
Abstract
Falling asleep as a means of ending migraine attack was studied in 133 4–16-year-old children in out-patient settings. Children registered 999 migraine attacks in headache diaries using a visual analogue scale (VAS) in 409 attacks and a five-face scale in 590 attacks. The distribution of maximal pain intensity was similar on both scales; on VAS 88% assigned grades between 63 and 100, and on the face scale 93% assigned grades of 4 or 5. Children fell asleep during 33% of the attacks (n = 329), in 64% of these within the first hour (n = 209). Of the children, 68% (n = 91) had fallen asleep at least once during an attack. Falling asleep was more common in children under 8 years of age than in older children. In those under 8 years, 62% (95% confidence interval (CI) 49–75%) of attacks were resolved by sleep, in those aged 8–12 years 34% (26–41%), and in children > 12 years 24% (15–33%) (
Introduction
Headache is a common complaint among children; 70% of all children have suffered from headache at least once and 20% of 15-year-old children have had recurrent headache (1). Prevalence of migraine in different studies has been 4–11% among schoolchildren and somewhat less common in younger children (1–3). Migraine attacks in children can also be very painful (4). The assessment of pain in children is often difficult, thus self-reporting scales have been widely used to simplify the procedure. Visual analogue scales (VAS) and face scales have both been described as comparable and reliable methods of assessment in children over 4 years of age, objectively correlating with the intensity of pain evaluated by behaviour (5).
Migraine attacks commonly end during sleep; 50–84% of adult migraine patients had complete recovery or marked resolution after sleep (6, 7). Clinically, sleep seems to be a common conclusion for children as well, but very little research data exist so far. The aim of this study was to investigate sleep as an end of migraine attacks in children in the home setting.
Patients and methods
This prospective study enrolled 133 patients and was part of a larger investigation of optimal treatment of childhood migraine performed during the years 1992–1995 (8). All children were out-patients of the Children's Hospital of the Helsinki University Central Hospital, Jorvi Hospital or Aurora Hospital and lived in the Helsinki metropolitan area during the study. Recurrent headaches were diagnosed as migraine according to the International Headache Society (HIS) criteria (9). The mean age of the children was 10.8 (4.6–16.9) years; 52.6% (n = 70) were boys and 47.4% (n = 63) were girls.
Patients kept a headache diary using either a five-grade face scale (5) or a 10-cm VAS (10) chosen according to patients' preference. In the scale applied, patient chose a value that best described the intensity of headache at the beginning of the attack, a second value 30 min later, and then hourly for a maximum of 5 h. In addition, throughout the attack, patient or parents made remarks about falling asleep, nausea, vomiting and other accompanying symptoms. Close correlation between the five-grade face scale and the continuous visual scale has been demonstrated previously (5). To combine the two groups with different scales, the VAS data were transformed as follows: 0 to ≤12 = grade 1; 13 to ≤37 = grade 2; 38 to ≤62 = grade 3; 63 to ≤87 = grade 4; and 88 to ≤100 = grade 5. Diaries used in this study were not included in the previously mentioned pharmacological study.
For evaluation, patients were grouped according to their age as follows: patients younger than 8 years, those between 8 and 12 years, and those older than 12 years.
For analysis, attacks were classified according to the mode of the end: (i) attacks that ended in falling asleep (after 0.5 h, 1 h, 2 h or > 2 h from headache inception); (ii) attacks that ended without sleep (duration less than 2 h, from 2 h to 4 h or more than 4 h to 5 h); and (iii) attacks in which the resolution of the symptoms was not registered (duration < 5 h or > 5 h).
In this study, the effect of any drugs administered was not analysed, as the aim of the study was to clarify what happens in a real clinical situation. Almost all of the children used drugs (125 out of 133), the number of which varied from one to six. Results are given in percentages, mean values and 95% confidence intervals (CI). Frequency of falling asleep is defined as the proportion of attacks that resolved by falling asleep in a single patient. Frequency of missing data is defined as the proportion of attacks in which the recording failed in a single patient. Differences between the groups were assessed with the χ2 test, the analysis of variance (
Results
Altogether 999 attacks of migraine were registered in the diaries; the mean number of attacks in one patient was 7.5 (range 1–49). A total of 409 attacks were registered with the VAS and 590 attacks with the face scale. Of all attacks, 329 (32.9%) ended in falling asleep, in 431 attacks (43.1%) the pain resolved without sleep, and in 239 attacks (23.9%), the resolution of symptoms was not registered.
The VAS was chosen by 49.6% (n = 66) of the children; mean age 12.1 (7.6–16.9) years. The face scale was chosen by 44.4% (n = 59); mean age 9.5 (4.6–15.3) years. Eight patients (6%) used both scales. Use of the VAS requires higher cognitive skills and children using this scale were older than those using the face scale (t-test, P < 0.0001).
The distribution of the maximum intensity of pain observed in each child was comparable for both VAS and face scale (Fig. 1a). Most of the patients estimated the pain during the attack to be close to the worst pain imaginable. The median maximum pain intensity of all the attacks registered on the face scale was grade V. When the VAS was used, the median maximum intensity was 94, which corresponded with grade V (87–100). Maximum intensities of pain during single attacks are presented in Fig. 1B.

Pain observed in migraine attacks. (a) Maximum pain observed in 133 individual children, aged 4–16 years. (b) Maximum pain of 999 attacks in the same children. ▪, VAS;□, face.
Within the 5-h observation time, 431 attacks were resolved without sleep, of which 165 (38%) resolved within the first 2 h, 218 (51%) between 2 h to 4 h and only 48 (11%) lasted > 4 h.
Data on migraine resolution were missing in 239 attacks. In 96 attacks (10% of all attacks), registration had failed during the first 5 h; 50 patients belonged to this group. End of 143 attacks (14%, 51 patients) was not registered because the attacks exceeded the maximum follow-up time of 5 h. In the VAS group, registration failed in 142 of 409 attacks (35%; 90 attacks after 5 h), and in the group using face scale, end was not registered in 97 of 590 attacks (19%; 53 after 5 h). Registration failed in 12% of the attacks in children < 8 years, in 21% in those between 8 years and 12 years and in 39% in those > 12 years.
Falling asleep was observed at least once in 68% (n = 91) of the children. In the subgroup of 24 patients < 8 years of age, 57% of attacks (118 of 209), in the 62 children from 8 to 12 years of age, 33% of attacks (166 of 503), and in the 47 children over 12 years old, 16% of attacks (45 of 287) ended with falling asleep. Mean frequencies of falling asleep, CIs in different age groups and in relation to gender are given in Table 1 and frequency distributions in Fig. 2. Children usually fell asleep quite soon after onset of the attack. Sleep terminated 126 attacks within the first 0.5 h, 83 attacks between 0.5 h and 1 h, 55 attacks between 1 h and 2 h, and 65 attacks after 2 h observation time. Termination of the migraine attack in children who fell asleep was significantly more common during the first 2 h compared with those who did not fall asleep (80% vs. 38%; χ2 P < 0.0001).
Mean percentage of migraine attacks in children that ended in falling asleep

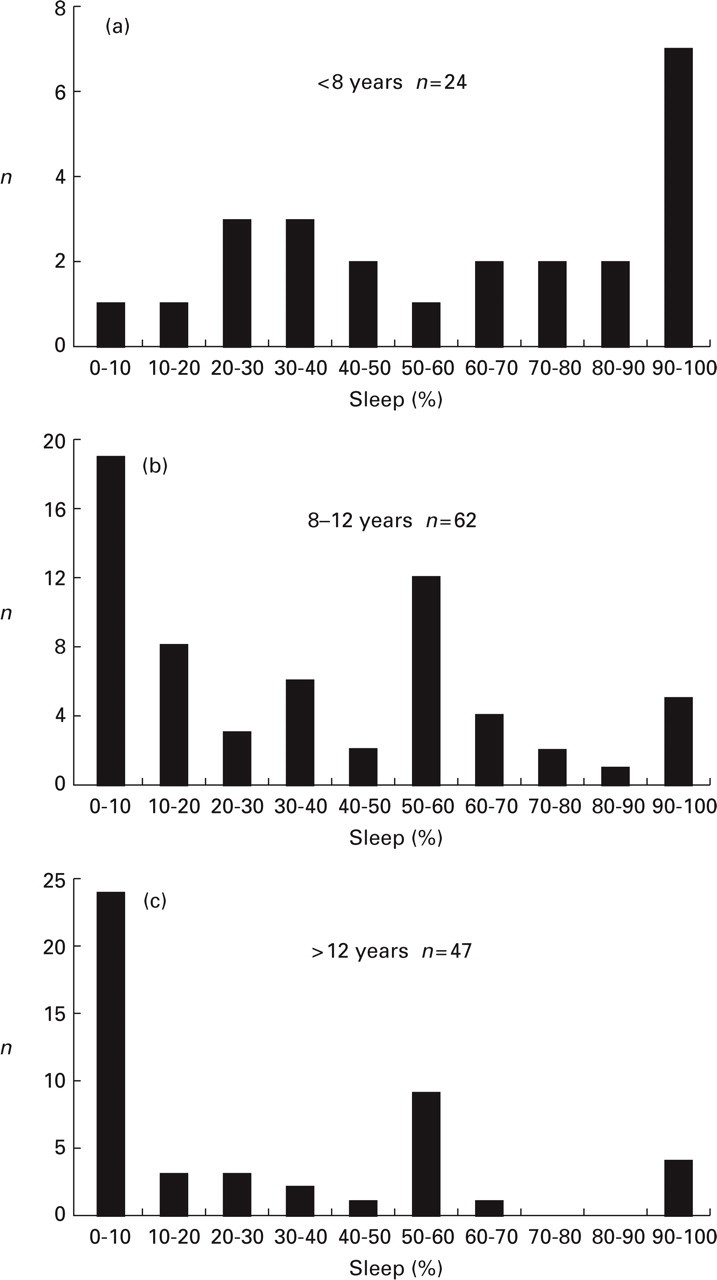
(a–c) Frequency distribution of migraine attacks that ended with sleep shown in percentages for different age groups.(a) Twenty-four children under 8 years; (b) 62 children 8–12 years; (c) 47 children over 12 years.
Frequency of falling asleep during attack was significantly more common in patients < 8 years of age compared with older patients (
The missing data of migraine resolution due to registration failure did not have a significant effect on results (
Discussion
This study confirms that children's migraine attacks are quite painful and frequently in younger children end in falling asleep. Most of the patients had described the pain during some attacks as the worst possible pain imaginable; similar results were obtained whether the face scale or the VAS was used. In previous study, partially based on the same population as this study, 69% of patients described their pain to be close to the worst imaginable pain (11). The median of maximum pain intensity of all the attacks registered was also very high on both scales. The attacks that were registered with VAS appeared to be slightly more painful compared with the attacks registered with face scale (Fig. 1b). Patients using VAS were older than patients using face scale, and these results are in agreement with previous findings that older patients have stronger symptoms during a migraine attack (4, 12). VAS and face scale have earlier been shown to correlate well with other types of measurement of pain (5). Former studies have also shown that migraine attacks in children are very painful; for example, half of the children cry during the attack and more than half are forced periodically to stay out of school or kindergarten (4).
Children's migraine attacks are often shorter in duration compared with migraine attacks of adults. The results of earlier studies concerning the duration of the attack are variable. In one study, 45% of attacks ended within 2 h of onset (13), whereas in another study, the mean duration of an attack was from 7.9 h to 18.1 h, depending on the children's age and the type of migraine. Attacks with aura were significantly longer in duration compared with attacks without aura (4). Within the 5-h observation period in our study, 43% of attacks ended without sleep. We did not assess the effect of the type of attack or any pain medications used.
Diaries were filled in quite carefully; only 10% of attacks were inadequately registered. Registration was interrupted before the end of attack, most often because the duration of the attack exceeded the 5-h follow-up time. This was true for both scales applied, but especially for the patients using the VAS. Termination of the attack was registered with VAS less frequently than with face scale. This difference was mostly due to the longer duration of attacks in patients who were applying VAS. Patients using the VAS were generally older than patients using the face scale. It has been previously reported that older children tend to have longer attacks (4). Furthermore, parents of younger children, who more frequently used face scale, were more active in taking part in filling in the diary; this may explain in part the better compliance of the face-scale group.
End of the attack by falling asleep was significantly more common in patients < 8 years old than in older patients; it was most frequently observed in girls < 8 years old. The role of sleep in the resolution of headache and as a part of the natural healing process of migraine attack has long been known, although there are relatively few publications on the subject. In a child population, sleep and resting were cited as the primary treatment choice for 28% of migraine patients (14). The role of sleep as a treatment of migraine was studied in 310 adult patients, half of whom fell asleep within 3 h after taking medication, with the other half resting without sleep; 50% of those who fell asleep had full recovery, while this was true for only 31% of the control group (7).
In a study of 34 children, 74% fell asleep during migraine attack, 56% of them within the first half an hour (15). In our study, results were quite similar: 68% of children fell asleep during the attack, 38% within the first half an hour. In patients < 8 years old, falling asleep is more common during the attacks, possibly due to their milder intensity (4).
In our study, almost half of the attacks resolved within 5 h and one-third of attacks ended in falling asleep. Duration of attacks was thus quite short; almost all the children used drugs to relieve the attacks (125 children out of 133). Administered medication was likely to have an effect on the duration of pain and may also have had an effect on sleep frequency. Falling asleep may be considered a sign of pain resolution or a normal phase of the migraine attack. Headache generally has been shown to disturb sleep; 10% of paediatric migraine patients have been reported to wake repeatedly because of headache (16). The tendency to fall asleep is more common among young children; furthermore, resolution of an attack seems to be faster in young patients. Falling asleep was less common in older children, who had more painful attacks of longer duration. In future studies, falling asleep in resolution of a migraine attack should be further studied and the effect of administered medication also assessed.
Footnotes
Acknowledgements
This paper was presented in part at the 12th Migraine Trust International Symposium, 1–4 September 1998, London, UK.