
Abstract
New Zealand has a shortage of psychiatrists. The current ratio of one psychiatrist for 14 880 people is considerably lower than the ratio of 1:10 000 recommended by the World Health Organization [1]. The country has vacant training positions in psychiatry and directors of training expect this situation to continue in the foreseeable future. This shortage of psychiatrists and trainees may be due to a number of factors including a low rate of recruitment into psychiatric training programs, a high rate of failure to complete training, failure to practise after completion of training or departure from New Zealand after completion of training. Some of these variables have been explored in studies overseas.
There are reports of difficulties in maintaining adequate recruitment into psychiatric training programs in a number of countries [2–4]. The decision making process around the choice of specialty career is complex, and studies suggest that, for psychiatry at least, both premedical [5–9] and medical school factors [7,10–13] are likely to be important. The premedical school factors include demographic, social and personality factors as well as personal and family experiences of illness and therapy. The medical school factors that emerge as most prominent are the quality of psychiatric undergraduate medical education, the priority given to psychiatry in undergraduate training and the clinical experience of contact with both patients and psychiatrists.
Failure to complete psychiatric training may relate to job dissatisfaction, high levels of stress and burnout, emotional illness, failure in examinations or dismissal. There are high rates of burnout and psychiatric morbidity in doctors in general [14–16] and in mental health staff in particular [17–19]. It therefore seems likely that burnout or psychiatric morbidity may be influential factors in psychiatric trainees' decisions to leave prior to completing training. In a recent publication [20], The New Zealand Doctors' Health Advisory Service commented on the lack of information about the health of doctors in New Zealand, but noted that many of the referrals to the service are for problems related to mental illness and alcohol/drug addiction.
There is a poverty of literature on the other factors (of failure to practise or emigration after completion of training) and minimal literature that looks specifically at the New Zealand setting. This study was designed to explore the factors influencing recruitment and retention in psychiatric training in New Zealand.
Method
The study was conducted through the Department of Psychological Medicine at the Wellington School of Medicine. Ethical approval was obtained from the Central Regional Health Authority Wellington Ethics Committee.
The aims were: (i) to construct a profile of the psychiatric registrars currently working in New Zealand, (ii) to identify factors of importance in the recruitment and retention of psychiatric trainees in New Zealand and (iii) to compare current trainees with those who had discontinued training, in order to attempt to identify any factors which might predict failure to complete training.
Samples
Sample A (current trainees): all of the current psychiatric trainees in New Zealand (n = 123) were eligible to participate. The names and addresses of those registered as trainees with the Royal Australian and New Zealand College of Psychiatrists (RANZCP) were provided by the Staff of the Secretariat of the RANZCP.
Sample B (ex-trainees): all those who had left training during the preceding 5 years, without completing the training program were eligible to participate. The Secretariat of the RANZCP provided their names and most recent addresses and the New Zealand medical register was used to update the addresses of those still registered as medical practitioners.
Procedure
Sample A: an 83-item postal questionnaire was designed and sent to all psychiatric trainees in New Zealand in March 1997. A stamped addressed return envelope and numbered card, along with an explanatory letter, were included with the questionnaire. The envelope and numbered card ensured anonymity of the returned questionnaires, while allowing for the follow-up of initial non-responders. Two further mail-outs were sent to non-responders between March and May 1997.
Sample B: a 27-item questionnaire was designed and sent to all ‘ex-trainees’, again with an explanatory letter, and using the numbered card to ensure anonymity while allowing follow up of non-responders.
Measures
Sample A
The questionnaire included (i) questions about demographic information including age, gender, marital status, country of birth; (ii) questions about alcohol and cannabis use and family and personal history of mental illness; (iii) the 12-item General Health Questionnaire (GHQ-12) [21] which has been used as a screening measure of general psychological well-being in community samples and in a range of occupational samples including health professionals; (iv) the Maslach Burnout Inventory (MBI) [22], a self-report questionnaire which is the instrument used most widely for measuring ‘burnout’ in the caring professions; (v) a modified version of a physician satisfaction instrument [23,24]. Two items relating to availability of supervision and peer support were added; and (vi) questions about recruitment [25], training and future career plans.
Sample B
The questionnaire sought: (i) the same demographic data regarding age, gender, marital status, country of birth; (ii) the same information about family and personal history of mental illness, and alcohol and cannabis use; and (iii) data related to recruitment, training and reasons for discontinuing training.
Statistical analysis
Epi-Info Version 6 (Centers for Disease control and Prevention, Atlanta, GA, USA), a word-processing, database and statistics program for public health, was used for data entry and analysis. The Chi-squared test and Fisher exact test were used to analyse categorical data. The Kruskal–Wallis test was used for ordinal data.
Results
Of the 123 current trainees (sample A) to whom questionnaires were sent, six had left the training program, three had become consultants, and no current address was available for one, resulting in a sample size of 113. The response rate for this group was 87.6% (n = 99).
Of the 51 trainees who had left training prematurely (sample B), no current address was available for 9, leaving a sample size of 42. The response rate from this group was lower at 66.7% (n = 28).
As the same information on general characteristics and recruitment was requested from both current trainees and ex-trainees, these data are presented together. This provides a general profile of both groups, and allows for ease of comparison between them. Most questionnaires were completed fully therefore the response rates for the individual items of the following data are 100% unless otherwise stated.
General characteristics
1) Sociodemographic
The general sociodemographic features of the groups are demonstrated in Table 1. The only significant difference between groups was that more of the trainees who had left training had been born overseas.
2) Mental illness
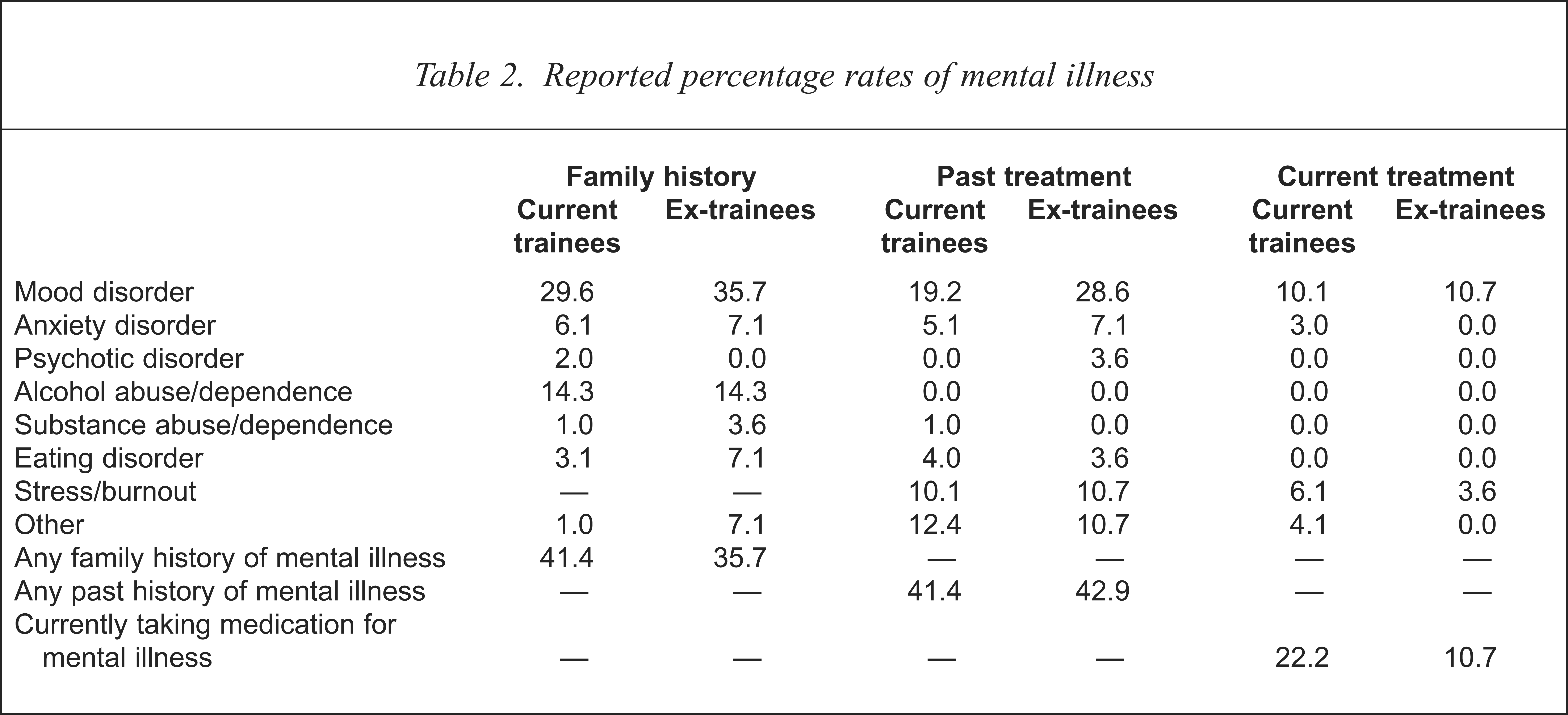
These items focused on family history of mental illness, and past and current personal history of mental illness. Respondents were asked:
‘Do you have a family history (parents and siblings) of any of the following?’, ‘In the past have you had treatment (including counselling) for any of the following?’ and ‘Are you currently receiving treatment (including counselling) for any of the following?’ Results are shown in Table 2. There were no significant differences in the reported rates of family, past or current history of mental illness between the current trainees and those who had discontinued training. Note however, that although the data provide a profile of both groups currently, it does not provide direct information on rates of illness in the ex-trainee group at the time that training was discontinued.
3) Alcohol and cannabis use
In the current trainee group, 30.3% identified themselves as non-drinkers, 42.4% reported a weekly intake of 1–6 standard drinks and 19.2% reported a weekly intake of 7–12 standard drinks. The two groups showed no significant difference in terms of the percentage of alcohol drinkers and non-drinkers. However, of the current trainees, three females and one male were consuming above the upper limit of safe drinking (21 standard drinks/week for males, and 14 standard drinks/week for females) [26].
There was no significant difference in the proportion of cannabis users between the current trainees (31.3%) and ex-trainees (28.6%). Note that the ex-trainee data describe current use and do not provide information on alcohol or cannabis use in the ex-trainee group at the time training was discontinued.
Demographic data
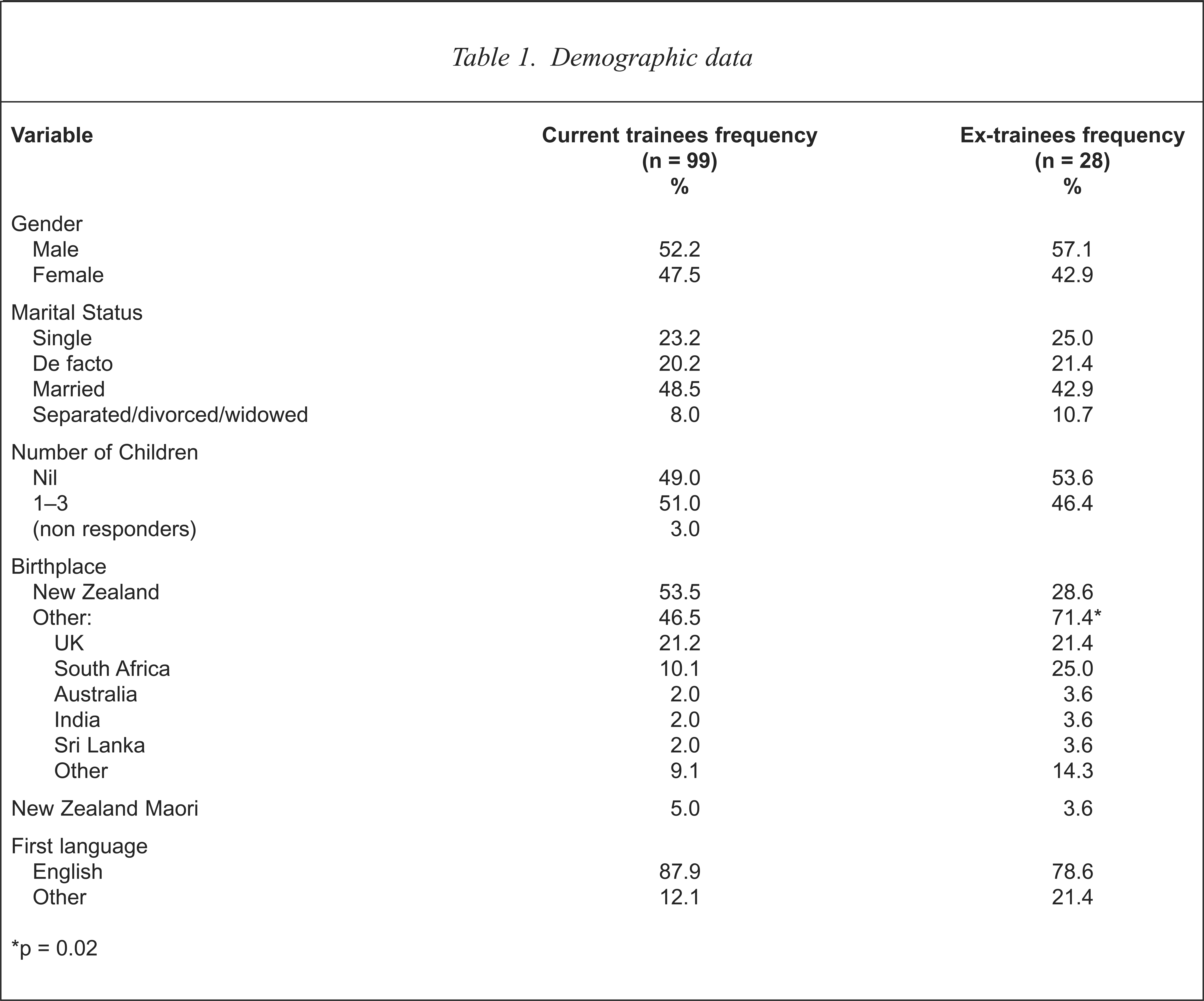
p = 0.02
Reported percentage rates of mental illness
Recruitment
Items in this category related to the site of training and the timing and reasons for the choice of psychiatry as a career. Of current trainees, 60.7% were New Zealand graduates, compared with 38.3% of ex-trainees (p = 0.04). This correlates with the high proportion of overseas-born ex-trainees as noted in the demographic data. The majority of overseas-trained doctors in both groups completed their undergraduate training in the United Kingdom and South Africa.
There were no significant differences between current trainees and ‘ex-trainees’ as to when psychiatry was seriously considered as a career, which was most commonly as a house-surgeon or senior house officer (SHO) (55.6% for current trainees).
The most important factors identified by the trainees in their decision to train in psychiatry were philosophical interest in psychiatry (27.5%), house-surgeon/SHO experience in psychiatry (20.3%) and possession of attributes they thought would be successful for psychiatry (15.9%). There was no significant difference in frequency of factors between the two groups.
For the remainder of the results, the survey questions differed between the two groups, and so will be considered separately.
Work/training experience
For current trainees, items in this category included current year of training, work/training satisfaction and examination experience; 16.1% of trainees were completing their sixth or greater year of training.
Respondents were asked to indicate their satisfaction with various factors related to training and employment, using a modified physician satisfaction instrument. Overall, 94.0% indicated that they were satisfied or very satisfied with their decision to pursue a career in psychiatry. However, dissatisfaction was expressed with a wide range of factors. Most dissatisfaction was expressed regarding satisfaction with availability of resources, with 82.6% dissatisfied with workforce resources available to meet the needs of patients, while around one-third were dissatisfied with quality and availability of supervision, as well as availability of peer support. For satisfaction with clinical practice, 52.5% were dissatisfied with their role in organisational and administrative decisions, and over one-third were dissatisfied with the degree of status and prestige associated with the work, the patient volume and the amount of contact with other physicians. For satisfaction with opportunities for personal development, 28.3% were dissatisfied with their ability to remain knowledgeable and current.
RANZCP examination results for current trainees are given below for each step in the examination process. The numbers indicate first the percentage who passed with their first attempt, and second, in parentheses, the percentage who have passed overall. First year exam 86.2% (98.3%), all cases 82.2% (100%), written exam 38.1% (80.9%), clinical exam 28.6% (64.3%).
Nearly 90% of current trainees indicated that they were likely or very likely to complete training. Future failure in examinations and unsatisfactory working conditions were identified as the two factors that would be most likely to cause the trainee to leave the program.
In the work/training experience category, ex-trainees were asked about the stage of training at which they discontinued, their reasons for leaving training, and examination results. Most of those who had left training prematurely did so within the first two years, with 18 of the 28 leaving in first or second year, 6 in the third year and 4 in subsequent years. This suggested that examination failure is not a common reason for leaving training, which is supported by the finding that 91% of the 17 ex-trainees who attempted the first year exam passed with their first attempt.
The commonest reasons given for discontinuing training were job dissatisfaction (53.6%), stress/burnout (39.3%), pregnancy/parenthood (10.7%), other mental health problems (10.7%) and exam failure (10.7%).
Only one trainee had obtained a qualification in psychiatry from another college, after leaving the training program. A further eight still worked in psychiatry as Medical Officers or trainees in programs overseas.
Burnout and general health
Current trainees completed the Maslach Burnout Inventory (MBI) (Table 3). The total score for each subscale is categorised as low, medium or high according to predetermined cut-off scores based on normative data from a sample of American health professionals [27]. A high degree of burnout is indicated by high scores on the emotional exhaustion and depersonalisation subscales and low scores on the personal accomplishment subscale.
Estimated rates of burnout using Maslach Burnout Inventory
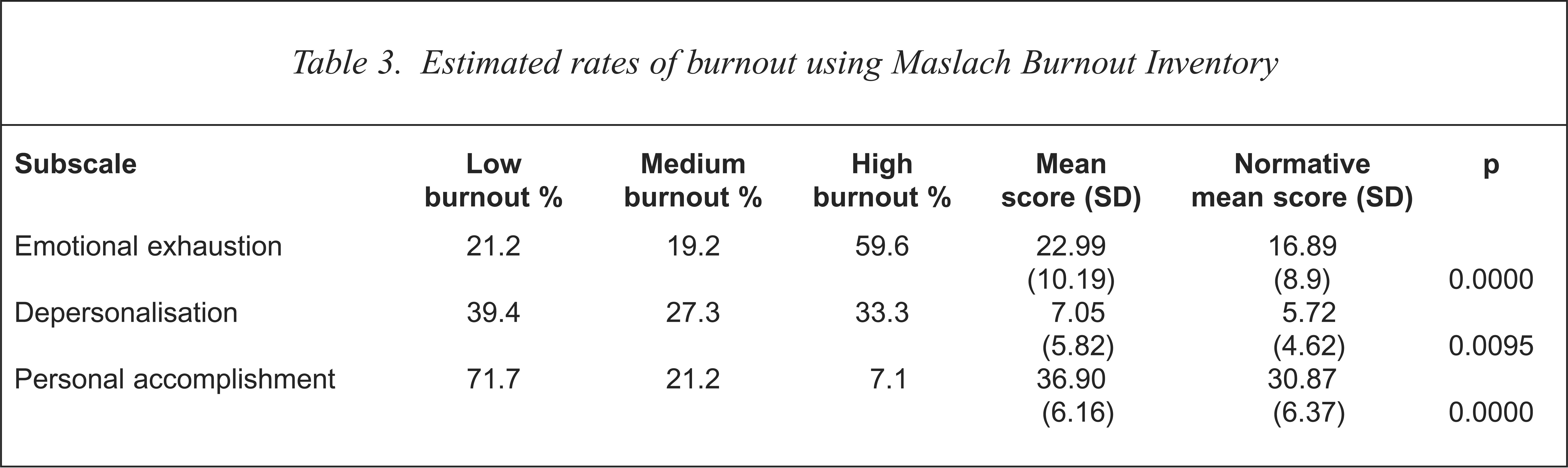
The left side of the table shows the results using standard cut-off scores and the right side of the table uses the original numerical scores for statistical analyses, as recommended by the MBI authors. Compared to the normative data, which is based on MBI ratings of mental health workers, the current trainees scored significantly higher on each subscale of the MBI. Note that for emotional exhaustion and depersonalisation higher scores suggest higher levels of burnout. The low burnout levels for personal accomplishment fit with the observation of Onyetts et al. [18] that a high level of work commitment is regarded by some theorists as a prerequisite to burnout.
This same group completed the General Health Questionnaire-12 (GHQ-12). Of these, 31.3% had a GHQ-12 score of 4 or more (indicating likely psychiatric morbidity) using the GHQ scoring method. The range was 0–12, mean 2.3, median 1.0, and standard deviation 2.9.
Future plans
The trainees were asked to estimate how long it would take them to complete training. Most, 76.5% of trainees, thought that it would take longer than 5 years to complete the training program, and more than 20% thought that it would take longer than 8 years; 34.3% indicated that they were likely to leave New Zealand when they had completed training, most (77.4% of these) believing that this would be for up to 3 years and usually to broaden experience. Overall, 90.6% intended to practise in New Zealand eventually.
Comments on recruitment and retention
Current trainees were invited to make general suggestions of ways to improve recruitment. The most frequent suggestions were to: (i) improve undergraduate experience and teaching (41%) and (ii) encourage/ensure house-surgeon experience in psychiatry (24%).
All respondents were invited to make general comments about ways to improve the retention of trainees in psychiatry. The most frequent suggestions from both groups were to: (i) improve supervision, (ii) increase the emphasis on training as opposed to service, (iii) improve support from senior colleagues and (iv) improve the resources in mental health.
Discussion
This study provides a profile of current psychiatric trainees in New Zealand and of those who had left training prematurely in the preceding 5 years. It identifies some of the factors important in recruitment and retention and explores factors which may predict failure to complete training. The response rate of 87.6% of current trainees suggests that the study has representative validity in terms of current New Zealand psychiatric trainees. The response rate of 66.7% of those who had left training is gratifying, given that one might expect less enthusiasm from those who may have been dissatisfied with psychiatry.
The key finding with respect to recruitment is that the decision about the future medical speciality was generally made in the house-officer years, based on positive experiences and philosophical interests in psychiatry. This is in agreement with previous findings [5,6,10–12].
In considering factors which might influence retention, there were high rates of psychological morbidity and burnout among current trainees and high rates of dissatisfaction with numerous aspects of the work environment particularly the availability of resources, workload and role in administrative decisions. Despite this, most trainees were satisfied with their decision to train in psychiatry and expected to complete their training and eventually to work in New Zealand. Poor working conditions and possible future failure in examinations were the most common factors identified by the trainees that could potentially result in a decision to discontinue training. However, it is noteworthy that the experience of failure in examinations was not a significant determinant of failure to complete training in the ex-trainee group.
The trainees who had left training prematurely were largely indistinguishable from those who remained in training, with the exception that a higher percentage of trainees who had been born and trained overseas left training. The reason for this is not apparent from the data but could relate to language difficulties, cultural differences or the experience of prejudice. The possibility that doctors from overseas took positions in psychiatry because no other positions were available warrants consideration. However, it was not identified in this study as an important factor by those who discontinued training.
The high rates of mental illness reported in both groups are of particular note. However, a family or personal history of mental illness was not identified as an important determinant of career choice, and the rates did not differ between the current and the ex-trainees groups, which suggests that this is not a major factor in determining retention in psychiatry. The high rates of treated mental illness and burnout reported are of concern and are consistent with other reports [14–20]. The current study may have reported more accurately the level of psychiatric morbidity (as indicated using the GHQ) than other studies, because the high response rate minimised non-responder bias due to psychiatric morbidity. It should also be noted that the threshold score used in this study (4 or greater on the GHQ-12, using the GHQ scoring method) is one of the highest thresholds used for identifying psychiatric morbidity. Using a lower threshold would be expected to have identified even higher rates of probable psychiatric morbidity.
The question of whether such findings reflect vulnerability at intake (‘susceptible personality’) [28] or the stress of practice resulting in psychological impairment (‘role strain hypothesis’) [29] is yet to be resolved. Rucinski [30] proposed an interacting model of the ‘role strain hypothesis’ and the ‘susceptible personality theory’, suggesting that the stresses that are inherent in the practice of medicine precipitate mental disorder in those predisposed to it and that practice is particularly stressful for the ambitious, inflexible individual with a family history of mental disturbance and an unhappy or unstable childhood.
The Christchurch Psychiatric Epidemiology Study [31] studied a New Zealand community population using the Diagnostic Interview Schedule and reported an overall lifetime prevalence rate of 36.6% for the main Epidemiologic Catchment Area (ECA) diagnoses. The highest lifetime prevalences found were for generalised anxiety disorder (31%) and alcohol abuse/dependence (19%), with the reported rate for mood disorders of 14.7%. In comparison, the reported rates of treatment for any disorder (41.4%) and mood disorder (19.2%) in this survey are high, while the reported rates for treated anxiety disorders and alcohol abuse/dependence are lower. A combination of age, cohort effect, improved recognition of disorder and the addition of the stress/burnout category may explain the higher rates in this group.
Interpretation of these results is limited by several factors. One possible limitation of this work is the reliance on accurate self-reporting. However, there were few missing data, and most repondents seemed to be very candid about personal information, as indicated by the responses to questions regarding mental illness and drug and alcohol use, so it is unlikely that this has significantly influenced the results. A second possible limitation is that of the definitions used. For example, past and current mental illness were defined as ‘having received treatment’. This will have underestimated rates because psychiatric illness is frequently untreated, and doctors may be particularly reluctant to present for treatment. Equally, the inclusion of stress/burnout as a mental illness category may have inflated those results although the receipt of treatment for those conditions suggests that they caused a significant degree of psychological disturbance or distress. A third limitation is that data gathered from those who had left training were retrospective. This meant that factors such as the levels of stress and burnout at the time of leaving could not be assessed, and the rates of current mental illness and drug use may not necessarily reflect the rates at the time that the trainees discontinued training. However, there was no difference between the groups in their reported past history of mental illness.
The data from this survey and the review of literature suggest a number of issues that could be addressed to improve the recruitment and retention of trainees in psychiatry including the following
Encouraging students into a career in psychiatry. Factors to consider include establishing a compulsory rotation in psychiatry for house-surgeons, improving the role models available to students in both academic departments and clinical settings and targeting interested students early.
Improving training and work experiences. In particular, increasing the support of trainees by consultants and managers, improving supervision, improving teaching and the training scheme, improving resources, and reducing the workload.
Attending to the emotional needs of trainees. This could include the development of a mentor system, the development of support groups for trainees and education in personal health and well-being.
Improving working conditions and job satisfaction for consultants.
Acknowledgements
We thank the study participants, the New Zealand directors of training, and the RANZCP Secretariat. Special thanks to Robyn Green for statistical assistance, the Ashburn Hall Research Foundation for generous support and Sunny Collings for comments on earlier drafts.