group exposed to another injury: ankle distortion. This suggests that sensitization of musculoskeletal structures is found in the early period after injury, and that this sensitization would not be ascribed to general stress associated with an external trauma. In addition, it appears that musculoskeletal sensitization is local, rather than general. The observed correlation between mean VAS pain and total tenderness score and the inverse relationship between mean VAS pain and total pressure pain detection threshold also suggest that local sensitization and pain are linked. Whether the observed small numerical difference in pressure pain detection thresholds (Table 2, Fig. 3a-f) between whiplash and ankle-injured participants is a clinical difference is, however, to be questioned. The difference in palpation score is larger, and seems to be of clinical importance also (Table 3).
Sensitization in muscle pain
A vast literature shows that persistent noxious input from muscles results in sensitization (28–32). Sensitization of muscles is reflected in, for example, a lowering of threshold to pressure and palpation, an altered stimulus response function (17), and a build-up of pain following repetitive stimulation at the same location, abnormal temporal summation and following spatially separated saline infusions, spatial summation (16). Previous studies have shown a lowering of threshold to electrical stimulation of muscles in fibromyalgia or musculoskeletal pain (33). Similar findings have been seen using hypertonic saline infusions in fibromyalgia (17). Stimulus response function has been found to be qualitatively different in fibromyalgia (16) and in tension-type headache (21). Repetitive stimulation of the tibial muscle has also been shown to produce a facilitation of temporal summation in fibromyalgia subjects (16). In the present study, only threshold to mechanical pressure and palpation was measured. The clear lowering of threshold to palpation and mechanical pressure in the first 3 months but not 6 months after whiplash injury suggests that sensitization may only be a transient phenomenon. We have previously seen that in a small proportion of whiplash-injured patients with long-term complaints, sensitization is indeed seen.
General vs. local sensitization
While mechanical threshold was clearly reduced in the cervical region in whiplash-injured patients early after injury, such reduction of threshold was not seen remote from the injury site, indicating a local, as opposed to a general, sensitization. We would note, however, that in a recent study (22) of 11 chronic whiplash-injured persons, muscular hyperalgesia was reported locally as well as distantly from the injury site. We have no explanation for this difference between studies. Differences in selection of patients, the retrospective design, and a longer lasting pain condition in the latter study are factors that may play a role.
In previous studies of patients with other musculoskeletal disorders, findings differ from our study. Vecchiet et al. (33) in fibromyalgia patients found that these patients had a lowering of threshold to electrical stimuli in both painful and non-painful muscles. While their study suggests that fibromyalgia patients may have a generalized reduction of threshold, the reduction appears to be local in unselected prospectively followed whiplash-injured subjects. This notion is supported by preliminary observations in whiplash-injured patients that they perceive cold pain to the same extent as ankle-injured patients when their hand is immersed into ice-cold water (unpublished observations).
Post-injury stress vs. sensitization
In the present study, we compared two groups of subjects exposed to a traumatic injury: a group of whiplash-injured and a group of ankle-injured persons. Ankle-injured controls reported pain, and the present global pain intensity reported initially by means of the McGill Pain Questionnaire in controls was actually significantly higher than in whiplash-injured patients (Kasch et al., unpublished observations). The observation that pain threshold in the cervical region was significantly lowered in the whiplash group, but not in the ankle distortion group, suggests that the general stress associated with a traumatic injury can not explain the lower threshold in the whiplash group. This notion is also supported by the finding that threshold to pressure at distance from the injury region was not different from that seen in the control group. It must, however, be noted that whiplash-injured patients probably have different expectations regarding recovery than ankle-injured patients, that subsequently might influence their attitudes after injury. In the whiplash group, 10% were still on sick-leave after 6 months, whereas ankle-injured patients had made a full recovery.
Pain threshold and women
Pain threshold and tenderness scores were lower in women than in men in both whiplash and in ankle distortion subjects. This was observed both locally and at distance. This finding is consistent with an extensive literature showing a reduction of pain threshold in normal female subjects (34–36), and in patients with fibromyalgia (37), cephalic muscle tenderness (21, 38), tension-type headache (27) and temporomandibular dysfunction (39). The reduction is found both on detection and on tolerance threshold. The mechanism for this gender effect on pain threshold is not known. Relationships between lowered threshold in female gender and preponderance of women with musculoskeletal disorders including whiplash injury complaints remain speculative. Higher percentage of body fat, smaller muscle mass, lower blood pressure, different stress-response, cyclic hormonal fluctuations, different cerebral and medullar organization and bio-psycho-social factors, are factors that can influence pain thresholds (40).
Conclusion
In this study, we found that whiplash-injured patients in the early phase after whiplash injury had focal sensitization to pressure of deep structures in the neck and jaw muscles by means of pressure algometry and palpation. Six months after injury, whiplash- and ankle-injured patients were similar with respect to muscle tenderness. Total pressure pain in the neck and jaw muscles is inversely correlated to reported pain in whiplash. Focal sensitization may play a role in early, but not in late, symptoms after whiplash injury.
Footnotes
Acknowledgements
Recruitment of subjects was facilitated by the staff at the emergency units at Aarhus County Hospital and Aarhus Municipal Hospital during the enrolment period.
Statistical guidance was given by the Department of Biostatistics, University of Aarhus. The prospective study was supported financially by grants from: The Danish Society of Polio and Accident Victims (PTU), Insurance and Pensions in Denmark, The Danish Medical Research Council, Danish Pain Research Center, and The Danish Rheumatism Association.