
Abstract
Keywords
The high prevalence of unawareness of illness in bipolar disorder and schizophrenia has been replicated in several studies [1–5]. Approximately one half of bipolar patients studied show deficits in their awareness of being ill and insight into specific signs and symptoms [5–7]. The International Pilot Study of Schizophrenia, a multinational and cross-cultural study conducted for the World Health Organization found that 81% of 811 patients with schizophrenia denied that they had an illness [8, 9]. One of the authors (XFA) replicated the main results of these studies finding that nearly 60% of 221 patients with schizophrenia did not think they were ill [10]. Finally, at least one type of anxiety disorder, obsessive– compulsive disorder (OCD), is commonly accompanied by poor insight into illness [11, 12]. The deficit is so common and considered to be of such clinical value that the Diagnostic and statistical manual for mental disorders, fourth edition (DSM-IV) now include an OCD subtype that hinges on illness awareness (i.e. OCD with, vs without, insight) [13].
In bipolar disorder, schizophrenia and schizoaffective disorder, lower levels of insight into illness have been found to be predictive of a poorer course of illness and non-compliance with treatment [7–14]. In schizophrenia, neurocognitive deficits involving the frontal lobes have been implicated in the aetiology of awareness deficits [15]. Whether poor insight into illness in bipolar disorder and anxiety disorders is caused, in part, by neurocognitive deficits, is as of yet unknown. Regardless of the cause, poor insight in these disorders is an important prognostic indicator and a useful dimension on which patients can be subtyped [7–16]. Another question left largely unanswered is the nature of insight in bipolar patients with comorbid anxiety disorder. Indeed, we are aware of only one study that has examined insight in patients who have both disorders [16].
Studies find that approximately 20–60% of patients with bipolar I disorder also have a comorbid anxiety disorder [16–18]. In a previous study, we have found that a comorbid diagnosis of an anxiety disorder is associated with better insight, fewer psychotic symptoms and lower risk of serious suicide attempts [16]. These results are largely consistent with the extant literature insight in psychotic disorders which shows that higher levels of insight are frequently correlated with a better outcome and course [1, 7, 10, 14]. However, in the Pini et al. study [16], we did not examine whether different types of comorbid anxiety disorders showed different associations with course variables and insight into bipolar disorder. The pathophysiology of panic disorder is thought to be different than that of other anxiety disorders [19–21] and insight into illness has been used to subtype patients with OCD but not social phobia and panic disorder [13]. Since anxiety disorders differ from each other in their phenomenology, and very likely their pathophysiology, it is reasonable to hypothesize that they may also show differences in insight.
The present study examined whether specific types of comorbid anxiety disorders are differentially associated with course variables and insight into bipolar illness. Specifically, we compared bipolar I patients with, and without, comorbid OCD, social phobia and panic disorder, to determine whether specific types of anxiety disorder were more likely to be associated with better insight.
Method
The patients in this study were recruited within the framework of the University of Pisa Comorbidity in Psychosis Project [16, 18]. For the purpose of this study, 151 consecutively hospitalized patients with bipolar I disorder were selected on the basis of the following criteria: (i) age over 16 years; (ii) presence of psychotic symptoms (i.e. formal thought disorders, delusions, hallucinations); and (iii) provision of written informed consent. Exclusion criteria were psychotic symptoms secondary to acute intoxication, withdrawal from psychotropic substances, or severe medical conditions. The inclusion diagnosis of affective psychosis was made by a senior psychiatrist not directly involved in the study. Subjects were interviewed the week before their discharge to confirm inclusion diagnosis and to assess lifetime Axis I comorbidity; the Structured Clinical Interview for DSM-III-R [22] – patient version (SCID-P) [23] was used. For the assessment of lifetime comorbidity, the SCID-P hierarchy was maintained for the psychotic disorder diagnosis; therefore, patients who met the criteria for schizophrenia or delusional disorder were excluded from the analyses. After previous training in the use of the instrument, three resident physicians interviewed patients with the SCID-P. To complete the SCID-P, information was obtained from any source available in addition to the patient interview, including medical records, first-degree relatives and treating clinicians. Syndromes clearly secondary to the principal psychotic illness were not rated as comorbid disorders by interviewers.
Level of symptomatology during the week preceding discharge was assessed using the 18-item version of the Brief Psychiatric Rating Scale (BPRS) [24]. The frequency of delusions, hallucinations and formal thought disorders was evaluated with the SCID-P. Overall judgement of patient's social and occupational functioning was obtained by the SCID-P Axis V Global Assessment of Functioning Scale (GAF) [25].
Level of insight was assessed with the Scale to assess Unawareness of Mental Disorders (SUMD) [10]. Interrater reliability among the three interviewers was assessed on nine interviews (n = 24 interviews). Cohen's Kappa agreement ranged from 0.88 and 1 for diagnosis. The intraclass coefficient correlation for the three general items of the SUMD and the total BPRS score ranged between 0.88 and 0.95.
The SUMD assesses patient's awareness of multiple domains of psychopathology. In addition to evaluating patients’ general awareness of having a mental disorder, we also evaluated awareness of response to medication, of social consequences of having a mental disorder, and awareness of three symptoms relevant for mood disorders with psychotic features: delusions, hallucinations, thought disturbances. For each dimension of insight into having a mental disorder and awareness of symptoms two scores were obtained; one assessing the current episode of illness (current awareness) and the second assessing previous episodes of illness (retrospective awareness). A more detailed discussion of our assessment of the multiple dimensions of insight appears elsewhere [6]. For the purposes of this report, the term insight will be used to encompass all of the aforementioned dimensions of insight into illness unless otherwise stated.
Statistical analyses
The χ 2 test was used to analyse categorical variables; post-hoc pairwise comparisons were performed inspecting adjusted standardized residuals. One-way analysis of variance (ANOVA) with post-hoc pairwise Tukey's multiple comparisons and ANCOVA were used to analyse continuous variables. Predictive value of anxiety comorbidity and course variables on good insight was investigated by means of a logistic regression analysis, including good insight versus poor insight as dependent variable and social anxiety and OCD comorbidity (no panic type anxiety comorbidity), duration of bipolar illness, age at onset of bipolar illness, number of hospitalizations and the total BPRS score as covariates. Statistical analyses were performed by using SPSS, Version 10.0 for Windows 98 (SPSS, Chicago, IL, USA).
Results
Of the 151 bipolar subjects, 92 had no lifetime panic disorder (PD), social phobia (SP) or OCD cormorbidity, 35 had lifetime PD and 24 had lifetime SP and/or OCD. Descriptive characteristics of the sample are shown in Table 1. No significant differences were found between bipolar patients with, versus without, comorbid anxiety disorders.
Descriptive characteristics of the sample of bipolar patients (n = 151) with, and without, comorbid anxiety disorders
First, to examine differences between groups in insight we performed an ANOVA on the first three summary items of the SUMD, both current and retrospective. Table 2 shows the results of these analyses. The three groups differed significantly on the current awareness of illness and treatment response scores (Item 1: p = 0.01; Item 2: p = 0.02) and the retrospective awareness of illness and treatment response scores (Item 1: p = 0.02; Item 2: p = 0.05). Post-hoc analyses revealed that, compared to both bipolar patients without comorbid anxiety disorders and those with comorbid panic disorder, patients with comorbid social phobia and/or OCD had better insight on current awareness of illness (p = 0.034 and p = 0.021), current awareness of treatment response (p = 0.043 and p = 0.007) and retrospective awareness of awareness of illness (p = 0.038 and p = 0.017); retrospective awareness of treatment response was better than those with comorbid panic disorder (p = 0.041).
General items SUMD scores in the three study groups
One out of the three awareness of symptom items examined was significantly different in the direction of patients, with comorbid social phobia and OCD again showing better current awareness of hallucinations than the subjects without anxiety comorbidity (Tukey test: mean difference (I-J) −1.24, p = 0.049, df = 2,64). Current and retrospective awareness of delusions and current awareness of having thought disturbances were not significantly different between groups. Retrospective awareness of having thought disturbances differed between groups in the same direction (Tukey test: mean difference (I-J) −2.27, p = 0.037, df = 2,24).
We also performed an analysis of variance (ANCOVA) for the first three summary items of the SUMD by comorbidity controlling for the effect of polarity of index episode (manic, mixed, or depressive). We found that both comorbidity and polarity of index episode were significantly predictive of insight but not the interaction between the two factors [data available from the authors].
To better examine whether the statistically significant differences were also clinically meaningful, we dichotomized patients into those with good insight (SUMD scores of 1 or 2) and poor insight (SUMD scores of 3, 4, or 5). Scores of 1 or 2 clearly reflect an understanding by the patient that s/he has a mental illness, or symptom, etc., while scores of 3, 4 and 5 indicate moderate to severe lack of awareness. Figure 1 shows the results of these analyses for the current general insight scores and for the retrospective scores.
Proportion of the sample with good insight on the Scale to assess Unawareness of Mental Disorders general awareness items. (a) Current awareness. ∗ χ 2: 6.504, df = 2, p = 0.039; ∗∗ χ 2: 9.194, df = 2, p = 0.010. □, no comorbidity; □, panic disorder; ▪, social phobia/ obsessive–compulsive disorder. (b) Retrospective awareness. ∗ χ 2: 6.296, df = 2, p = 0.043; ∗∗ χ 2: 8.225, df = 2, p = 0.016. □, no comorbidity; □, panic disorder; ▪, social phobia/ obsessive–compulsive disorder.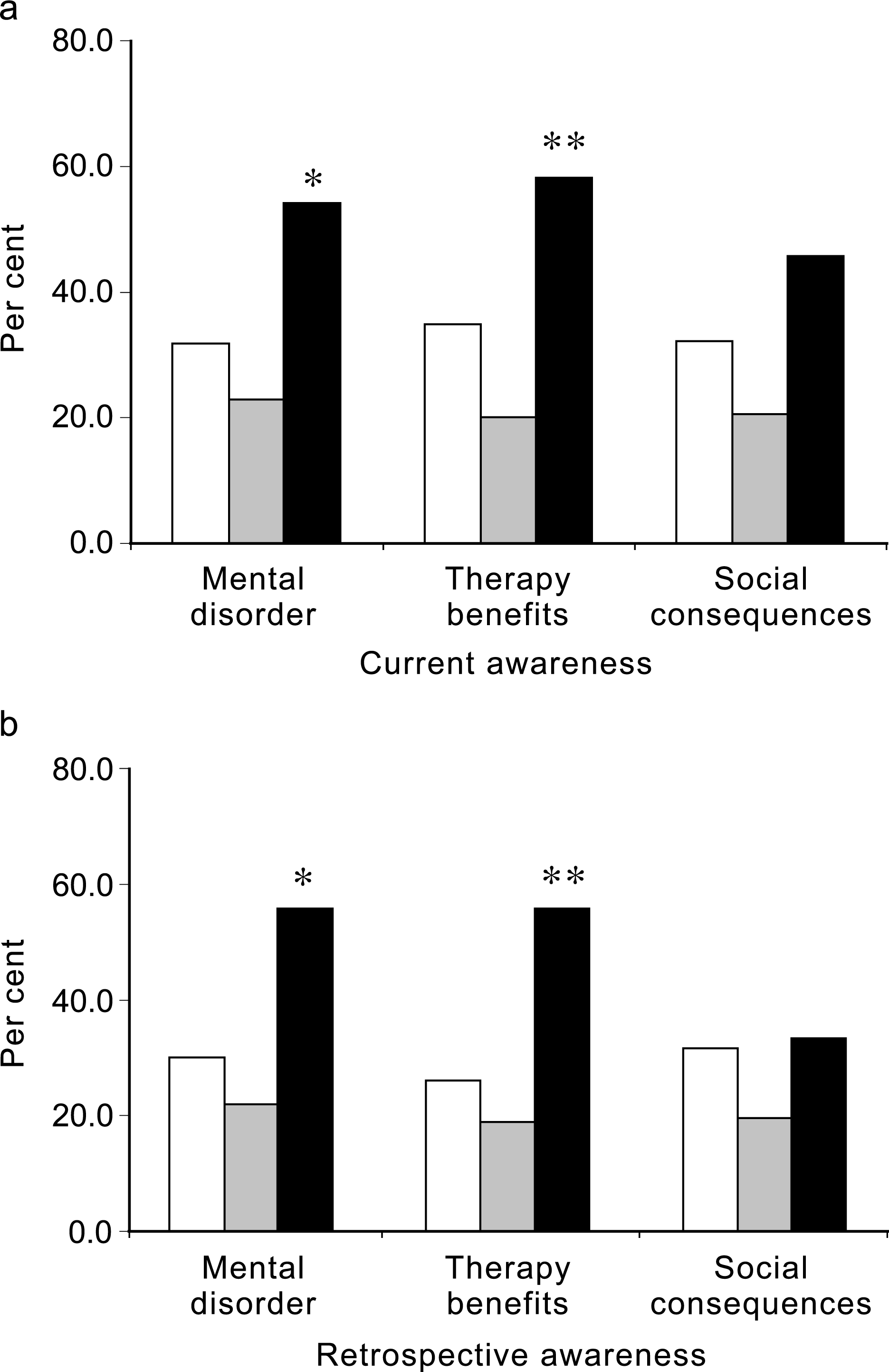
Although parametric analyses revealed few differences on the awareness of symptom items, we dichotomized these data as well as the means for the two groups that hovered around the cut-off point. Table 3 shows the results of χ 2 analyses on the awareness of symptom items. As can be seen, patients with comorbid social phobia and OCD showed good insight more often than bipolar patients with no comorbid disorders.
χ2 analyses comparing good and poor awareness of symptoms in bipolar patients with, and without, co-morbid anxiety disorders
We also wanted to see the extent to which comorbid social phobia and OCD, BPRS total score, duration of bipolar illness, number of manic episodes, and age at onset of bipolar disorder predicted good insight. Although most studies of schizophrenia do not find a link between overall severity of symptoms of the illness and insight [6, 7, 10], this hypothesis, common in clinical practice, has been studied very little in bipolar disorder. For this reason, we used the BPRS total score in the regression analyses reported below. Duration of illness and number of hospitalizations were also used because exposure to knowledge about one's illness is increased with longer duration of illness and increased interaction with mental health professionals. Finally, we have previously found an earlier age of onset of bipolar disorder in patients with comorbid anxiety disorder [16] with the onset of the concomitant anxiety disorder antecedent. Table 4 shows the results of these analyses.
Results of logistic regression analysis examining predictors of good insight
Discussion
This study replicates and extends our previous finding that comorbid anxiety disorders are associated with higher levels of insight into bipolar disorder [16]. In this study we found that patients with comorbid social phobia and OCD had better insight than those with panic disorder adding to the growing body of literature indicating the value of identifying comorbid anxiety disorders in patients with bipolar illness. We also found that the number of manic episodes and number of hospitalizations was lower in the bipolar patients with social phobia and OCD. This was not the case in the group with comorbid panic disorder. These data also suggest that specification of the type of anxiety disorder comorbidity may be especially valuable in patients with bipolar disorder.
In some disorders, insight has been used as a dimension on which patients can be subtyped [7–13]. Similarly, specific anxiety disorders have been described that are distinguished phenomenologically and in terms of various diagnostic validators such as course of illness and treatment response. Further research is needed to clarify whether bipolar disorder with comorbid social phobia and\or OCD, with good insight, has similar value as a subtype of bipolar disorder.
In general, it is reasonable to expect that the presence of an anxiety disorder would result in a poorer course and increased admissions to the hospital. From this perspective, bipolar patients with comorbid social phobia and\or OCD should have had more, rather than less, episodes of mania and number of admissions. However, in schizophrenia and affective disorders, we know that higher levels of insight into illness almost always bode well for clinical outcome and long-term course of illness [26–29]. In this context it is not surprising that the bipolar patients with comorbid social phobia and OCD, who had the best insight overall, were hospitalized less often and had fewer manic episodes. In light of this finding, we decided to examine whether these patients also differed from the bipolar patients with comorbid panic disorder. In fact, we found that compared to the good insight social phobia/OCD patients, the bipolar patients with comorbid panic disorder had significantly more episodes of mania (t = 2.03, df = 1,35, p < 0.05). The results of this post-hoc analysis suggest that perhaps bipolar patients with panic disorder differ in more ways than one from those with comorbid social phobia and/or OCD. These data beg the question: why do patients with comorbid panic disorder have worse insight than those with other anxiety disorders? We found (not reported here) that the bipolar patients with comorbid panic disorder somatized significantly more than those with comorbid social phobia and/or OCD. Perhaps this more extreme focus on physical illness inhibited their ability to see the ways in which they suffered from a mental illness.
We could not examine whether comorbid anxiety disorders were merely correlated with, or in some way influencing, the level of insight. Nevertheless, it is noteworthy that the absence of anxiety in patients with schizophrenia spectrum disorders has also been found to be correlated with lower levels of insight [7, Amador et al. unpublished data]. Taken together with the results reported here, one could argue that at least some forms of anxiety may play a role in the development of awareness of having an illness. The results of the regression analyses are consistent with this proposition. Only the presence of a comorbid anxiety disorder (social phobia and OCD), and not overall severity of illness and exposure to education about the illness, predicted higher levels of insight into having an illness and having responded to treatment.
The results are also consistent with the proposition that in many patients with psychotic disorders deficits in awareness of illness are trait-related, rather than associated with state factors such as overall symptomatology [30]. In particular, the regression analyses revealed that lifetime diagnoses of social phobia and/or OCD, and not overall symptom severity when evaluated, was the best predictor of good insight while a lifetime diagnosis of panic disorder was not. It is noteworthy that not all patients with comorbid social phobia and/or OCD met criteria for the disorder at the time they were evaluated for this study and yet the lifetime diagnosis, a trait variable in these patients, predicted better insight.
Among the limitations of this study was our inability to directly examine the relations between level of insight and symptoms of mania and trait psychoticism. These dimensions have been hypothesized, by some investigators, to be related to insight. Future studies could examine this question and the temporal stability of insight in bipolar disorder more directly by assessing such symptoms and the stability of insight over time. An additional limitation is that our sample is skewed toward the severe/psychotic end of the bipolar spectrum. Therefore, our data can not be generalized to bipolar I patients at large.
One could argue that our results are consistent with nosological conceptualizations of anxiety and affective illness lying on a continuum with significant overlap in symptomatology. Under this model, the results could be interpreted as evidence of discrete disorders within the bipolar spectrum, one that is characterized by, among other things, social phobia and/or OCD with good insight, another characterized by panic disorder with poor insight. Regardless, the results need replication and future studies should better characterize the severity of anxiety, depressive and manic symptoms over time, to answer the question of whether some forms of pathological anxiety play an important role in the development of insight. There are increasing attempts to understand the implications of insight. Some recent efforts in clinical research and treatment have placed increasing emphasis on actively educating the patient about his illness [31]. The understanding of interventions seems likely to be most accurate and the interventions most helpful if the many aspects of insight are considered and dealt with specifically