
Abstract
The concept of melancholia or endogenous depression has a long history in psychiatry, and is closely related to the classification debate as to whether depression is best conceptualized as a unitary or binary disorder [1]. When DSM-IV was introduced, there was debate as to whether the episode specifier ‘with melancholia’ should be retained or discarded. Rush and Weissenburger reviewed empirical research on melancholia, in relationship to clinical features, treatment response, neuroendocrine markers, sleep disturbance, consistency across depressive episodes, family history and course of illness [2]. Although the reviewed data contained many inconsistencies, it was considered that the melancholic specifier should be retained, and that more research on this subtype was indicated.
Since the introduction of DSM-IV in 1994, some of the key new work on melancholia has come from Gordon Parker and the Sydney Mood Disorders Unit [3–7]. Parker considers that the essential feature of melancholic depression is psychomotor disturbance, and has developed the CORE measure which has scales of non-interactiveness, retardation and agitation [3, 6]. Parker thus refers to melancholia as a disorder of movement and mood [6]. Outside of the Sydney group, we are not aware of attempts to validate the CORE construct of melancholia, or to compare it with the DSM-IV criteria.
In this paper we report on the diagnostic reliability of the CORE measure and compare CORE and DSM-IV constructs of melancholia. Against each definition of melancholia we test the hypotheses that melancholic depression is associated with less childhood adversity, less personality dysfunction, less anxiety disorder comorbidity, a greater family history loading of affective disorder, greater neuroendocrine dysfunction, and a better treatment response to a tricyclic antidepressant (nortriptyline) than to a selective serotonin re-uptake inhibitor (fluoxetine).
Method
Details about the characteristics of the depressed patients, assessment, treatment and outcome are reported in the accompanying paper (Joyce et al. [8]). Only methodological issues additional to those described and relevant to this paper will be expanded upon.
Assessment of melancholia
When depressed patients reported for their afternoon research assessment, and after giving consent, they were seen by both their treating psychiatrist or psychiatric registrar, and the research nurse (RMA) who has 18 years of clinical research experience with patients suffering from affective disorders. The psychiatrist completed the Structured Clinical Interview for DSM-III–R (SCID) [9], the expanded 27 item Hamilton Depression Rating Scale (HDRS) [10], and the Montgomery Asberg Depression Rating Scale (MADRS) [11]. Both the psychiatrist and the research nurse independently rated the patient on the CORE mental state examination [7]. The CORE is an 18-item scale, from which measures of non-interactiveness (possible range 0–18), retardation (possible range 0–21), agitation (possible range 0–15) and total CORE score (possible range 0–54) are obtained. Parker [7] has suggested that a total CORE score of 8 or more defines melancholia.
Neuroendocrine assessment
Prior to patients attending for their afternoon research assessment at 13.00 hours, patients were requested to have a light breakfast and to fast from 10.30 hours. After 10.30 hours they were also requested to refrain from tea, coffee and other such drinks. After arrival at the clinical research unit (CRU), patients were seated comfortably in a reclining chair, and an indwelling intravenous catheter was inserted into an antecubital vein. Baseline blood samples were drawn for routine biochemical (glucose, liver function, renal function, lipids and plasma proteins) and haematological (blood count, folate, vitamin B12) measures.
Further blood samples were drawn at 15-minute intervals, until 15.00 hours, for the measurement of hormone levels. Following the 15.00 hour blood sample, 400 mg thyrotropin-releasing hormone (TRH) was infused intravenously over 1–2 minutes. Further blood samples were obtained 15 and 30 min after the TRH infusion. Blood samples were centrifuged, and plasma was frozen and stored for later hormone measurement.
Cortisol was measured by an enzyme-linked immunosorbent assay [12], ACTH, by immunoradiometric assay using a commercially available kit (Nichols Institute; coefficients of variation 3.0% [intra-assay] and 7.8% [interassay] sensitivity at 0.7 pmol/L), AVP by radioimmunoassay after acetonitrile extraction (coefficients of variation 9.7% [intra-assay] and 10.8% [interassay] and detection limit 0.3 pmol/L) [13], and CRH by radioimmunoassay [14]. Serum TSH was measured by radioimmunoassay (‘low-sensitivity’ TSH), standardized against the World Health Organization standard (coefficients of variation: 5.3% at 3.39 mU/L and 7.8% at 76 mU/L).
The mean afternoon cortisol level was obtained by averaging the seven cortisol levels obtained prior to 15.00 hours. Previous research has found that a mean afternoon cortisol level correlates highly with 24 h level cortisol production [15]. Mean afternoon CRF, ACTH and AVP levels were also calculated in a similar way. Delta TSH was calculated by subtracting the 15.00 hour (pre-TRH) TSH level from the peak TSH level 15 or 30 min after the TRH infusion.
Data management and statistical analyses
All data was entered into the relational database PARADOX, and transferred to SYSTAT for statistical analyses including descriptive statistics, analysis of variance, Pearson correlations, t-tests, kappa and chi squared tests.
Results
Of the 195 depressed outpatients in this study, 44% (86) met the DSM-IV criteria for melancholia. Furthermore, 16% (32) had two criteria in excess of that required to meet the DSM-IV melancholic criteria, and are identified as a severe melancholic group.
In this study all patients were assessed on the CORE by one research nurse (CORE total 9.3 (± 5.4)) and by one of 10 psychiatrists or senior psychiatric registrars (CORE total 10.2 [± 5.6]). Sixty percent (116) scored eight or more on the CORE as rated by the nurse, and 20% (39) scored 14 or more on the CORE. These represent a broadly and narrowly defined CORE melancholic group.
Interrater and diagnostic reliability
The Pearson correlation between the research nurse and the psychiatrist for the total CORE score was 0.61; although the correlation of the nurse with the three psychiatrists (PRJ, RJM, SEL) who rated most patients (n = 112) was 0.70. Despite the satisfactory interrater reliability on a dimensional CORE score, if the score is dichotomised at a cut point of 8, then the kappa for agreement for a diagnosis of melancholia between the psychiatrists and the nurse with the CORE is only 0.35.
Of the 195 patients, 44% (86) met the DSM-IV criteria for melancholia, 60% (116) met the CORE criteria for melancholia, 29% (57) met both sets of melancholic criteria, and 26% (50) met neither criteria for melancholia. The kappa value for agreement between the two diagnostic systems is only 0.11. At best therefore, CORE melancholia and DSM-IV melancholia are only partially overlapping constructs.
The effect of age and gender on psychomotor measures
Of the three subscales of the CORE, only agitation correlated with age (r = 0.24, p = 0.001). Non-interactiveness by contrast had a zero correlation with age. However, there were marked differences on the CORE by gender, with males having significantly higher scores than females; (non-interactiveness M 4.2 [± 2.3] vs F 3.0 [± 2.0] [t = 3.88, p < 0.001]; retardation M 5.7 [± 3.2] vs F 3.9 [± 2.7] [t = 4.21, p < 0.001]; agitation M 1.4 [± 1.5] vs F 0.8 [± 1.0] [t = 3.36, p = 0.001]).
Validating DSM and CORE constructs of melancholia with developmental and clinical variables
Table 1 divides the sample into three discrete groups using DSM-IV melancholic criteria; not melancholia (DNON), melancholia (DM) and severe melancholia (DSM). From Table 1 it can be seen that these three groups differ significantly as regards depression severity (whether measured by MADRS or HDRS), but in no other way. Thus, the DSM-IV melancholic patients do not report a greater family history of depression, poorer childhood environments, and do not have lower rates of comorbid axis I or axis II disorders.
Childhood risk factors, family history, anxiety disorder comorbidity andpersonality disorder in DSM-IV melancholia
Table 2 divides the sample into three distinct groups using the CORE measure; not melancholia (CNON), broad melancholia (CBM) (CORE score 8–13), and narrow melancholia (CNM) (CORE score ≥ 14). Like the DSM-IV construct, CORE-defined melancholic patients have more severe depressions. There are also important gender differences in CORE defined groups, such as males make up 25% of the non-melancholic group but 69% of the narrow melancholic group. These results are consistent with the males being rated as having more psychomotor disturbance on the CORE. The other two statistically significant findings are in the opposite direction to that hypothesized by some writers, that the melancholic patients have higher rates of comorbid obsessive compulsive disorder and of avoidant personality disorder.
Childhood risk factors, family history, anxiety disorder comorbidityand personality disorder in CORE melancholia
Thus, neither the DSM-IV nor the CORE definitions of melancholia are associated with less anxiety disorder comorbidity, less personality disorder comorbidity, less abnormal childhood experiences or more family history of depression in first degree relatives.
Neuroendocrine measures as validators of melancholia
Table 3 shows the relationships between mean afternoon cortisol levels, the TSH response to TRH challenge and the DSM and CORE constructs of melancholia. Neither DSM melancholia nor DSM severe melancholia differed from the DSM-non-melancholia patients with regards to measures on the hypothalamic-pituitary-adrenal or thyroid axes.
Neuroendocrine measures in DSM-IV and CORE melancholia
However, the CORE melancholic criteria were validated against both the adrenal and thyroid axis measures. In the whole sample the TSH response to TRH challenge was blunted in the CORE melancholic patients. However, as men have significantly lower TSH responses to TRH than women, the lower portion of Table 3 shows the data for males only; this shows that TSH blunting is associated with a broad concept of melancholia. Similarly, with the hypothalamic-pituitaryadrenal axis, a broad CORE definition of melancholia identifies patients with higher afternoon cortisol levels.
As we had arginine vasopressin (AVP), ACTH and corticotropin releasing hormone (CRH) mean afternoon levels on a subsample of these patients, we examined the correlation of these neurohormones with the CORE measures. Neither AVP nor ACTH levels approached any significant correlations with CORE; however, CRH levels correlated 0.34 (p = 0.01) with non-interactiveness, 0.22 (ns) with retardation, 0.05 (ns) with agitation and 0.28 (p < 0.05) with total CORE score, in the subsample of 56 patients. In 24 male patients the correlation of CRH with non-interactiveness was 0.41 (p < 0.05).
Differential antidepressant response
Using intention to treat analysis, Table 4 shows the percentage of patients who meet criteria for response (≥ 60% improvement on MADRS after 6 weeks) or recovery (sustained global improvement of much improved or very much improved for at least 2 months). When patients are classified by DSM-IV melancholic criteria, there is no suggestion that those with melancholia or severe melancholia have a superior response to nortriptyline; indeed the trends all favour fluoxetine. In the DSM-IV non-melancholic group fluoxetine has superior response and recovery rates, but this is largely explained by those with atypical depression (see Joyce et al. this issue [8]).
Response and recovery rates by melancholia status and drug
Table 4 also shows antidepressant response by CORE-defined melancholia. In the non-melancholia group fluoxetine produces superior response and recovery rates. In the broad melancholia group (CORE 8–13) fluoxetine and nortriptyline appear comparable, but contrary to hypothesis, in the narrow melancholia group (CORE ≥ 14) fluoxetine trends towards superiority over nortriptyline on response rate and is significantly superior to nortriptyline as regards recovery rates. Recovery rates by drug and CORE melancholia are also shown in Fig. 1.
Recovery rates by CORE melancholia groupings and drug. F, fluroxetine; N, nortriptyline.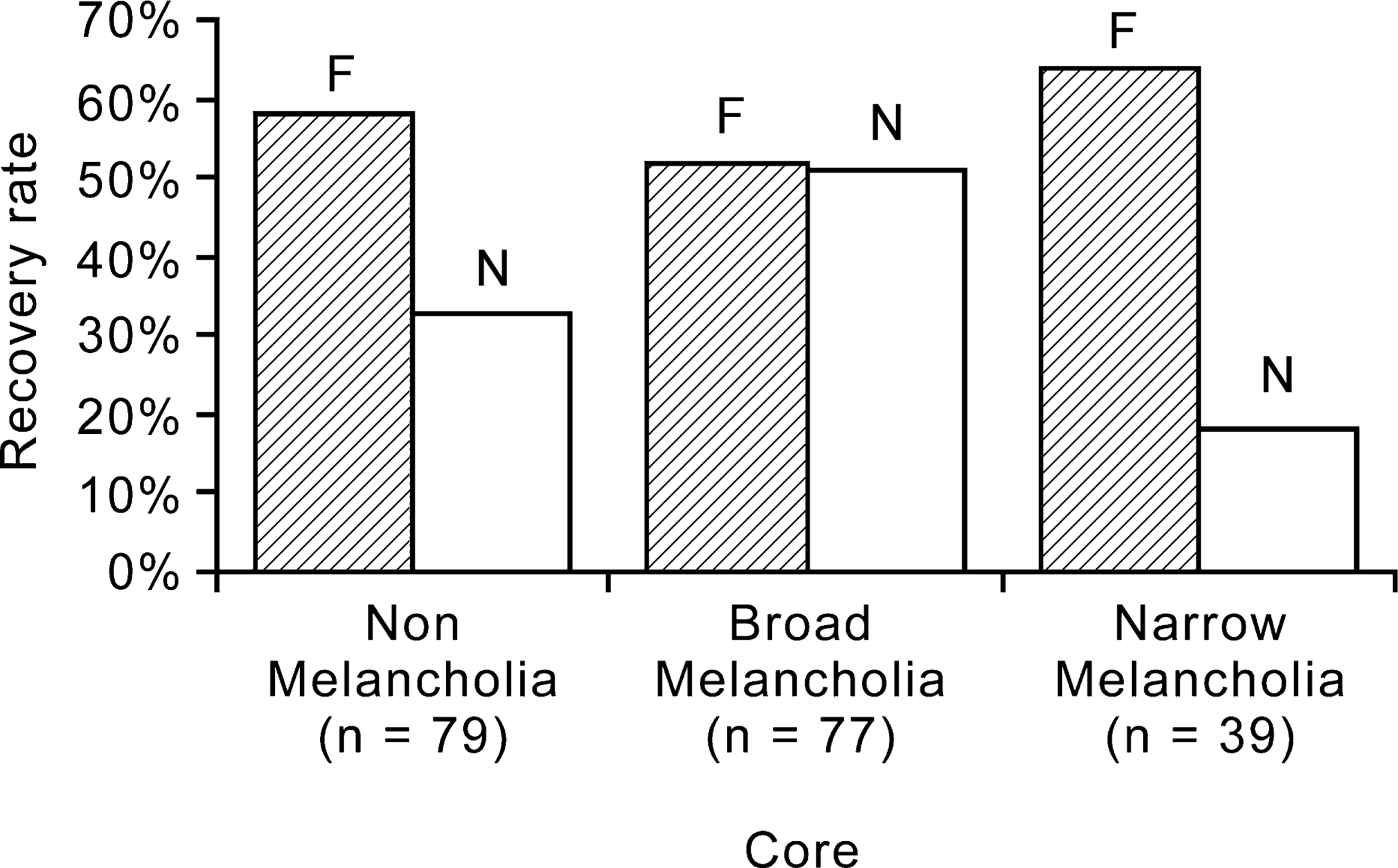
Discussion
The CORE mental state examination has been a useful additional measure for research into the phenomenology and functional psychopathology of depressive disorders. In this study we have shown that the CORE has satisfactory interrater reliability when used as a dimensional measure. However, when we dichotomised the CORE total score with a cut point of 8, the kappa statistic of 0.35 suggests that the interrater reliability of defining a melancholic category is too low for the measure to be useful for categorical diagnosis of a melancholic subtype.
In this study the interrater reliability of the CORE was probably enhanced by two clinicians seeing the patient at the same time, rather than in separate interviews. Also, in this study the time of the day of the assessment was standardized (13.00–15.00 hours). In clinical practice, when patients could be seen at any time of the day, and when many may be partially treated (rather than drug-free) when assessed, there would be additional concerns that the CORE is not an appropriate measure for usual clinical practice on which to make a diagnosis of melancholia. In this study a cut point of 8 on the CORE defined 60% of these young outpatients with depression as having melancholia. The DSM-IV definition of melancholia defined 44% as meeting criteria, and fully 74% of these patients meet either the CORE or DSM-IV criteria for melancholia. Furthermore, the agreement between the CORE construct of melancholia and the DSM-IV definition of melancholia was minimal (kappa = 0.11), which suggests that the optimal criteria for defining melancholia are far from resolved. This is not confined to the development of the CORE, as in many other studies when varying definitions of melancholia or endogenous depression have been examined within one study, the overlap between definitions has usually been less than wished for [16–18]. This lack of agreement on the optimal criteria for defining melancholia limits the utility of the concept as a depressive episode specifier or subtype.
Neither DSM-IV nor CORE melancholic criteria identified a group of depressed patients with less abnormal developmental histories or with less personality psychopathology. Previously we have reported that deficient parental care, as assessed with the Parental Bonding Instrument [19, 20], is related to personality dysfunction but not depression subtype [21]. This analysis extends that finding, and now includes that CORE defined melancholia is not associated with more normal parental care. Only Parker [20] has found that melancholic or endogenous depressed patients report having received superior parental care compared with non-melancholic depressed patients. Similarly, reported childhood physical and sexual abuse were not associated with nonmelancholic depression. The melancholic depressives, whether defined by CORE or DSM-IV, did not have lower rates of anxiety disorder comorbidity or of personality disorder comorbidity.
When the CORE and DSM-IV constructs of melancholia were assessed against neuroendocrine measures, then CORE did, but DSM-IV did not, identify a group of patients with greater neuroendocrine dysfunction. Our findings with mean afternoon cortisol levels, are very comparable with the findings of Mitchell et al. [22] who found a positive relationship between CORE measures and postdexamethasone cortisol levels. Our findings also suggest that the blunted TSH response to TRH challenge is also associated with CORE-defined melancholia. Within the CORE, the strongest associations of these neuroendocrine measures was non-interactiveness, rather than the more traditional measures of psychomotor retardation or agitation. Also, within the hypothalamic-pituitaryadrenal axis, the correlation of non-interactiveness was strongest with CRH, weaker with cortisol, but did not correlate with ACTH or AVP. Given the association of CRH with non-interactiveness it is relevant to note the animal literature on the behavioural effects of CRH, which are dependent both on the dose and the environment in which CRH is administered. While in a familiar environment, CRH increases motor activity, in an unfamiliar environment and at higher doses it produces a dramatic decrease in motor activity [23].
DSM-IV melancholic criteria did not define a group of patients for whom the tricyclic antidepressant nortriptyline was superior to fluoxetine. However, with the CORE, interesting but unexpected results emerged. At an intermediate level of melancholic symptoms, nortriptyline and fluoxetine were comparable, but at either low levels of psychomotor disturbance or at very high levels of psychomotor disturbance fluoxetine was superior to nortriptyline. Indeed, the most surprising result was that in the 20% of most narrowly defined CORE melancholic patients, the recovery rate was 64% with fluoxetine, but only 18% with nortriptyline.
One notable difference between our study and other studies on SSRIs and TCAs in melancholia is that our sample consists of younger outpatients, while others typically have older melancholic inpatient samples [24, 25]. This suggests two possibilities to explain the discrepant findings. First, age itself could be a key factor. For instance it is now relatively clear that tricyclic antidepressants (except clomipramine) do not work in adolescent depression, but SSRIs do work [26]. Perhaps during the middle adult years SSRIs and TCAs are comparable, but in older patients TCAs have advantages which are especially notable in older melancholic patients. Another possibility is that a clinical syndrome of melancholia arises through different aetiological pathways. In younger patients, greater genetic vulnerability may be the key risk factor for melancholic depression, but in older melancholic patients vascular risk factors assume greater importance [27–29]. In depressions associated with vascular risk factors TCAs could be superior to SSRIs. Indeed in poststroke depression the only study of a tricyclic (nortriptyline) versus an SSRI (fluoxetine) found that nortriptyline was superior to fluoxetine and placebo, while fluoxetine was not superior to placebo [30]. If this type of explanation is correct then we will need to move away from thinking about optimal treatments based on a symptom-defined syndrome, and think of optimal treatments in relationship to the age of the brain, or in relationship to genetic or vascular risk factors.
The results from this paper suggest that fluoxetine is approximately equally effective across all ranges of CORE defined melancholia, but that nortriptyline is less effective in both low and high CORE depressions, and most effective in those with intermediate CORE scores. These results are consistent with a review written by Joyce and Paykel [31] in which it was concluded that the best response to tricyclic antidepressant is seen in patients with intermediate levels of severity and endogeneity.
In this study, the only consistent correlate of melancholia across both DSM-IV and CORE was severity of depression. Most other studies have also found this relationship, and questions have been asked as to whether or not the key issue is severity rather than endogeneity or melancholia [18, 32]. Kendler [33] in a population-based twin study, found that melancholic major depression is a quantitatively more severe form of depression, but is not aetiologically distinct from-non-melancholic depression.
The data in this paper, both with regards to severity and also the absence of difference in psychosocial and developmental risk factors, are consistent with the results of Kendler.
All studies have their strengths and weaknesses. While we did assess the interrater reliability of the CORE measure, and utilized the ratings of the research nurse who assessed all but four of the patients, we did not examine the interrater reliability of clinicians assessing the DSM-IV criteria. However, as we utilized both the DSM-IV criteria plus more stringent criteria requiring at least two further symptoms, and as the severe melancholic group did not differ, the results are unlikely to be biased in any particular way. While the patients were randomised to one or the other antidepressant, treatment was not double-blind. However, we consider it unlikely that this introduced bias in showing a differential response to the two antidepressants in some subgroups but not in others, especially as the CORE rating utilized was not the clinician's but the nurse's assessment.
Melancholia has a distinguished history in psychiatry, but the validity of current definitions remains contentious. The DSM-IV and CORE constructs of melancholia show remarkably little overlap, and 74% of our patients meet criteria for melancholia by one or both systems. The key aspect, which is consistent across both definitions, is that melancholic depression is more severe. Otherwise, the DSM-IV criteria were not validated by psychosocial or developmental history differences, patterns of comorbidity, treatment response or by neuroendocrine markers. In contrast the CORE construct of melancholia was validated by an anticipated association with neuroendocrine dysfunction, and by an unexpected differential antidepressant response and recovery rate. The non-interactiveness scale of the CORE was especially related to the neuroendocrine disturbance, and utilized dimensionally should be evaluated further in attempts to dissect a psychopathology of depression.
Acknowledgements
The Clinical Research Unit is supported by the University of Otago, the Mental Health Division of the Canterbury District Health Board, and receives a Health Research Council of New Zealand Programme Grant.
We thank the patients who participated and the clinicians who referred patients or who were involved in assessment and treatment.