
Abstract
Are patients with thought disorder aware of their deficit? More specifically, are patients with disorganised communication or poverty of speech aware of their deficit? If they are aware of their deficit, what are the clinical and research implications of this awareness? How can awareness versus unawareness of thought disorder inform our understanding of the pathogenesis of this symptom? In this paper we present details of a new instrument designed to assess awareness of communication deficits, and explore correlations between scores on this instrument, ability on tests sensitive to impaired executive ability and objective ratings of thought disorder.
In clinical practice patients with thought disorder rarely complain spontaneously about this symptom and most appear unaware that the listener has found their discourse difficult to follow. From a research perspective, little is known about awareness of thought disorder. In his classic paper, Chapman [1] transcribed the responses of patients with recent-onset schizophrenia to open-ended questions related to their symptoms. Although Chapman provided no information on whether these same patients actually had thought disorder, he suggested that the monitoring of speech output might have been altered in thought disorder.
Chaika [2] commented that the thought-disordered patient seemed unaware of errors and suggested that this feature was a distinguishing feature of thought disorder. Chaika proposed that this unawareness was due to an impaired ability to monitor speech output. Comparing patients with schizophrenia with patients with posterior aphasia, Gerson and colleagues [3] found that the schizophrenia group was less aware of communication problems.
There are no instruments designed to specifically assess awareness of thought disorder. Recently, a comprehensive scale for the assessment of insight in psychosis was published: the Scale to Assess Unawareness of Mental Disorder (SUMD) [4,5]. This scale contains 40 items, one of which is related to awareness of thought disorder. Using this scale, Amador and colleagues reported that 57.4% of patients with schizophrenia (n = 199) had a moderate to severe lack of awareness of having a mental disorder [5]. Of those with at least mild thought disorder (as assessed by the Scale for the Assessment of Positive Symptoms [6]), approximately 52% had ‘severe unawareness’ of the symptom.
Error monitoring and error utilisation in efficient communication
Efficient speakers constantly and simultaneously monitor many aspects of communication (e.g. articulation, semantics, syntax construction, discourse planning, pragmatics) [7]. Rubens and Garrett [8] have cited the constant interruptions, reformulations and repairs that occur in the speech of even the most proficient speaker as indicative of the crucial role of monitoring in everyday communication, and have suggested that the ability to detect and then correct errors is central to efficient speech. The detection of errors in one's speech will be referred to in this paper as ‘error monitoring’ (synonyms include self-monitoring, error detection, error identification, error recognition, error evaluation). Once an error is detected, efficient speakers attempt to restore fidelity between the desired and performed actions. In this paper, this restoration will be referred to as ‘error utilisation’ (synonymous with self-correction, error correction).
Error monitoring and error utilisation are key features of executive ability and are thought to be central to general awareness of deficit [9]. Young et al. [10] have reported an association between impaired performance on tests of executive function and a generalised lack of awareness of illness (based on the SUMD) in a group of patients with chronic schizophrenia. This finding would suggest that those with unawareness of their thought disorder would do poorly on tests sensitive to impaired executive ability. We have previously hypothesised links between aspects of impaired executive ability and thought disorder [11,12]. We have recently reported significant correlations between increased levels of positive and negative thought disorder and impaired performance on various tests of executive ability [13].
The Communication Awareness Scale (CAS)
In order to explore issues related to awareness of thought disorder a self-report scale was developed: the Communication Awareness Scale (CAS). Items for the CAS were generated from clinical experience and from the main items in Andreasen's Scale for the Assessment of Thought, Language and Communication [14,15]. The CAS consists of 38 statements describing awareness of aspects of positive thought disorder (e.g. ‘I have trouble keeping on the topic’, I forget the point of what I was saying', ‘I have episodes when my speech is jumbled’) and poverty of speech (e.g. ‘I don't say much'). In addition, there are items related to awareness of the needs of the listener (e.g. ‘My speech seems confused to others’, ‘I find people have trouble following what I say’) and general items (e.g. ‘I feel frustrated when I can't get my message across'). Subjects are asked to respond to the items by circling one of four anchor points related to frequency (e.g. ‘never’, ‘very rarely’, ‘sometimes’, ‘very often’). For all CAS scores, higher values indicate increased frequency of awareness of communication deficit.
During the development of the CAS a well control sample was drawn from undergraduate university students, hospital and community mental health staff and members of a non-government organisation (n = 121). Forty of these subjects participated in test–retest assessment after an interval of 3 weeks. The intra-class correlation [16] between the two tests was 0.86. In addition, 40 patients with a DSM-III-R [17] diagnosis of chronic schizophrenia were recruited from a long-stay hospital. Based on all subjects, the split-half correlation was 0.89. Cronbach's alpha was used to assess the internal consistency of the items [18]. The coefficient alpha for an all-item analysis was 0.92. Full details of the CAS are available from the authors.
In light of empirical data which have shown that poverty of speech tends to load on a different symptom factor from positive thought disorder [19], an a priori decision was made to construct a separate score for the four items related to awareness of poverty of speech (CAS-Poverty). The scores on the remaining 34 items, which included items related to positive thought disorder, to the needs of the listener and to general communication, were summed to give a separate subscale score (CAS-Total). Finally, to assess the potential confounding effect of delusions (i.e. listener confusion as a result of disorders of content rather than form), scores on the nine items related to listener needs were extracted to give a sub-scale score called CAS-Listener.
Hypotheses
We proposed two main hypotheses for this study:
Subjects with higher objective ratings on positive thought disorder will have higher CAS-Total scores.
Subjects with poorer performance on tests sensitive to impaired executive ability will have lower CAS-Total scores.
Methods
Patients with schizophrenia, mania and a well control group involved in a longitudinal study of thought disorder were approached to participate in the present study [13,20]. The patients were recruited from consecutive admissions to two short-stay psychiatry units. The patients met criteria for a current DSM-III-R diagnosis of schizophrenia or bipolar disorder, manic phase. Well controls were recruited from advertisements placed at a local unemployment office (n = 15) and from hospital staff and their relatives (n = 5). Well controls were screened to exclude past or present psychiatric diagnoses. Participants were aged between 18 and 65 years. Exclusion criteria included the participant having colour blindness, current substance abuse or dependence (apart from nicotine and caffeine), a past history of epilepsy or a significant head injury, electroconvulsive therapy within the last 12 months and English as a second language. The relevant institutional ethics committees approved the study. After complete description of the study to the subjects, written informed consent was obtained.
The subjects included 31 patients with schizophrenia (10 female), 16 with bipolar disorder, manic phase (15 female), and 20 well controls (10 female). The mean age (and standard deviation) of the schizophrenia, mania and well control groups were 31.5 (8.9), 40.6 (12.8) and 34.0 (12.4), respectively.
Assessments
All patients were recruited four weeks after an acute admission (i.e. in the subacute phase). The Brief Psychiatric Rating Scale (BPRS) [21] was used to assess general psychopathology, and the presence of delusions in particular (item 15). Four tests were chosen to assess components of executive ability. The Wisconsin Card Sorting Test (WCST) [22], the Controlled Oral Word Association Test, the Trail Making Test (TMT) [23], and the Stroop test [24]. In order to reduce the number of comparisons, scores from these five tests were combined to give a summary score. Using data from all subjects, results for each test were transformed to z-scores. Scores from two tests (WCST Perseverative Errors and Trail B-A) were inverted (multiplied by −1) so that all transformed scores had a uniform direction (i.e. higher scores indicate superior performance). For each subject, the mean of the transformed scores of the five tests became the executive ability score. The raw and summary scores for these patients during acute and subacute phases are provided in detail in a related article [13].
Free speech samples were audiotaped and scored according to Andreasen's Scale of Thought, Language and Communication (TLC) [14,15] by a rater who was blind to all other variables. A summary score for positive thought disorder was calculated from the sum of five of the 20 TLC items (distractible speech, tangentiality, derailment, loss of goal and perseveration). Poverty of speech is the sole item representing negative thought disorder. The inter-rater reliability for these individual items, which was assessed using weighted kappa, was in the moderate to good range (0.51–0.66) [25].
Pearson product moment coefficients, or Spearman rank coefficients, were used to assess the degree of correlation between the variables of interest. In order to examine the possible impact of delusions on the CAS (patients may be aware that the listener is confused because of the presence of delusions rather than thought disorder), the relationship between the CAS-Listener subscale score and the presence of delusions (item 15 from the BPRS) was assessed when controlled for positive thought disorder (partial correlation). Two-tailed p-values are reported.
Results
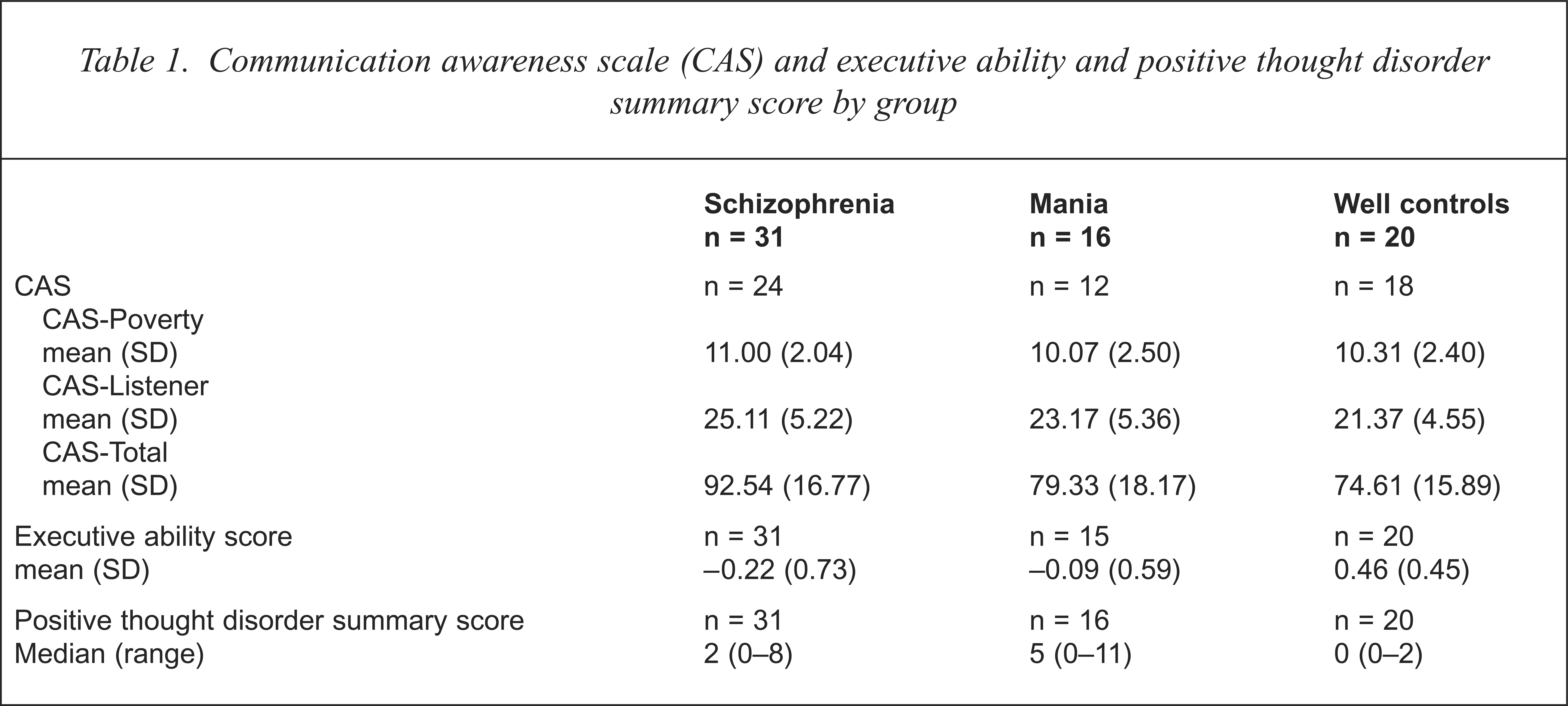
Table 1 shows the mean (and standard deviation) on the three CAS scores and the executive ability score for each group. The median and range of the positive thought disorder summary score for each group is also shown in Table 1. Note that 13 of the subjects did not complete the CAS, and one patient in the mania group did not complete the tests of executive ability (sample sizes shown in Table 1).
Communication awareness scale (CAS) and executive ability and positive thought disorder summary score by group
In order to assess the first hypothesis, a Spearman rank coefficient was calculated between the CAS-Total subscale score and the positive thought disorder summary scores. A weak but statistically significant correlation was found (Spearman rho = 0.28, p = 0.04). Inspection of the scatterplot (Fig. 1) revealed that those without positive thought disorder had a wide range of CAS-Total scores. Post hoc analysis of the subgroup with thought disorder (greater or equal to 1 on the summary score) found a stronger relationship between thought disorder and CAS-Total scores (Spearman rho = 0.50, p = 0.005).
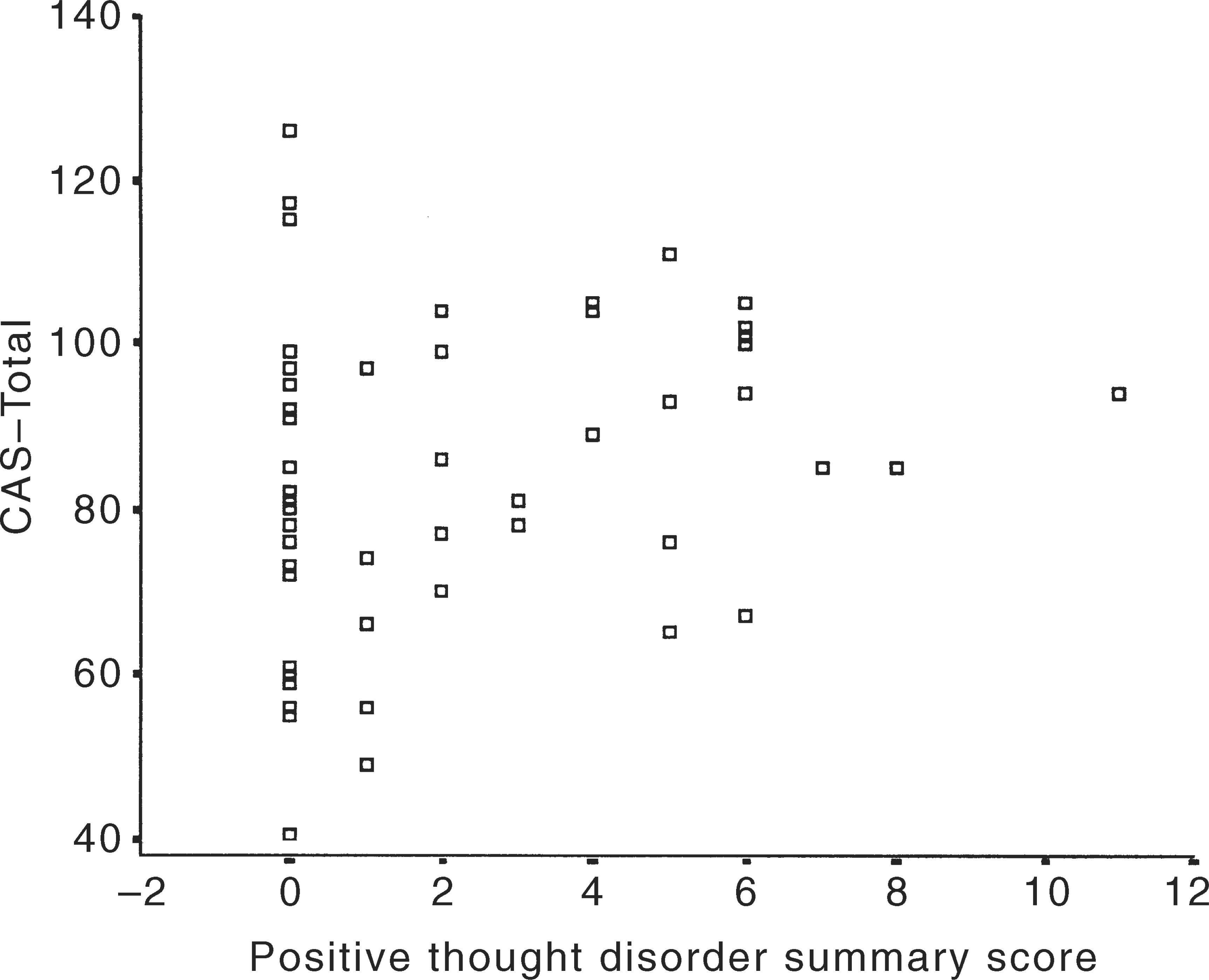
Scatterplot of positive thought disorder summary score by CAS-Total
There was no association between poverty of speech as measured on the free speech sample, and the CAS-Poverty subscale score (Spearman rho = 0.03, p = 0.81).
Next, the relationship between CAS-Total subscale score and performance on tests of executive ability was examined. The Pearson product moment correlation between the two variables was –0.33 (p = 0.01), a relationship opposite to that hypothesised (see Fig. 2).
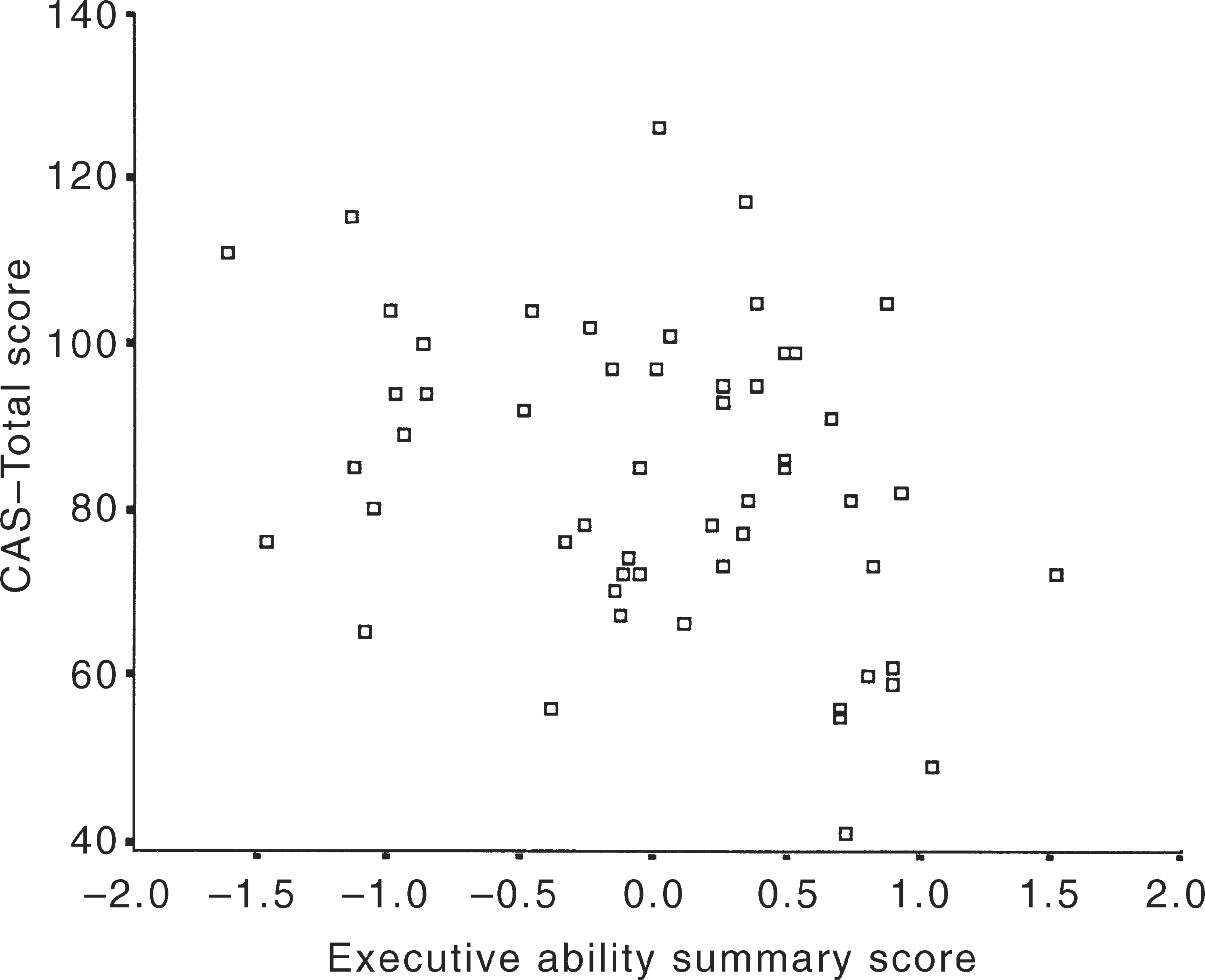
Scatterplot of executive ability summary score by CAS-Total score
A significant negative correlation was also found between scores of executive ability and CAS-Poverty subscale score (Spearman rho = –0.31, p = 0.01). Finally, the association between the CAS-Listener subscale score and delusions (item 15 on the BPRS) was not significant when controlled for the presence of positive thought disorder (r = 0.04, p = 0.80).
Discussion
A weak but significant positive correlation was found between positive thought disorder and awareness of this symptom. Therefore, Hypothesis 1 received support. However, post hoc analysis revealed that those without thought disorder behaved heterogeneously with respect to the CAS-Total sub-scale score thus lessening the strength of the correlation for the hypothesis as it was originally stated. In light of these data it seems prudent to restate the hypothesis as follows: in subjects with positive thought disorder, those with higher levels of thought disorder will tend to show more frequent awareness of communication deficit than those with lower levels of thought disorder.
There was no association between poverty of speech and the CAS-Poverty subscale score. However, there were relatively few patients with poverty of speech in this subacute patient sample (only 10 individuals with schizophrenia scored 1 or higher on this TLC item). The finding therefore is inconclusive due to lack of power rather than a negative finding. When controlled for the presence of thought disorder, there was no significant relationship between the presence of delusions and the CAS-Listener subscale score. This suggests that awareness of listener confusion due to the content of speech (e.g. the speaker suffered from delusions), rather than due to the form of speech, was not a significant confounding variable in this group.
There was a relationship between performance on tests of executive functioning and CAS-Total sub-scale score; however, this relationship was in the opposite direction to that hypothesised. Subjects who were impaired on the neuropsychological tests had higher rather than lower CAS scores. When only those subjects who scored greater than zero on the positive thought disorder summary score were assessed, the negative correlation became non-significant (data not shown). Hypothesis 2 can be rejected. The only published work that assessed unawareness of illness and neuropsychological performance found a relationship in the hypothesised direction [10]. The instrument they used to measure awareness (the Scale to Assess Unawareness of Mental Disorder), is a general instrument that assesses awareness of thought disorder among a large range of other variables. As insight is a heterogeneous concept [26,27], it is conceivable that patients could maintain awareness of thought disorder while losing awareness of other symptoms. Patients with neurological disorders have been reported who are aware of only some of their impairments [28]. Future studies will need to include general instruments such as the Scale to Assess Unawareness of Mental Disorders as well as the CAS in order to explore this issue.
One explanation for the paradoxical findings for Hypothesis 2 could be dissociation between the executive functions of error monitoring and error utilisation. In the present context, subjects with thought disorder are either not monitoring their output for errors, or if they are aware of errors, not correcting them. If a subject is both thought disordered and aware of this deficit, it follows that he or she is not effectively error utilising. Such error correction would lead to the restoration of normal speech. If error utilisation was intact (all errors monitored and utilised), then this group would not have thought disorder. However, the CAS scores for this group would be related to the base rate of errors that they are monitoring and utilising. Those with more errors to monitor and utilise will have higher CAS scores than those with fewer errors. In other words, within the well control group the CAS scores will be proportional to the number of errors monitored and utilised. It is only when the subjects' ability to error utilise begins to fail that the subject becomes thought disordered.
With respect to the present study's unexpected finding of an association between poor scores on the executive ability summary score and increased awareness, this may relate to the complex nature of executive ability. Subjects could have done poorly on the tests used in this study with intact error monitoring and impaired error utilisation (i.e. They know they may have made a mistake, but they can't use this information to improve their performance of the tasks). This speculation will need to be addressed in future studies.
Table 2 outlines a model of thought disorder that describes four permutations between three predictor variables (error rate, error monitoring, error utilisation) and two outcome variables (the presence or absence of thought disorder, CAS scores). The rate of errors could result from any number of factors that have an impact on the construction of discourse. In particular, the inability to maintain or change set would result in an increase in the base error rate in language production. The error rate would be increased, by definition, in all thought-disordered speakers, but also could be increased in some speakers without thought disorder. The ability to utilise errors would also be reflected in the subject's performance on tests of executive ability (poor error utilisation resulting in impaired performance on selected neuropsychological tests).
Proposed model of the pathogenesis of thought disorder
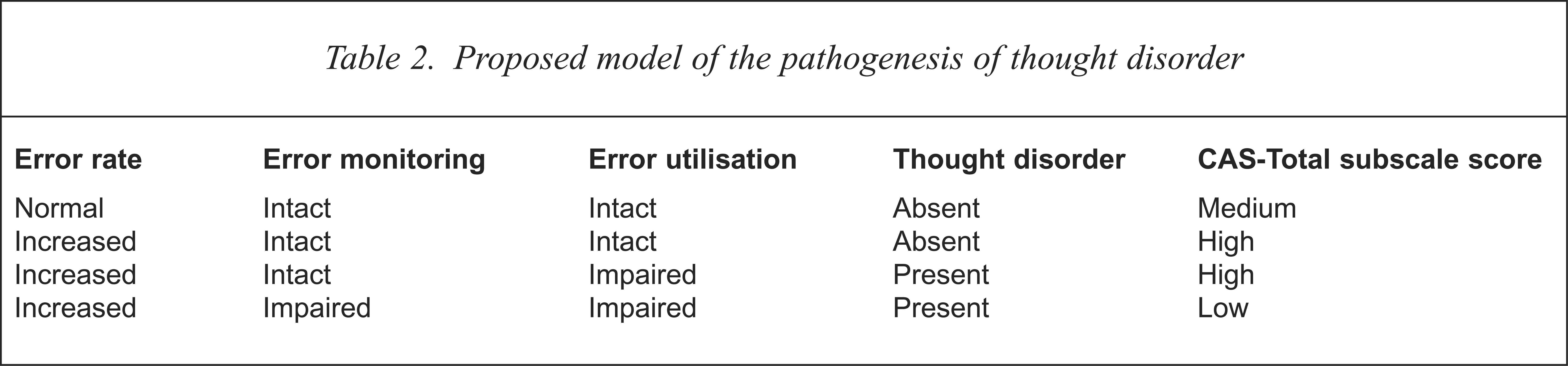
The table presents selected permutations in order to illustrate aspects of the model. It does not portray all potential permutations, nor does it reflect the variable ‘reserve capacities’ of the putative elements of the model. The first row of the table reflects the ideal situation, the unimpaired, non-thought disordered speaker. The second row describes the non-thought disordered/increased awareness speaker. The heterogeneity of CAS scores in the non-thought disordered group (see Fig. 2) would be accounted for by this combination. The next row describes the thought disordered/increased awareness speakers, who are well represented in this study. These subjects can no longer utilise all the errors that are being detected, with the end result that thought disorder ‘breaks through’. As error monitoring is intact, the subject is still aware of their increased error rate. This awareness is reflected in their higher CAS scores. The table also shows another, final combination of variables which describes the thought disordered/low awareness speaker. The current study, with subjects in the subacute phase of their illness, identified few subjects in this category, so this element of the model is entirely speculative. A sample of patients in a stable, chronic phase of illness may identify more subjects with the last combination of variables.
The mechanisms that cause unawareness of thought disorder are unknown. Lack of awareness may be a consequence of many years of positive thought disorder. Some patients may ‘habituate’ to chronic thought disorder, and become less motivated to correct their errors. Early researchers such as Harry Stack Sullivan [29] noted that thought disordered patients could be embarrassed by their disturbed speech early in their illness, but totally indifferent to similar symptoms later in the course of their illness. Leudar et al. [30] noted that while patients with schizophrenia were aware of errors in an experimental language task, their attempts to make corrections only resulted in more errors. It is conceivable that after years of frustration associated with failed attempts at correcting communication errors, the persistently thought-disordered speaker could reduce or neglect error monitoring.
Limitations of the study
Several qualifying points need to be made in respect to this study. These involve properties of the CAS, the degree to which these results may be generalised, and alternative explanations for the results. Andreasen's Scale for the Assessment of Thought, Language and Communication [14,15] is a ‘present state’ instrument, while the CAS provides no explicit time frame for the responses. Subjects may score the CAS for variable periods depending on factors such as memory and total lifetime episodes of thought disorder. The result of this mismatch in time frames between the two instruments would tend to reduce the strength of an association between positive thought disorder and CAS scores. A similar qualification would apply when assessing the degree of correlation between performance on neuropsychological tests and the CAS.
To determine whether the results of this study can be generalised, it will be necessary to re-assess the variables presented in this study in other groups of patients. As mentioned already, more long-stay inpatients will need to be recruited in order to increase the sample size of subjects with the unaware/thought disordered pattern of responses and poverty of speech. Future studies should also examine awareness of thought disorder in the wider context of general awareness and insight. Instruments have recently become available that can provide such an assessment [4]. It will be of interest to learn if the aware/thought disordered patients have unawareness of other deficits (i.e. is the awareness of thought disorder a ‘splinter’ skill?). It will also be important to examine the state and trait features of the CAS by undertaking repeated measures in patient groups over time.
Conclusions
This study found that subjects with thought disorder have an awareness of their symptom that is positively correlated with the severity of thought disorder. Contrary to expectations, impaired performance on tests sensitive to executive functioning was not associated with impaired ability to monitor the efficiency of speech output. We speculate that the rate of error production, combined with the ability of the speaker to error monitor and utilise, may contribute to a threshold beyond which ‘break through’ thought disorder occurs. This model suggests that error utilisation may be an important, rate-limiting step in the pathogenesis of thought disorder.
A clearer understanding of the factors that contribute to thought disorder may uncover variables suitable for intervention. For example, cognitive rehabilitation techniques can assist some neurological patients with unawareness of deficit [31]. Thought-disordered patients with high awareness may benefit from interventions that reduce the planning load on the speaker and maximise available error utilisation capacities. Thought-disordered patients with low awareness may benefit from social skills training, prompting them to occasionally check on the listener's needs. It remains to be seen whether thought-disordered patients could benefit from such techniques or other types of ‘speech therapy’.
Acknowledgements
Details of this study were presented at the Seventh Biennial European Workshop on Schizophrenia, Les Diablerets, Switzerland, 1994. The authors are indebted to Sue Scheldt, Joy Welham, Anne Clair and Beverley Raphael. The project was supported by the National Health and Medical Research Council.