
Abstract
Sumatriptan succinate (Imitrex) is a 5-HT(5-hydroxytryptamine) agonist used for relief of migraine symptoms. Some individuals experience short-lived side-effects, including heaviness of the limbs, chest heaviness and muscle aches and pains. The effects of this drug on skeletal muscle energy metabolism were studied during short submaximal isometric exercises. We studied ATP flux from anaerobic glycolysis (An Gly), the creatine kinase reaction (CK) and oxidative phosphorylation (Ox Phos) using 31P nuclear magnetic resonance spectroscopy (31P MRS) kinetic data collected during exercise. It was found that side-effects induced acutely by injection of 6 mg sumatriptan succinate s.c. were associated with reduced oxygen storage in peripheral skeletal muscle 5–20 min after injection as demonstrated by a transient reduction in mitochondrial function at end-exercise. These results suggest that mild vasoconstriction in peripheral skeletal muscle is associated with the action of sumatriptan and is likely to be the source of the side-effects experienced by some users. Migraine with aura patients were more susceptible to this effect than migraine without aura patients.
Dysfunction of skeletal muscle mitochondria has been reported in migraine patients studied with 31P magnetic resonance spectroscopy (31P MRS) (1). Reduced mitochondrial function may render migraine patients sensitive to added perturbations of mitochondrial function. A wide range of symptoms may accompany patients with mitochondrial myopathies. These symptoms include, but are not limited to, prevalence of headache, aura or stroke-like symptoms(e.g. MELAS patients) or muscle problems (ragged red fibers, muscle pain, muscle weakness). An excellent review of the genetics and clinical morphology of mitochondrial myopathies has been previously published by others (2).
We hypothesized that worsening of an underlying skeletal muscle mitochondrial defect after injection of sumatriptan succinate (6 mg s.c.) might explain some side-effects such as muscle pains and limb heaviness. This was tested using 31P MRS to measure exercise-induced effects on muscle energy metabolism at end-exercise and mitochondrial function during recovery from exercise before and after sumatriptan injection.
Materials and methods
Subject selection
Subjects were recruited from the the Headache Clinic of the Department of
Neurology, Henry Ford Hospital. All subjects (n = 18) suffered
from migraine headaches (eight migraine with aura (MWA), 10 migraine without
aura (MwoA)), diagnosed according to the classification criteria of the IHS
(3) by a
neurologist. The mean age of the subjects was 39.9 years (
Exercise instrumentation
The exercise bench was mounted onto the patient table of a 3 T (SMIS/Magnex) MRI/MRS system. The subject's exercising leg was put through straps to isolate the calf muscle. A strap at the knee kept the leg straight during exercise in order to prevent contributions to the force from the quadriceps. A 9-cm diameter 31P inductively coupled surface coil was placed in a slot below the calf and fastened to the leg using a pair of 4.5 cm wide Velcro straps. The foot was restrained at the ankle by three 4.5 cm wide straps. The foot was anchored to a plate directly above a force transducer (Tedea model 1250(300 Kg)) that was set to an angle of 15 degrees plantar flexion for optimal force production from the calf (4). The cable to the force transducer was RF filtered using 7-pole Butterworth filters. Outside the RF screen, the cable from the RF filters was connected to a Tedea model AD-4321 output stage. The force data from the output stage was collected through an RS-232C port connected to a Pentium personal computer during exercise. This allowed the computer to generate a tone with a pitch proportional to the force reading at each time point (3–4 points/s). Feedback for the subject was provided by the computer generated tone and by a coach at the magnet.
Exercise testing protocol
Subjects performed two pre-injection isometric contractions of the calf for 90 s to a target force of 50–65% of their maximum voluntary contraction (MVC) based on maximum muscle cross-sectional area (5). Each exercise was followed by a 15-min rest period. Ten minutes after the second exercise, the subject was injected with 6 mg sumatriptan succinate s.c. Target force exercises identical to the pre-injection exercises were performed at 5 and again at 20 min after injection. Thus we measured the acute effects of sumatriptan on exercising muscle energy metabolism, using each subject as their own control.
Spectroscopic measurements
Time-resolved 31P MR spectra of the calf muscle were obtained in a 3 T whole body magnet (Magnex Scientific) using an SMIS console (Surrey, UK). Spectra were collected using the inductively coupled surface coil. Excitation was provided by a block pulse calibrated to 135 degrees at the coil centre using a tube of hexamethyl phosphorus triamide (HMPT) in the plane of the coil. This provides signals from both heads of the gastrocnemius and the soleus. Saturation factors were obtained from the ratios of peak areas of fully relaxed spectra (four averages, 30 s TR) and partially relaxed spectra (eight averages, 24 dummy pulses, 1 s TR). Spectra with 1 s time resolution were collected before, during and 5 min after the exercise. Spectra were analysed in the time domain to eliminate baseline artifacts. Metabolite peak areas were corrected for partial saturation using the measured saturation factor.
Spectral analysis
Peak positions and areas were determined by fitting the time domain (FID) data to
a series of decaying exponentials. The algorithm used for fitting the time
domain data was a Levenberg-Marquardt non-linear least squares fit to a series
of exponentially decaying sine and cosine functions in the real and imaginary
channels, respectively (6, 7) (programme courtesy of Dr
Peter Barker). The time domain data were apodized with 15 Hz exponential
multiplication before fitting. Baseline artifacts were eliminated by skipping
the first four points of the data during fitting of the FID. Observer bias was
avoided by computer fitting FIDs in batch mode and then entering the results
into a spreadsheet. Concentrations of inorganic phosphate (Pi), phosphocreatine
(PCr), phosphomonoesters (PME), and phosphodiesters (PDE) were determined using
the peak areas corrected for partial saturation and assuming that [PME] + [Pi] +
[PDE] + [PCr] + [ATP] = 40.7 m
Fitting recovery curves
Single exponential fits to the recovery of PCr, Pi, and the calculated concentration of ADP were performed using SigmaPlot (Jandel Scientific). Results are expressed as the metabolite's time constant of recovery (T.C.) in seconds (s). [ADP] was calculated as previously described (5). The resulting parameters, fits and residuals were stored in a spreadsheet (Quattro-Pro, Borland) for subsequent display (Sigmaplot, Jandel Scientific) and statistical analysis (SigmaStat, Jandel Scientific).
Energy metabolism determinations
Using a previously published model (11), the pH vs. time, Pi vs. time and PCr vs. time curves generated from the spectral analysis were used to calculate: (1) mitochondrial ATP production rates (Ox Phos); (2) the creatine kinase reaction (CK); and (3) ATP synthesized during lactate production (An Gly) at end-exercise.
Imaging measurements
Using the 31P surface coil tuned to the 1H frequency using a Gordon-Timms arrangement (8), six contiguous imaging slices were obtained from the centre of the calf. Images were obtained using a gradient recalled echo multislice imaging sequence with the following parameters: TR = 100 ms, TE = 8 ms, 200 mm field of view, six contiguous slices, 1 cm slice thickness, two averages, 256 × 192 acquisition matrix, 120 degree pulse at surface coil centre. The purpose of the images was to obtain the maximum cross-sectional area for normalization of the force data (5).
Statistics
Student's t-tests were used to compare MWA patients with MwoA patients for the continuous measurements. Student's t-tests were also used to compare results from patients with side-effects to patients with no side-effects if the assumption of equal variances was met. If the assumption of equal variances was not met, Welch's t-tests were used for comparison. Paired t-tests were used for the comparison of energy metabolism and end-exercise metabolite concentrations before and after sumatriptan injection. Fisher's exact tests were done to compare MWA patients to MwoA patients for the presence of either (1) any side-effect or (2) each specific side-effect.
Results
Side-effects were experienced by 13 of the 18 subjects studied (Table 1). These included heaviness of the limbs (n = 3), muscle pressure and tightness in the head, chest or jaw regions (n = 8), a generalized sensation of weakness (n = 5), and a sensation of increased effort on exercise (n = 2). Nausea was also experienced in four patients and headache was elicited in one.
Summary of side-effects experienced by migraine patients after sumatriptan injection
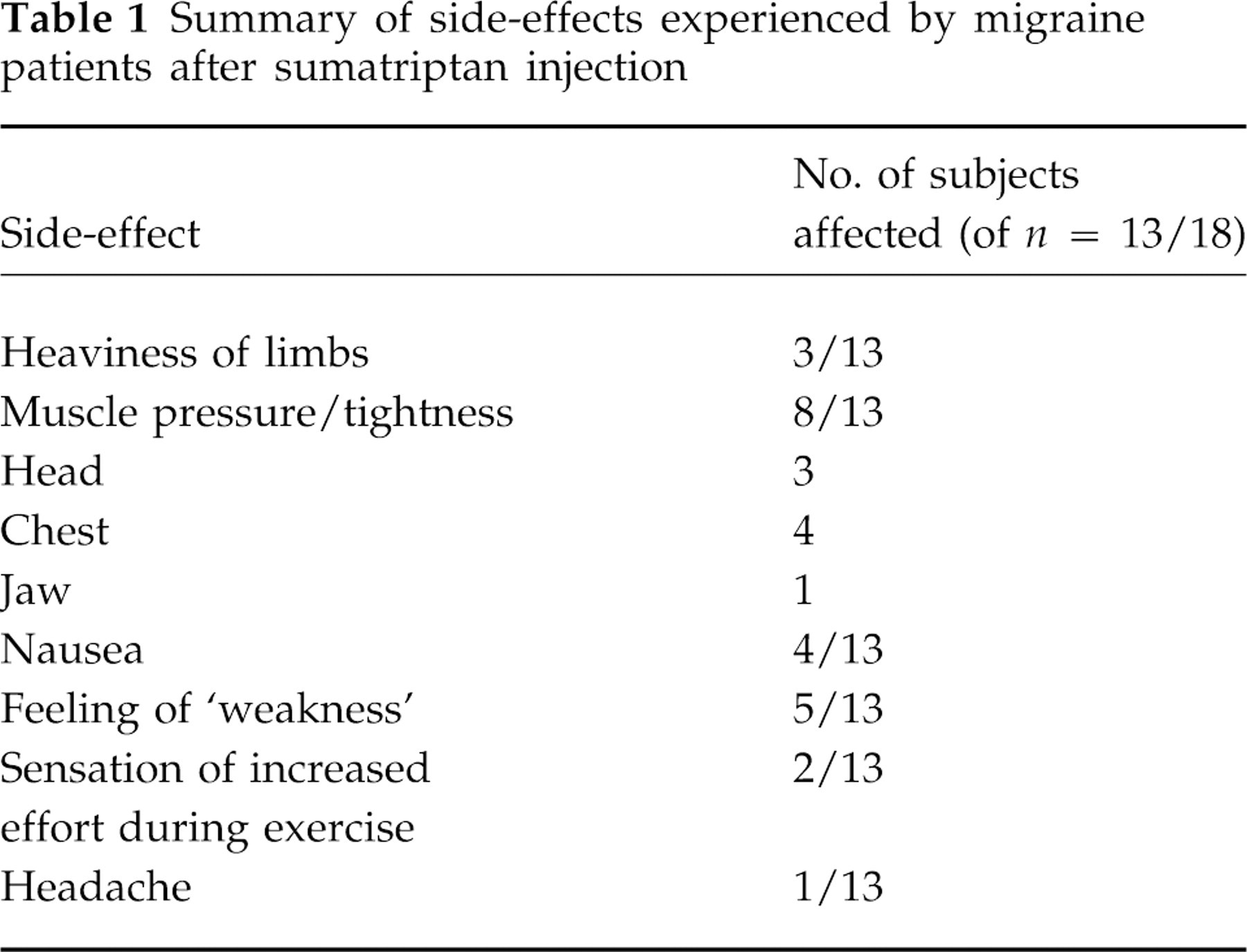
Table 2 shows the changes in energy metabolism in exercising muscle which occurred after sumatriptan. Results are the average of the two exercises before sumatriptan injection and the average of the two exercises after sumatriptan. There were no statistically significant differences between exercise 1 and exercise 2 when analysed individually using paired t-tests. This was also true between exercises 3 and 4, although a trend towards increasing PCr T.C., which indicates a slowing of the mitochondrial ATP synthesis activity, was observed going from exercise 3 to exercise 4 (P = 0.054) in all subjects combined.
Energy metabolism in migraine patients

*Statistically different (p = 0.009) from
before sumatriptan injection in a paired t-test. All
values are mean ± 1
In individuals who experienced side-effects after sumatriptan, there was a significant reduction in the initial rate of PCr recovery (Ox Phos) compared to before injection (Table 2). Table 2 also shows that there were trends towards increased ATP production rates from anaerobic sources of ATP, anaerobic glycolysis (An Gly) and the creatine kinase reaction (CK). Subjects without side-effects had no significant differences in any measure of energy metabolism after sumatriptan compared to results before injection (Table 2). Although there was a trend towards longer PCr recovery times in the patients with side-effects as compared to patients not experiencing side-effects (Table 2), the trend was not significant. Differences between these groups could be masked by the low sample size of the group with no side-effects.
A further discrimination within the group with side-effects showed that the reduction in Ox Phos was more pronounced in MWA than MwoA patients (Table 3). Although the average magnitude of the decrease in Ox Phos was similar in both groups, the change only was statistically significant in the MWA group. No other differences between the MWA and MwoA patient groups were significant, including the prevalence of side-effects and rates of energy metabolism before or after sumatriptan injection. In addition, discrimination of the group with no side-effects showed no significant differences between MWA and MwoA patients. Changes in this group could be masked by the small sample size in the group with no effects (MWA, n = 2; MwoA, n = 3).
Energy metabolism in migraine patients experiencing side-effects to sumatriptan injection

*Statistically different (p = 0.007) from
before sumatriptan injection in a paired t-test. All
values are mean ± 1
Figure 1 provides an example of PCr recovery data from one patient who experienced side-effects to sumatriptan injection. Several similarities and differences between the pre-injection exercise and the post-injection exercise are of interest. First, there was a small delay in the initial PCr recovery after injection (Fig. 1D) that decreased the initial slope during the first 10 s of recovery (Ox Phos). Second, the amount of PCr used during exercise was greater after injection, indicating a larger amount of total anaerobic metabolism. Third, the time constants to recovery were identical in both cases, indicating that mitochondrial ATP production was normal after sumatriptan injection during recovery from exercise in this patient, except during the initial 10–20 s. Some, but not all of these trends were found in the entire group of migraine patients who experienced side-effects, where none of these trends were observed in patients without side-effects.

Example of and individual's kinetic traces of PCr vs. time during recovery from exercise in a patient experiencing side-effects to an injection of 6 mg sumatriptan succinate, s.c. Before (A,C; open circles) and after (B,D; open squares) injection. Left (A,B), 5 min of recovery; Right (C,D) first 30 s of recovery. The lines through the data (points on the graph) are least squares nonlinear exponential fits of the full recovery curves.
Discussion
Isometric exercise causes the muscle to become a closed system, building up the by-products of energy metabolism necessary to support force production and depleting the supplies of nutrients, especially oxygen, PCr and substrates for mitochondrial ATP synthesis. Upon cessation of exercise, blood flow resumes and, in normal individuals, increases significantly above resting levels (reactive hyperemia). During this recovery phase, the mitochondria are supplying ATP at a rate much greater than demand, and the excess ATP generated replenishes the depleted PCr. The rate of PCr recovery is an indicator of mitochondrial turnover. Similarly, the rate of ADP recovery has also been used in many studies as an indicator of mitochondrial activity (10).
Comparison of pre-injection data obtained in this study with results from healthy controls obtained in a previous study (12) demonstrates that recovery time constants of PCr and ADP in migraine patients were similar to those of control subjects during recovery from a short, sub-maximal exercise of similar intensity. This was not in agreement with previously published results that the time constants of recovery were increased in migraine patients as compared to controls (1). The exercise and data collection protocols were different in the two studies, however.
In our study, a short, 90 s isometric exercise was used to compare results with our previous work (12). Barbirolli's lab used a longer (10–15 min) isotonic exercise protocol, which induces reactive hyperaemia, stimulating the mitochondria with greater oxygen supply, and giving the mitochondria time to be stimulated to near their maximum capacity (13). The isotonic exercise allows the muscle to transition into entirely aerobic ATP production if subjects have the mitochondrial capacity and oxygen supply from perfusion to achieve this at the final work level. Nevertheless, it remains to be determined as to how to isolate mitochondrial dysfunction from perfusion deficits using 31P MRS studies of exercise. Potentially, isotonic exercise is a metabolic condition wherein oxygen (perfusion) limited mitochondrial metabolism occurs in migraine patients, but not in controls. Alternatively, the longer exercise protocol may be demonstrating reduced mitochondrial function in migraine patients due to a reduced mitochondrial density, which may not be detected during shorter sub-maximal exercise.
Data collection conditions also differed between the two studies. This study was designed to collect signals from both the gastrocnemius and soleus muscles, both of which are involved in force production during plantar flexion. The work of Barbirolli et al. collected data primarily from the gastrocnemius (1), which is less oxidative than the soleus.
Reduction in instantaneous, but not steady state, mitochondrial function at the end of an isometric exercise was associated with the onset of side-effects to injection of 6 mg sumatriptan succinate s.c. This suggests that sumatriptan reduces muscle oxygen stores without significant reduction in the oxygen delivery to the muscle during recovery from the exercise in these subjects. Although reductions in the oxygen binding capacity of blood could produce such a result, alteration of oxygen binding capacity is unlikely in normal migraine patients. More likely, reduction in blood volume occurs in resting muscle due to minor constriction in arteries or capillaries or both. No difference between pre- and post-sumatriptan exercises were measured in patients experiencing no side-effects. Further studies on muscle perfusion rates during ischemic (isometric) exercise and monitoring of blood SAO2 in patients who develop side-effects to sumatriptan would be useful to shed further light on the physiological mechanisms involved in producing the side-effects.
Rest periods of the length we used allowed recovery of force and 31P MRS visible metabolites in longer (4 min) maximum voluntary isometric contractions (14). A careful analysis of trends in individual exercises among a series of controls, however, showed that oxidative metabolism increased slightly between the first and second exercises and again between the second and third exercises, reaching significance only between the first and third exercises (15). This trend is observed in patients without side-effects. The opposite trend was observed in the initial PCr recovery rates of patients who experienced one or more side-effects. These data suggest a relationship between reduction in oxidative metabolism and side-effects of sumatriptan, although the differences were not statistically significant in this study.
Reductions in the initial recovery kinetics with no significant reduction in recovery time constants was observed in severe chronic obstructive pulmonary disease (COPD) patients before and after they were taken off their supplemental oxygen (16). In these patients, oxygen deprivation reduced SAO2 of blood from 95% to 87%, leading to delay in initial PCr recovery without a change in PCr recovery time constant (16). This is the same result that we observed in patients reporting side-effects to sumatriptan (Table 2), suggesting that part of the effect of sumatriptan is to reduce oxygen stores, but not severely restrict muscle perfusion. One mechanism which could cause a minor reduction in muscle oxygen stores is reduced resting capillary volume. Normal recovery time constants indicate normal mitochondrial function, hence adequate oxygen delivery after exercise for normal mitochondrial function. Initial PCr recovery rate after isometric exercise is particularly sensitive to oxygen stores or minor reductions in perfusion because isometric exercise is inherently ischaemic.
The association of side-effects with reduced muscle oxygen stores provides a testable hypothesis for the source of side-effects experienced by some patients after sumatriptan. Further studies should include measurement of perfusion, oxygenation of the muscle blood pool, and distinguish the patients who experience side-effects associated with decreases in capillary volume or blood oxygen content. A combination of perfusion studies, energy metabolism studies both before and after injection, and either infrared measurements of blood oxygenation or NMR spectroscopic measurements of deoxygenated myoglobin could shed new light on the underlying mechanism(s) of side-effects caused by sumatriptan and aid in the design of therapies to counter the side-effects.
Footnotes
Acknowledgements
This work was supported by grants from Glaxo-Wellcome and NIH (P50-NS32399).