
Abstract
Polydipsia and water intoxication remains a continuing problem in a significant minority of mentally-ill patients [1, 2]. The condition is often difficult to manage, prevents discharge and has a high mortality [3]. The aetiology and mechanisms involved are ill-understood. However, polydipsia has been variously considered as secondary to positive symptoms, as a form of compulsive or manneristic behaviour, a means of stress reduction, a disturbance of homeostatic mechanisms, or secondary to medication side-effects (e.g. dry mouth). Traditional neuroleptics have been implicated as causative and considered curative [4]. Recent case reports suggest that atypical antipsychotics, particularly clozapine, may improve outcome [1, 5]. However, few studies have investigated the use of risperidone and olanzapine in the management of polydipsia and the results have been inconclusive [6, 7]. Further, despite the importance of angiotensin to water homeostasis [8], no study has examined the possible effects of drugs that act directly on this system. We report the impact of these atypical antipsychotic agents and of irbesartan (a novel angiotensin-II receptor blocking drug) in a patient with severe polydipsia.
Case report
Mr A was a 42-year-old man with a history of paranoid schizophrenia since the age of 18. He was first hospitalized at age 24 with worsening persecutory ideas, auditory hallucinations, thought disorder, lowered mood and irritability accompanied by verbal abuse directed towards his parents. Excessive fluid consumption was noted 8 years after Mr A's illness began, which could not be attributed to his mental state. He was treated with modecate 50 mg fortnightly and a tricyclic antidepressant. Polydipsia escalated over the subsequent 6 months. He was hospitalized because of marked deterioration in his physical state related to consumption of up to 20 L of cola soft drink daily. Attempts to discharge him to community care were unsuccessful because of persistent polydipsia. He was managed in a long-stay psychiatric hospital for most of the 12 years prior to his transfer to our inpatient intensive rehabilitation facility.
Mr A developed essential hypertension in his early thirties. Extensive investigations were undertaken to rule out secondary causes of hypertension and to screen for potential causes of polydipsia. A series of acetylcholinesterase (ACE) inhibitors (enalapril, captopril and perindopril) inadequately controlled his hypertension and appeared to have no significant effect on the severity of his polydipsia. His hypertension was subsequently managed with a combination of amlodipine 20 mg/day and perindopril 8 mg/day. Mr A's drinking behaviour, however, proved difficult to manage. Low serum sodium and osmolality levels were often associated with irritability and argumentativeness. He also suffered a number of seizures secondary to his excessive drinking, requiring emergency treatment. At the inpatient intensive rehabilitation facility, trials of atypical antipsychotic medications and a rigorous behavioural management programme were implemented. The latter included seclusion of Mr A from fluid sources if his weight increased more than 3.5 kg above an early morning base weight during the day.
Case progress
Figure 1 displays the monthly seclusion rates and the average diurnal weight change over a 34-month period of operation of the program. In the months prior to the period of observation Mr A had continued treatment of fortnightly doses of 100 mg fluphenazine decanoate IM. He continued to have psychotic symptoms, though specific delusions driving his drinking behaviour were not elicited. Polydipsic behaviour was severe despite behavioural intervention. Serum sodium was measured as low as 112 mmol during this period. At least one seizure required emergency medical intervention.
Monthly seclusion rates as number of episodes of greater than 3.5 kg weight gain (♦) and average diurnal weight change (▴) of polydipsic patient.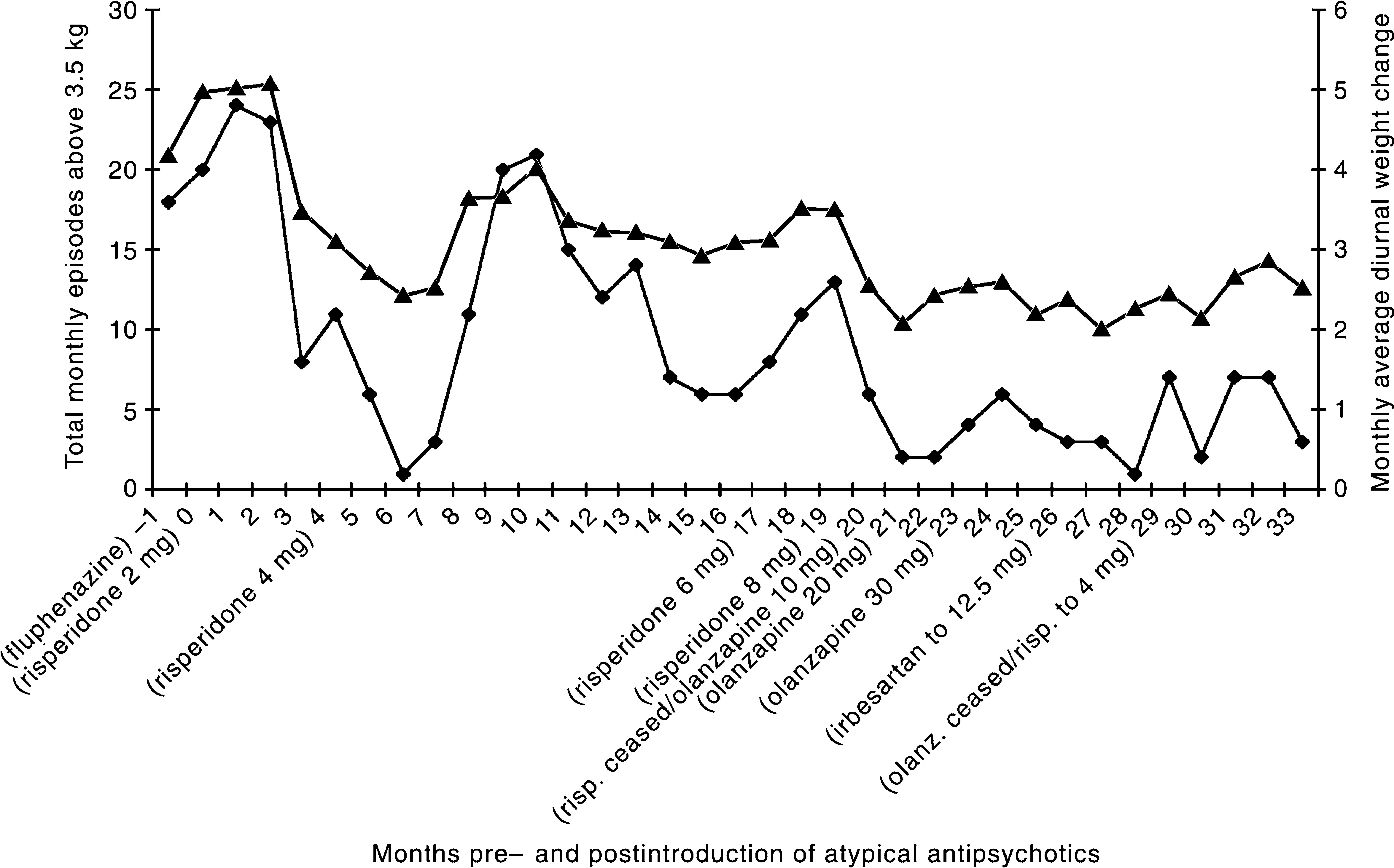
Clozapine treatment was precluded because of previous history of neutropenia on carbamazepine. Fluphenazine was discontinued and Mr A was commenced on 2 mg risperidone per day with mild improvement in his psychosis, but no noticeable improvement in his polydipsia. An increased dose of risperidone to 4 mg per day 3 months later led to further improvement in his psychosis and a marked improvement in Mr A's waterseeking and drinking behaviour. Diurnal weight change reduced, with marked reduction in periods of seclusion. Normalization of the early morning and mid-afternoon serum sodium and osmolality measures confirmed the clinical impression. These improvements on 4 mg risperidone were maintained over a 4-month period. However, an unexpected deterioration in his mental state followed, with periods of paranoid delusions about staff and other patients, increased irritability, absconding and increased polydipsia over 6 months. The polydipsia gradually reduced in the following 3 months, but his mental state did not improve. Risperidone was then increased to 6 mg and then to 8 mg daily. There was a moderate, but unsustained, mental state improvement with the increase in risperidone; but polydipsia worsened.
Risperidone was ceased and Mr A was commenced on a trial of olanzapine (at month 20; see Fig. 1), which was gradually increased to 30 mg daily. There was little change in Mr A's mental state but the average diurnal weight change seemed more stable. At the beginning of month 26, irbesartan was added to the olanzapine as a novel adjunctive treatment of his polydipsia, and replacing his previous antihypertensive treatment. Over the subsequent 3 months there was reduced polydipsic behaviour and a reduction of seclusions. However, because olanzapine had made little impact on his persecutory delusions, which were associated with irritability and argumentativeness, olanzapine was discontinued and Mr A was recommenced on 4 mg risperidone. Irbesartan was continued in conjunction with risperidone and his polydipsia remained relatively low but became more unstable.
Discussion
In this case report we investigated the effects of the novel atypical antipsychotics, risperidone and olanzapine, as possible treatments for severe polydipsia in a patient with schizophrenia. The introduction of risperidone significantly ameliorated the symptoms and behaviours associated with polydipsia in the first 6 months of treatment. However, this response was not subsequently sustained. Further increases in dose of risperidone were associated with a further deterioration suggesting that this beneficial effect may only be observed at lower doses. A change to olanzapine was associated with a sustained stabilization in weight and reduction in the number of seclusions required. The addition of irbesartan appeared to further reduce polydipsia in this man. Reintroduction of risperidone resulted in a mild destabilization of his polydipsia, perhaps ameliorated by adjunctive irbesartan.
It is unlikely that Mr A's mental state accounted for the effect on his polydipsic behaviour. Psychotic symptoms were not implicated in driving his excessive drinking. Our observations suggested that low-dose risperidone was initially helpful in improving his mental state, while higher doses of risperidone were less successful. In contrast, olanzapine was associated with stabilization of polydipsia, but had minimal impact on his psychotic symptoms. Thus, there was a dissociation between clinical state and drinking behaviour during the study period.
Recent literature on the use of atypical antipsychotics in the management of polydipsia has generally been in the form of case reports and small prospective studies. Clozapine has been shown to be effective in managing polydipsia and hyponatraemia in patients with chronic schizophrenia [1]. Previous reports on olanzapine have been inconsistent [7, 9].
The case reports with risperidone are consistent with our findings for a beneficial effect at the lower doses [6, 10]. For example, Millson et al. [10], reported no significant antipolydipsic effect in their report using risperidone at higher doses (up to 16 mg, mean dose 13 mg over 6 months). In our case, maximal efficacy for polydipsia was evident at 4 mg risperidone daily, which is consistent with risperidone's action as an atypical antipsychotic. At higher doses risperidone increasingly blocks the dopamine D2 receptor, thereby acting like a more traditional antipsychotic [11]. Although there are no reported studies of olanzapine in the treatment of polydipsia, the observed effects in this case study are consistent with its action as an atypical antipsychotic at all doses.
A number of authors have postulated that elevated dopamine activity may drive thirst, and provide the common link between psychotic illness and polydipsia [12]. This effect may be related directly to the pathophysiology of schizophrenia or arise secondarily as a neuroleptic-induced dopamine supersensitivity [5] akin to the mechanism put forward to explain tardive dyskinesia [13] and supersensitivity psychosis [14]. Thus, supersensitivity of the D2 receptors in the hypothalamicpituitary axis may explain polydipsic behaviour. This would predict that polydipsic behaviour occurs following chronic rather than acute treatment with antipsychotics and that it does not occur at the outset of the illness, as indeed was evident in our case report. Further, the use of atypical antipsychotic medications, with their alternative receptor profiles, particularly with regard to the D2 receptor, may avoid or reverse such effects.
In this case report we also examined the effects of a novel class of angiotensin-acting drugs. Hypothalamic angiotensin is a powerful dipsogenic agent, which has been demonstrated to play a key role in mediating the normal physiological drinking responses to hypertonicity and hypotension. Weisinger [8] reported that an angiotensin-II receptor blocker reduced the powerful dipsogenic effects of either angiotensin-II or hypertonic saline infused into the cerebral ventricles of animals.
Therapeutic trials of ACE inhibitors in polydipsic patients have yielded mixed results [15]. In Mr A's case several ACE inhibitors used for treatment of his hypertension showed no coincidental significant impact on his problems with polydipsia and hyponatraemia.
Recent angiotensin-II receptor blocking drugs, developed for the treatment of hypertension, have not previously been used to treat polydipsia. In the case presented, adjunctive irbesartan successfully controlled Mr A's hypertension and also improved his polydipsia to manageable levels. Thus, for those polydipsic patients who respond poorly to antipsychotic medications or other behavioural interventions, a trial of this novel class of drugs acting centrally on the angiotensin system should be considered.
Footnotes
Acknowledgements
We thank the staff on the Adult Mental Health Rehabilitation Unit at Sunshine Hospital, St Albans, for their help with the assessments and the patient for his cooperation.