
Abstract

Professor Goadsby
We have a full but interesting programme this afternoon. The first half is very sumatriptan-focused, with presentations on adolescent migraine, safety, primary care and the evolution of the sumatriptan story. Helen Connor will talk about the development of naratriptan and Roger Cady about using naratriptan and sumatriptan in creative ways. The first presentation will be from Reijo Salonen, who started his headache life as a neurologist in Finland. He was involved in the first sumatriptan intranasal studies and later joined GlaxoWellcome, first in Finland and then with GlaxoWellcome International, where he has continued his interest in clinical trials and development programmes with sumatriptan from the company side.
Reijo Salonen
Thank you Peter. It is great to be here in the eternal city among so many old friends. I am now responsible for medical strategy overall in our neurology and psychiatry portfolio, and I reside in the United States.
Think back to when you were first involved in the clinical trials of sumatriptan or when you first used sumatriptan in clinical practice. What was your perception of the drug in those days? and has that changed over the past 10 years? Let me help you by taking you back to the first intranasal trial that I presented 10 years ago, in 1990 in London. It was a very successful trial; at 2 h there was an efficacy rate of 75% with intranasal sumatriptan and the headache-free figures are even more impressive (Figs. 1 and 2). In this presentation, however, I am not so interested in efficacy figures. There are now four formulations (Table 1).

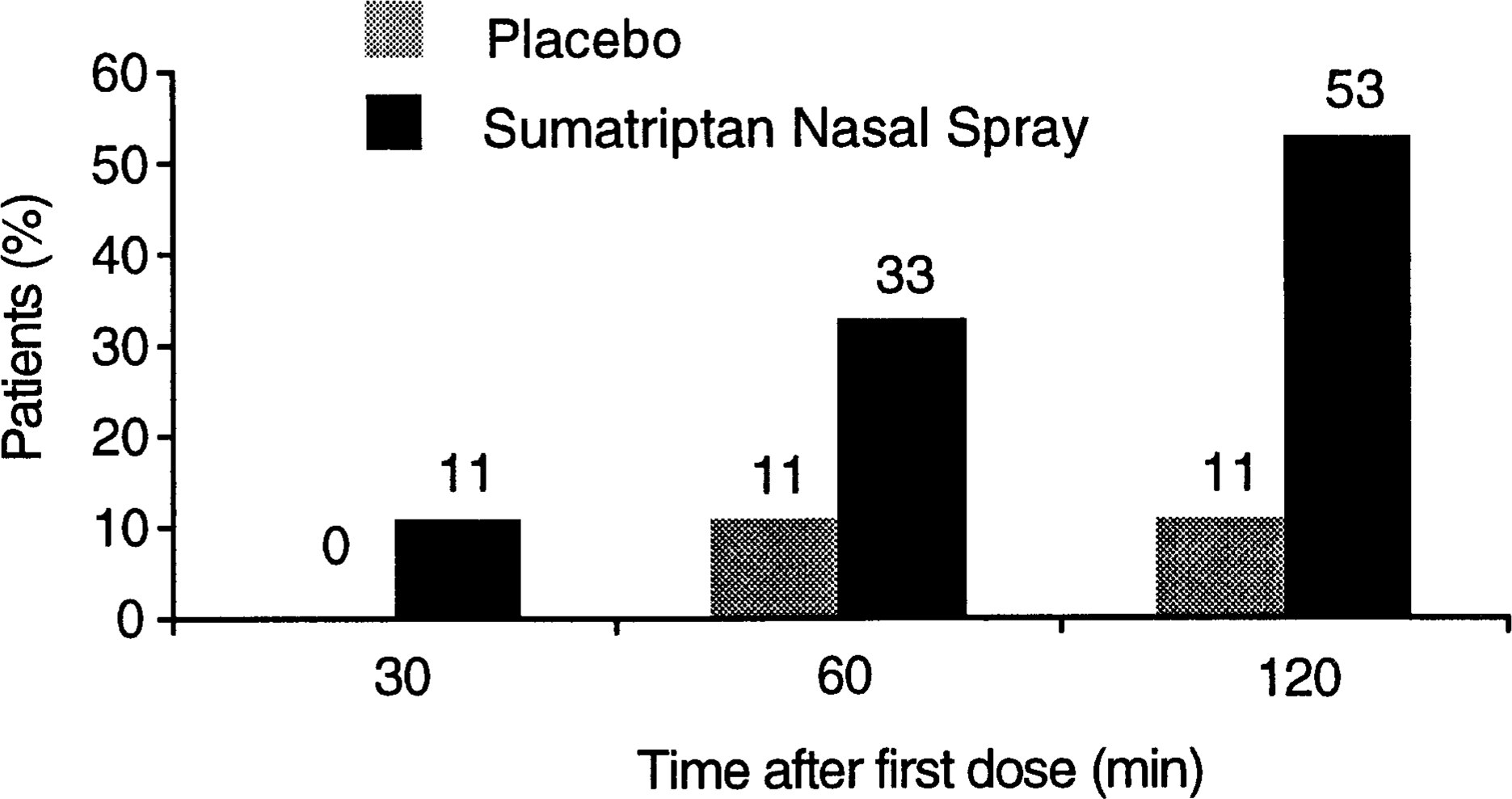
Patients with headache relief at points up to 2 h with sumatriptan nasal spray 20 mg doses. ∗P<0.005. [From Salonen, for The Finnish Sumatriptan Group and the Cardiovascular Research Group (1).]
Patients pain-free after treatment of headache with sumatriptan nasal spray 20 mg doses at points up to 2 h. Significance not determined. [From Salonen, for The Finnish Sumatriptan Group and the Cardiovascular Research Group (1).]
The four formulations of sumatriptan available and their respective times to onset of clinical action

What about time to onset of action? Has our perception of sumatriptan as a fast-acting medication changed from what it was 10 years ago? I do not think so. Clinical trials have shown that the time to onset of action for the injection is 10 min, for the nasal spray 15 min, for the suppository and the tablet 30 min (the same as for rizatriptan tabets); for zolmitriptan tablets the time is 45 min and for naratriptan tablets, 60 min. These are very efficacious drugs with a fast onset of action. In the early days we were amazed that a drug for acute migraine could act so fast and so effectively; over 10 years the results are as good as ever but our surprise has abated through familiarity.
The adverse events were generally mild and transient in the early sumatriptan trials. Taste disturbance is a peculiarity of the nasal formulation, but we did see the typical triptan adverse events such as pressure and heavy sensations in different parts of the body, including the chest. These sensations are maybe of less concern now that we know that the only clinically tested selective 5-HT1D agonist can cause the same sensations. Because the 5-HT1D agonists do not stimulate receptors on coronary arteries, the origin of these sensations is probably elsewhere. GlaxoWellcome addressed the problem of pressure sensations by developing the 2.5 mg naratriptan dose, which has the tolerability profile of placebo. We have used sumatriptan for more than 300000 attacks in clinical trials, and in clinical practice over 340 million attacks have been treated. I am sure that it will not cause major surprises to us in the future.
Over the decade, some things have changed, though. You may remember the slogan of the early 1990s when it was thought that Imigran works well when at taken any time during of the attack and whatever its severity. There were people who criticized that statement and said that it works better in mild attacks and if taken early on. They were clearly right, as shown in some recent trials. In the Spectrum study of Richard Lipton and Roger Cady (2), data on patients who treated mild attacks with 50 mg sumatriptan show that about half were pain free at 2 h and 84% at 4 h (Fig. 3). Pffaffenrath and his colleagues (3) compared different doses of oral sumatriptan. Again, for sumatriptan 50 mg the pain-free data are as in the Spectrum study, while with 100 mg the figures are even more impressive, about 70% being pain free at 2 h and over 90% at 4 h (Fig. 4). This is something we have sometimes found also in trials with traditional designs: the 50 and 100 mg doses are equally efficacious for headache relief, but the pain-free comparative data show that the 100 mg dose is better.

Percentages of patients treating while pain is mild who were pain free at 2 and 4 h after placebo or sumatriptan 50 mg PO, Spectrum Trial. (From (2).)

Pain-free responses at 2 h and 4 h with differing doses of sumatripan and with placebo, charted according to initial pain severity, M09 study. (From (3).)
In terms of efficacy, sumatriptan has lived up to its expectations and has certain advantages over other drugs with the same indication. Of course, my perception may be biased because sumatriptan and naratriptan are my children, and you have your own perception how this has changed over the 10 years based on your own clinical experience.
What about other features of sumatriptan? We have shown additional advantages for this drug with the emergence of those of our competitors. Sumatriptan is the least lipophilic of the triptans, so it has minimal CNS penetration and a very benign CNS adverse event profile. It is also metabolized by various routes but not by isoenzyme 3A4 of the cytochrome P 450 system, unlike some competing products. Inhibitors of this iso-enzyme (Table 2) raise blood levels of those triptans that are metabolized by this route and this may cause tolerance or safety problems. The MSD scientists have drawn our attention to the P-glycoprotein system, a membrane pump that removes lipophilic substances from the CNS. Sumatriptan is not a substrate for the PGP pump and thus concentrations of sumatriptan in the CNS and the blood will not be increased when inhibitors of the pump (Table 3) are also being taken.
Drugs known to inhibit the P-glycoprotein pump

Drugs known to inhibit the cytochrome P450–3A4 system

The availability of sumatriptan has brought fast and effective relief of both pain and the associated symptoms to migraine patients. As with most pharmaceutical breakthroughs, however, what started as an unique agent becomes, in time, one of a class. Each new triptan has been evaluated against sumatriptan in comparative studies, but these can be subject to subtle biases. I take issue with some aspects of the trials conducted by our competitors, such as the inclusion of previous sumatriptan users in many of them—it is likely that many of these subjects were also non-responders. One could also criticize certain aspects of data analysis in some trials and the blinding of sumatriptan by encapsulation of the tablet.
My conclusions are simple. The major issue in headache today is the suboptimal diagnosis of migraine, which is where much future effort must be focused, but in the meantime sumatriptan has revolutionized the understanding and treatment of this disabling condition. We are committed to working with you in engineering the next revolution in migraine; may that day be soon.
Thank you.