
Abstract
The reason that estrogen is strongly protective in various estrogen-deficient animal models while seemingly detrimental in postmenopausal women remains unclear. It hypothesized that prolonged oral medroxyprogesterone (MPA) plus oral conjugated equine estrogens (CEE) diminishes estrogen ability to reduce stroke damage in the rodent stroke model. To test the hypothesis, we fed ovariectomized rats CEE or MPA, or a combination of CEE and MPA (CEP), before inducing 120 min of reversible focal stroke, using the intraluminal filament model. After 22 h reperfusion, the brains were harvested and infarction volumes were quantified. Treatment with CEE alone or with CEP reduced cortical infarction volume. However, CEP failed to provide ischemic protection in subcortical regions. It was concluded that CEE alone, or with CEP, is neuroprotective in the cortex, but interactive effects between the hormones may counteract CEE beneficial effects in subcortical brain regions.
Introduction
Numerous animal models of experimental stroke show the protective effect of estrogen (Hall et al, 1991; Alkayed et al, 1998; Zhang et al, 1998), and that this gender-specific protection is lost with ovariectomy (Hall et al, 1991; Alkayed et al, 1998; Pelligrino et al, 1998). Like estrogen, progesterone has been shown to be protective in models of traumatic brain injury (Bramlett and Dietrich, 2001; Stein, 2001; Wright et al, 2001), but variable effects have been noted after ischemic brain injury (Roof and Hall, 2000; Stein and Hoffman, 2003). Early studies of unopposed estrogen replacement in women report a reduction in risk for cardiovascular disease (Hurn and Brass, 2003). Yet, recent prospective studies of women on prolonged, daily combined hormone replacement therapy (HRT) of conjugated equine estrogens (CEE; 0.625 mg) and medroxyprogesterone acetate (MPA; 2.5 mg) for primary prevention (Rossouw et al, 2002), or on 17β-estradiol alone for secondary stroke prevention (Viscoli et al, 2001), reported no protection or adverse effects of the hormones on women's risk of stroke (Wassertheil-Smoller et al, 2003).
The reason for the discrepancies between animal and human studies remains unclear, but the discrepancies highlight the fact that long-term HRT is not without risk. One difference in the animal compared with human investigations is related to study end points. Most studies of women assess long-term neurologic and/or behavioral outcomes, whereas few studies investigate neurobehavioral outcomes following stroke in animal models. Another potential explanation for these differing findings may be methodological, as most animal studies use 17β-estradiol, not CEE, and do not combine estrogen with MPA. Further, most investigations have employed parenteral routes, while studies of postmenopausal women have examined oral HRT. Unlike drugs given parenterally or subcutaneously, orally administered drugs undergo a first-pass effect in the liver that may diminish the hormone bioavailability; thus, the therapeutic effectiveness may be altered. Further, recent data indicate that under some conditions, coadministration of estrogen with MPA can antagonize the effects of estrogen (Herkert et al, 2001; Nilsen and Brinton, 2002a; Pazol et al, 2004). Although animal studies using 17β-estradiol for hormone replacement report that estrogen has a neuroprotective effect on ischemic lesion size, to date, no experimental studies have examined the effect of prolonged oral CEE, MPA, or combined CEE and MPA (CEP) on brain infarct volume after stroke. These studies are a first attempt to determine if the treatment duration, drug preparation, and the route of hormone administration alter the neuroprotective effects of CEE and MPA on brain injury previously observed in the same model. We hypothesized that prolonged oral MPA plus CEE diminishes estrogen's ability to reduce stroke damage in the rodent model. Therefore, the aims of this study were to (1) determine if the effects of long-term oral HRT treatment of ovariectomized rats (OVX) parallel the effects of parenterally or subcutaneously administered hormones and (2) ascertain if oral CEE, MPA, or the combination of CEE and MPA in doses based on body weight, relative to doses taken by postmenopausal women, differentially affect postischemic brain infarct volume.
Materials and methods
Animals and Treatments
All protocols for this study were approved by the The Johns Hopkins Medical Institutional Animal Care and Use Committee. Sexually mature (2 to 3 months old, 220 to 270 g) female Wistar rats (Harlan, Indianapolis, IN, USA) were fed CEE or MPA for 2 months before the initiation of focal stroke. All rats were OVX under halothane anesthesia, as previously described (Alkayed et al, 1998), 1 week before the initiation of drug treatment. Rats were then randomized into the following four groups: OVX, (n=7), OVX plus CEE (CEE, n=8), OVX plus MPA (MPA, n=8), OVX plus combined CEE and MPA (CEP, n=7). All drugs were mixed with commercially available strawberry jelly and fed to the rats daily for the 2 months. Each rat consumed 3 mL of the jelly or drug/jelly combination daily for the 2-month treatment phase of the study. Dosages of the drugs were calculated based on the normal daily dosage of Prempro for postmenopausal women (CEE, 0.625 mg, and MPA, 2.5 mg). To determine the dose for rats, we made our calculations assuming the average daily weight for women is 60 kg. Plasma hormone levels were obtained before killing to insure that normal estrogen levels, ranging from 17±2 to 88±2 pg/mL, and progesterone levels, ranging from 2±2 to 46±7 ng/mL, were achieved (Butcher et al, 1974). During the drug-treatment phase, rats were weighed daily and the drug dosage was adjusted accordingly. Rats in the OVX group were fed only the strawberry jelly daily.
Experimental Design
All rats were anesthetized with halothane (4% induction and 1% to 1.5% maintenance) plus oxygen-enriched air via nose cone, and they were prepared for reversible middle cerebral artery occlusion (MCAO) using the intraluminal filament (4–0 nylon monofilament suture) model, as previously described (Alkayed et al, 1998). Lines were inserted into a femoral vein and artery for fluid administration and blood pressure monitoring. Briefly, the scalp was reflected back to expose the skull, the bone was thinned, and a laser-Doppler flowmetry (LDF) probe was fixed over the right parietal cortex 2 mm posterior and 6 mm lateral to the bregma. After exposure of the right common carotid artery, ligation of the external carotid and pterygopalatine arteries, and cauterization of the occipital branch, the occluding suture was threaded through the common carotid artery until the LDF signal was abruptly reduced to less than 60% of the original flow values. Ischemia was maintained for 120 min and the suture was withdrawn to restore perfusion. Throughout the ischemic period, rectal and temporalis muscle temperatures were maintained at approximately 37.5°C by the use of heat lamps. During the recovery period, supplemental Lactated Ringers solution and oxygen were administered to the rats as needed. Rats were allowed to recover for 22 h of reperfusion. At the end of 22 h, rats were deeply anesthetized with halothane and their brains were harvested, sectioned into 7 2-mm-thick coronal slices, and stained with 2,3,5-triphenyltetrazolium chloride. Infarct volume was quantified using standard photography and digital planimetry (Sigmascan Pro, Jandel Scientific, San Rafael, CA, USA). Each section was measured and numerically integrated over the entire right hemisphere for both cortex and caudate putamen. Finally, the infarct volume was expressed as a volume percentage of the ipsilateral structure.
At the end of 22 h before killing, blood samples were obtained for determination of plasma hormone concentrations. Hormone levels were quantified using a commercial radioimmunoassay (Coat-a-Count, Diagnostic Products Corp., Los Angeles, CA, USA), as previously described (Palmon et al, 1998).
Statistical Analysis
All data are expressed as mean±s.d. All variables were analyzed using one-way ANOVA with Neuman–Kuels post hoc tests. The level of significance was set at P⩽0.05.
Results
The mean arterial blood pressure, pO2, pCO2, oxygen saturation, and hemoglobin did not vary among groups. During occlusion, cortical flow, as measured by LDF, decreased to less than 40% of baseline flow in all groups; and no differences were noted between groups, thus confirming ischemia. Plasma hormone levels were within the expected ranges for the groups (OVX, 10.92±5.92; CEE, 12.06±10.88; MPA, 9.7±13.61; and CEP, 30.04±10.75 pg/mL), as were the plasma progesterone levels (OVX, 12.58±6.0; CEE, 2.8±5.54; MPA, 17.52±7.83; CEP, 38.45±30.29 pg/mL).
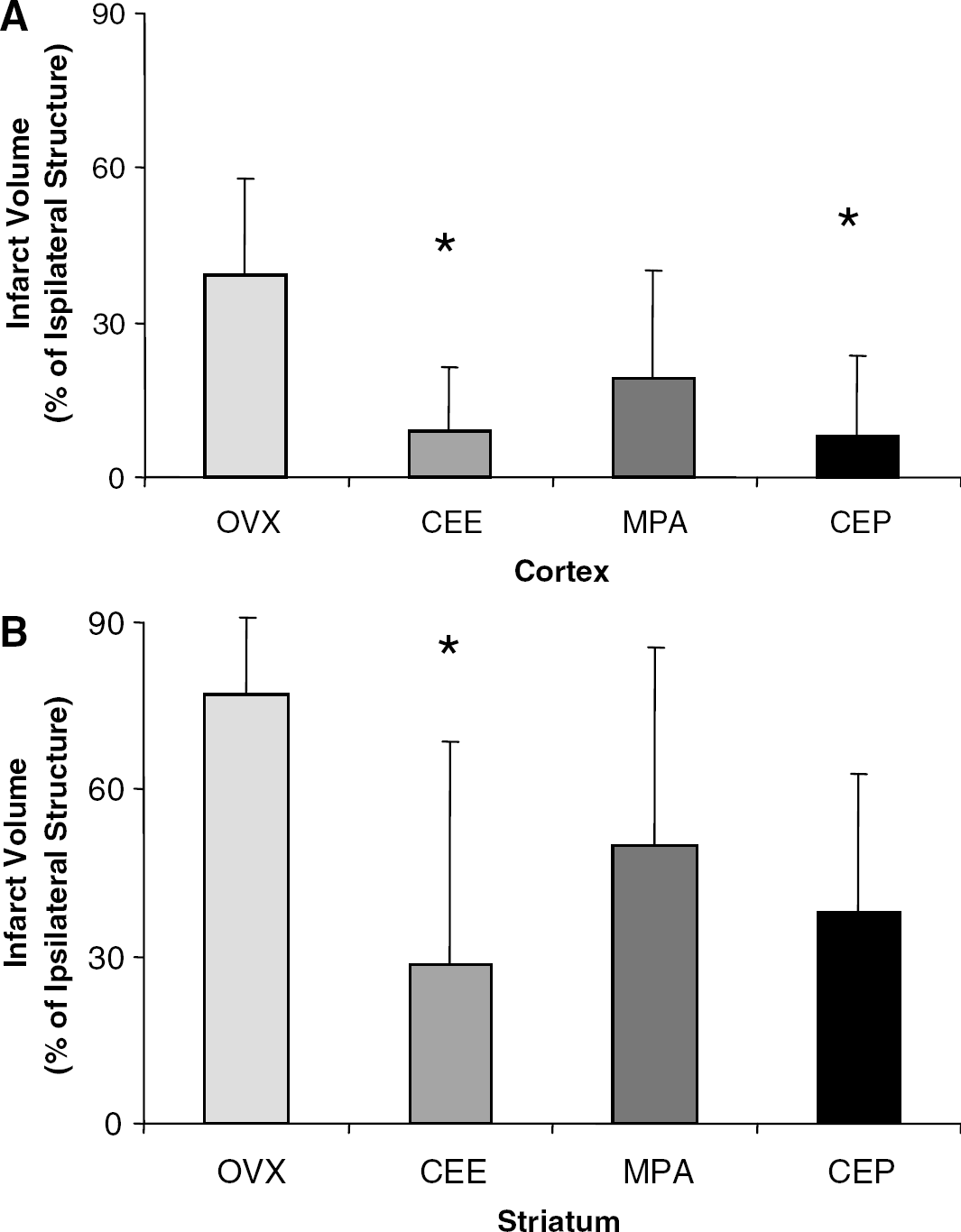
Cortical infarction volume in the CEE, MPA, and CEP groups was compared with that in the OVX rats (Figure 1A). Rats treated with CEE and CEP showed reduction in infarction volume relative to the OVX group. In contrast, in the striatum, only the rats in the CEE group showed a reduction in infarction volume (Figure 1B).
(
Discussion
In this study, we showed three major findings. First, prolonged daily oral CEE in doses relevant to those administered to healthy postmenopausal women reduces both cortical and subcortical infarct volume in rats. Second, the combination of oral CEE and MPA also shrinks infarction volume in the cortex, but not in the caudate-putamen. Third, treatment with MPA alone neither reduces nor increases the degree of cortical or striatal infarction volume after focal stroke. By feeding rats daily doses of ovarian hormones over 2 months, we were able to achieve plasma estrogen and progesterone concentrations within physiologically relevant ranges of normally cycling young rats. Our findings suggest that after experimental focal stroke, long-term oral CEE, but not MPA, provides neuroprotection in a manner similar to parenterally or subcutaneously administered 17β-estradiol. Further, the addition of MPA to CEE may have regional effects in the brain, as the combined hormones counteract the protective effects of CEE in subcortical regions.
Although a variety of animal models establish estrogen as a neuroprotectant after cerebral ischemic injury, the hormone's effect in postmenopausal women remains controversial. Results of the recent study by the Women's Health Initiative (WHI) suggest that oral therapy with CEE alone or in combination with MPA can actually worsen risk for ischemic stroke in healthy postmenopausal women over 60 years (Wassertheil-Smoller et al, 2003; Anderson et al, 2004). However, to our knowledge, no animal studies have used a model that conforms to the prolonged HRT regimens used by humans.
In this study, our overall goal was to model long-term oral HRT in estrogen-deficient rats to determine if lengthy hormone treatment worsens or improves cerebral ischemic injury. Data from the present study confirm and extend the results of previous studies, showing a 10% to 30% reduction in cortical infarction volume with subcutaneous 17β-estradiol alone (Toung et al, 1998) and in combination with acute, intraperitoneal progesterone (Toung et al, 2004). To our knowledge, this is the first study to demonstrate that long-term oral CEE alone or co-administered with MPA reduces cortical lesion volume following experimental focal stroke. Unlike 17β-estradiol, which has been almost exclusively employed in studies of experimental stroke, as many as 10 estrogens (including 17β-estradiol) comprise the CEEs routinely prescribed for postmenopausal women (Bhavnani, 2003), and each of these estrogens may have different effects. When administered orally, the hormones undergo a first-pass effect through the liver, which may significantly lower their biologically active concentrations. Once absorbed in the gut, the hormones are at their highest concentration befire reaching the liver. Passage through the liver increases hepatic synthesis of steroid hormone-binding globulin that can lower bioavailability by binding free hormone (Bhavnani, 2003). Reduction in the amount of free, biologically active hormone may reduce the protective effects of CEE following stroke. Our data indicate that CEE, despite the potential decrease in bioavailability as a result of the first-pass effect, attenuates cerebral ischemic injury in rodents. It is not clear if CEE doses taken by postmenopausal women produce dose-dependent effects, as the WHI examined only one dose—0.625 mg/day. Earlier studies from our laboratory reveal that estrogen-induced protection after focal stroke is concentration dependent (Rusa et al, 1999). Although we attempted to mirror the normal CEE doses given to postmenopausal women and we achieved normal physiologic hormone levels for rat, it is possible that higher doses of CEE worsen infarct volume.
The predominant effects of synthetic progestins, such as MPA, on the brain remain controversial and it is unclear if coadministration of progestins with estrogen negates estrogen's beneficial effects in the postischemic brain. Data from the present study indicate that MPA alone has neutral effects on postischemic infarction volume in both the cortex and in the striatum. However, in contrast to the protective effects of oral CEE alone, combination oral CEE with MPA blocks estrogen's ability to reduce infarction volume in striatal brain regions. These findings differ from those of our previous observations regarding the effects of estrogen (subcutaneous) combined with progesterone (intraperitoneal) therapy in reproductively senescent rats. In those studies, we found that neither estrogen alone nor estrogen combined with progesterone alters the degree of striatal injury after stroke in reproductively senescent females (Toung et al, 2004). Several factors may contribute to the different outcomes of the present study: (1) oral versus parenteral progesterone administration; (2) administration of the synthetic progestin MPA, as opposed to progesterone; and (3) differential metabolism of progesterone as a consequence of aging.
The recent findings of Gibson and Murphy (2004), showing the positive effects of natural progesterone on infarct volume and cognitive function after 60 mins MCAO, are very interesting in light of our current data. However, the design of their study differs from ours in several ways. We studied only female OVX rats subjected to a more severe injury (120 mins) and attained physiologically relevant plasma hormone levels over a 2-month period. Although Gibson and Murphy did not measure plasma progesterone, they likely achieved much higher progesterone concentrations immediately after stroke injury than were reached in the present study. In addition to differences in gender and injury, another possible explanation for the dissimilarity in the two studies may surround acute versus prolonged natural progesterone therapy, not MPA. However, in an earlier study in which progesterone was administered immediately at the onset of reperfusion, we noted a similar reduction in cortical, not striatal, infarct volume of OVX female rats that were subjected to 120 mins MCAO (Murphy et al, 2002). Similar to our data from stroked reproductively senescent female rat, our current findings suggest that long-term therapy with synthetic progestins, has little effect on the degree of brain infarction volume.
In injured brain, coadministration of MPA with CEE may reverse estrogen's favorable effects on migratory inflammatory cells and potentiate vascular endothelial disruption (Xing et al, 2004) or heighten glutamate-induced excitotoxic injury (Nilsen and Brinton, 2002a, 2002b). Alternatively, it is possible that subcortical brain regions may be more dependent on blood flow, making striatum more susceptible to postischemic vascular obstruction. Another potential effect of MPA may be related to enhanced cerebral microvascular thrombosis, as oral MPA has been shown to accentuate prothrombic side effects in female rats (Mimura et al, 2003) and to heighten procoagulant response to thrombin (Herkert et al, 2001). Finally, MPA may have differential effects in the striatum because of differences in progesterone-receptor distribution or increased vulnerability to excitotoxic injury subsequent to accumulation of MPA metabolites in the striatum compared with the cortex (Ciriza et al, 2004).
In these studies, we examined the effects of hormone preparation, route, and long-term administration using stroke lesion volume as an outcome measure, as brain lesion size has been reported to correlate with early functional outcomes in rat (Rogers et al, 1997). However, assessment of stroke lesion has been reported to be of limited value in murine MCAO models (Reglodi et al, 2002; Hattori et al, 2000). In murine MCAO models, specific functional and cognitive tests have been shown to better correlate with injury severity up to 21 days (Gibson and Murphy, 2004). It is possible that prolonged HRT produces different effects on brain lesions but we did not capture any of these effects during our window of observation. Further, our studies do not address the more complicated issues surrounding the effects of prolonged HRT on neurologic or behavioral recovery.
Conclusions
It is unclear why estrogen is strongly protective in various estrogen-deficient animal models while seemingly detrimental in postmenopausal women. The present study was designed to ascertain if prolonged oral hormone administration of CEE, MPA, or the CEE/MPA combination reverses the protection conferred by parenteral estrogen alone, which has been reported in the rat MCAO focal stroke model. To our knowledge, the present study is the first to examine this issue. During our window of observation, our findings suggest that daily oral estrogen alone, or combined with MPA, effectively reduces the cortical injury associated with stroke. However, in subcortical brain regions, CEE is blocked by coadministration with MPA, suggesting a nonbeneficial interactive effect with CEE. In light of the ongoing controversy surrounding hormone replacement regimens in women, the current study is timely and a first step toward determining if prolonged HRT alters postischemic brain injury. Further studies are needed to examine the effects of prolonged HRT on long-term neurologic and behavioral outcomes.
Footnotes
Acknowledgements
The authors gratefully acknowledge the fine editorial assistance provided by Tzipora Sofare, MA, in the preparation of this manuscript.