
Abstract
Migraine patients abusing ergotamine often have chronic daily headaches associated with tiredness, sleep and memory disturbances, and reduced general well‐being. We quantified psychological and cognitive functioning in 12 migraine patients with and 12 without ergotamine abuse (≥ 5 days/week for ≥ 6 months) and 12 healthy controls. Psychological functioning assessed by Symptom Checklist‐90 (SCL‐90) and Profile Of Mood State (POMS), was impaired in ergotamine abusers compared to healthy controls. Cognitive functioning divided into four domains:
Despite formal lack of evidence for efficacy and a wide range of often severe side‐effects, ergots are still being frequently used in the treatment of migraine attacks (1). On long‐term use, many patients will develop the syndrome of ‘ergot headache’, characterized by gradual increase of headache frequency and ergot consumption (2, 3). Ultimately, patients will use ergots (nearly) daily and will have chronic (nearly) daily headache associated with tiredness, attention problems, sleep and memory disturbances, and reduced general well‐being (4–6). These symptoms usually improve after drug withdrawal (7–9). Little is known about the effects of ergotamine abuse on psychological and cognitive functioning. Three studies, one using critical flicker fusion analysis (10) and two using visual evoked potentials (11, 12) have suggested impaired cognitive functioning in patients with ’ergot headache’. The present study was designed to quantify differences in psychological distress and cognitive performance in migraine patients with and without ergotamine abuse.
Methods
Subjects
Ergotamine‐abusing patients were recruited through advertisement in newspapers and the journal of the Dutch migraine patient association. Ergotamine abuse was defined as intake of ergotamine‐containing medication on 5 or more days a week, for more than 6 consecutive months. For each ergotamine abuser an age‐ and sex‐matched migraine patient (13) was selected from the migraine patient database of the neurology outpatient clinic of Leiden University Medical Centre. They were not to use or to have ever used on a regular basis ergotamine‐containing drugs on more than 1 day per 2 weeks. Age‐ and sex‐matched friends of the patients who had never experienced a migraine attack, nor had suffered from tension‐type headaches for more than 10 days a month or had abused analgesics, were invited as second control group. Approval of the study protocol was obtained from the local ethics committee of Leiden University Medical Center and informed consent was obtained from each subject before enrolment in the study.
Study design
All participants were investigated using a standardized protocol. Subjects were asked to complete a headache and medication questionnaire and the Symptom Checklist‐90 (SCL‐90) at home. During a visit to the hospital all participants were asked about their education years and level. Education years were defined as the amount of education years after primary school. Education level was defined using a 5‐point scale in which 1 represents special education, 2 = lower, 3 = middle, 4 = higher secondary school and 5 = university. Thereafter, short physical and neurological examinations were performed and participants were asked to complete the shortened Profile of Mood State (POMS) and to perform several neuropsychological tests. Ergotamine abusers were asked to withdraw abruptly from ergotamine. Those who did so were retested at least 3 months after withdrawal.
Psychological distress measures
The SCL‐90 estimates the general psychological and somatic state of the participants, and consists of 90 statements, which have to be rated on a 5‐point scale (14–15). The questionnaire shows a high validity and has been used previously in substance abuse populations (16–18). The Dutch version comprises nine subscales: depression, somatization, interpersonal sensitivity, obsessive‐compulsive disorder, anxiety, hostility, phobic anxiety, sleeping problems and miscellaneous. The total SCL‐90 score indicates the general level of distress. The questionnaire was completed by all participants in their usual environment, on a normal weekday and reflected the psychological distress over the past 7 days. The POMS measures the actual psychological state of the participant and consists of 32 feelings, which have to be rated on a 5‐point scale (19–20). It comprised five subscales: depression, anger, fatigue, tension and vigour. All items of the POMS referred to the patient's feeling at the time of completing the questionnaire (during the hospital visit).
Cognition
Based on complaints from ergotamine abusers, like tiredness, concentration problems, sleep and memory disturbance and reduced general well‐being, we selected four different neuropsychological domains in which we expected to see differences between the three groups. The selected domains, earlier described by Denburg et al. (21), were attention, speed of information processing, memory and cognitive flexibility. For each of the four domains standard neuropsychological measurements were used.
Attention was measured by the critical flicker fusion test (CFF) (10–22) and the mental control subscale of the Wechsler Memory Scale (WMS) (23).
Speed of information processing was measured by simple and complex visual reaction time tasks (24) and the lexical decision task (LEXDEC). The LEXDEC is a four‐level test with increasing cognitive task load (25), during which subjects had to evaluate words which appeared on a PC screen by pressing keyboard keys (← ‘yes’ or → ‘no’) according to the following criteria: onset of appearance (test 1, 25 trails for each key), written in capitals or not (test 2, 50 trials), representing organic matter or not (test 3), and finally, written in non‐capitals and representing non‐organic matter or not (test 4). For each task condition the same set of words was used, and reaction times and accuracy (% correct reactions) were computed.
Memory was assessed with four subscales of the WMS: immediate verbal memory (digits forward), verbal memory (logical passages), visual‐spatial memory (visual reproduction) and verbal learning (paired association) (23).
Cognitive flexibility was measured by trailmaking test A and B (22–27) and WMS digits backwards (23).
Statistical analysis
Differences between groups were analysed by means of the Kruskal–Wallis one‐way
Results
Subjects
The demographic and clinical characteristics of the study population are summarized in Table 1. A total of 12 ergotamine abusers (years of addiction 11.3 ± 2.3) entered the study. The average number of days of ergotamine intake per month was 28 ± 1, and the average dose per day was 2.1 ± 0.3 mg. One patient used in addition daily sumatriptan, six patients used daily analgesics, two used antidepressive medication, one used benzodiazepines, and three used β‐blockers (two as prophylactic medication for migraine and one for hypertension). All abusers took their normal daily dose of ergotamine on the day of investigation. Two migraine patients used β‐blockers (one for prophylactic medication and one for hypertension). The three groups showed no differences in education years or level of education.
Demographic and clinical characteristics of study population (n = 36)

Expressed as mean ±
Psychological distress
Total SCL‐90 scores (the general level of distress) differed significantly between the three groups (ergotamine abusers: 157 ± 13, migraine patients: 122 ± 7, healthy controls: 102 ± 2,
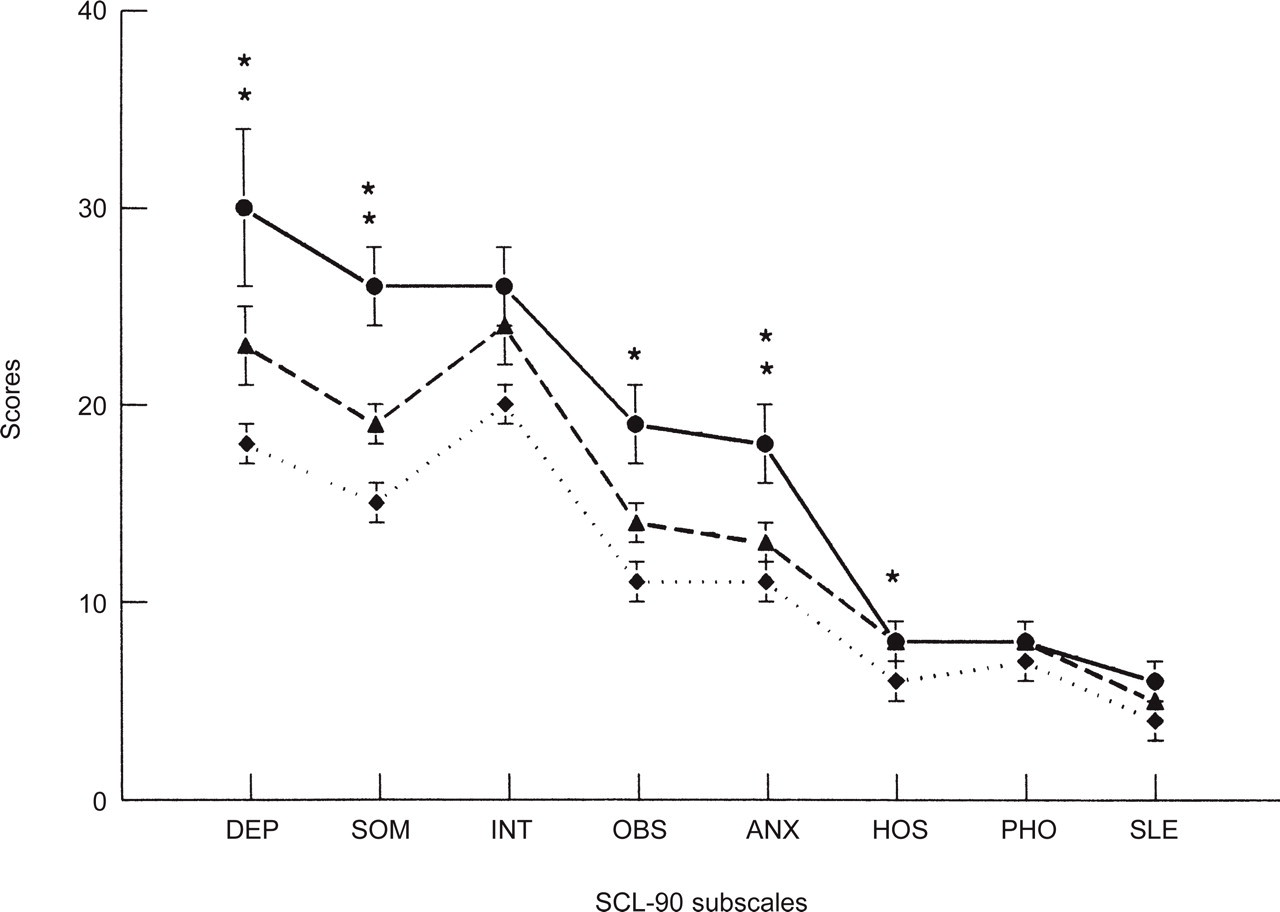
The SCL‐90 subscale scores expressed as mean ±

The POMS subscale scores expressed as mean ±
Cognition
All measures of cognition are summarized in Table 2. The measurements for attention and memory did not differ between the three groups. Speed of information processing differed significantly between groups only for complex reaction time tasks (CRT;
Results of cognitive measurements for the four neuropsychological domains (mean ±

Since psychological distress influences cognitive performances (28), we corrected the found differences in motor time (CRT) and speed of trailmaking test A for total SCL‐90 scores. After correction, neither of the two tests differed significantly between the three groups (
Withdrawal
Seven patients withdrew from ergotamine within the study period. Compared to those who did not they tended to have more years of education (6 ± 1 vs. 3 ± 1 years, respectively;

Total SCL‐90 scores of seven ergotamine abusers before and after withdrawal (mean withdrawal period 5.4 ± 1.8 months). The numbers of headache days per month before and after withdrawal are indicated.
Individual differences in psychological distress and cognitive performances after ergotamine withdrawal

Age in years; TMT‐A = trailmaking test A; CRT‐MT = motor time during the complex reaction time task.
Number of headache days per month before and after withdrawal; reduction of more than 20 headache days after withdrawal was defined as response to withdrawal treatment.
Discussion
In this study we objectivated psychological and cognitive functioning of migraine patients abusing ergotamine by means of a neuropsychological test battery. We found that ergotamine abusers showed higher psychological distress (total SCL‐90 scores) compared to healthy controls, and that migraine patients had intermediate scores (Fig. 1). Furthermore, we found that for the four selected cognitive domains ergotamine abusers had a slower speed of information processing (complex reaction time) and lower cortical flexibility (trailmaking test) compared to healthy controls. Again, migraine patients scored in‐between. However, the three groups did not differ in cognitive functioning after correction for psychological distress (total SCL‐90 score). Thus, ergotamine abusers and to a lesser degree migraine patients performed worse on two cognitive tests than healthy controls, most likely due to higher psychological distress.
This correlation between psychological and cognitive functioning is supported by findings in the seven abusers who were tested at least 3 months after withdrawal from ergotamine. All patients who improved after withdrawal (≤ 10 headache days per month) showed decreased psychological distress and performed better on the two cognitive tests (Table 3). Although both other groups were not tested for the second time, it seems unlikely that learning effects influenced our findings, since three patients with more than 15 headache days left after withdrawal performed worse on both psychological as well as cognitive functioning. Thus, response to withdrawal therapy is associated with reduction in psychological distress and improved cognitive functioning.
Psychological distress
The present findings show that ergotamine abusers scored high on the total SCL‐90 scale and most of the subscales. The high scores on the somatization subscale suggest a high level of physical symptoms, whereas high scores on the depression and anxiety subscales suggest large psychological problems in everyday life. Migraine patients scored in‐between ergotamine abusers and healthy controls. This is in agreement with earlier findings with other questionnaires in which migraine patients showed increased occurrence of depression (29–30), perceived disturbed contentment and vitality (MSEP (31)), more emotional distress (SSAP (31)) as well as a lesser sense of well‐being (PGWB (31); MOS (32); SF‐36 (33–35)) than did healthy control persons. When frequency of migraine attacks is used as measure for disease severity (35), ‘ergotamine’ headache (daily migraine‐like headache) can be seen as a very severe form of migraine with high psychological distress and low general well‐being.
Cognition
We could not objectivate impairment of cognitive functioning in ergotamine abusers. In contrast with this finding are the results of MRI investigations in the same participants during the same visit. All MRIs were scored for white matter hyperintensities (WMH; for detailed information see Bakker et al. 1999). Normal white matter (no lesion or only a single one) was found in none of the ergotamine abusers (0%; 95% C.I. = 0–26%), in four of the 12 migraine patients (33%; 95% C.I. = 9–65%) and in seven of the 12 healthy volunteers (58%; 95% C.I. = 28–65%). The mean number of WMH differed significantly between ergotamine abusers and healthy controls (
Earlier investigations in different populations suggest that WMH are related to cognitive decline (36–40). We found no correlation between cognitive functioning and severity of WMH. This lack of correlation can be explained by two factors. Firstly, earlier investigations were mostly done in subjects with hypertension or other cerebrovascular diseases instead of healthy controls. Most studies in healthy volunteers failed to find a relationship between WMH and cognitive performance (39–43). Some studies, however, found this relationship in the assessment of speed of information processing and cognitive flexibility (38–46). Secondly, none of these earlier investigations corrected cognitive performance for psychological distress. We concluded that white matter lesions in ergotamine abusers were not associated with general cognitive decline at the time of investigation.
In conclusion, ergotamine abuse in migraine patients is associated with high psychological distress but not with structural impaired cognitive functioning. Migraine patients scored in‐between ergotamine abusers and healthy volunteers. After withdrawal, psychological and cognitive functioning improved, proportional to reduction in headache frequency.
Footnotes
Acknowledgements
This study was in part financially supported by Glaxo‐Wellcome B.V., The Netherlands.