
Abstract
We investigated the effects of hormone replacement therapy (HRT) on frontal cerebral blood flow (CBF), depressive symptoms, and cognitive function in depressed postmenopausal women. Fourteen postmenopausal women with depressive symptoms underwent HRT, and seven controls not undergoing HRT were studied. We evaluated frontal CBF, expressed as frontal/cerebellum (F/C) ratio, using Tc-99m hexamethyl propylene amine oxime single photon emission computed tomography (Tc-99m HMPAO SPECT), cognitive function using the Mini-Mental Status Examination (MMSE), and depression using the HAD (Hospital Anxiety and Depression) scale. All studies were carried out at initial status and after 9 months. Single photon emission computed tomography was performed at rest and at activation during the Wisconsin Card Sorting Test (WCST). Initial frontal CBF was not different between groups. After 9 months, resting frontal CBF was similar between groups. However, activated frontal CBF was significantly higher in the HRT group than in controls (F/C ratio: 0.924±0.04 versus 0.853±0.05, P=0.007). Furthermore, the increase in the activated F/C ratio was inversely associated with years since menopause. Mini-Mental Status Examination scores improved after HRT, but depression scores did not. Hormone replacement therapy improved frontal CBF and cognitive function but not depression in postmenopausal women. The changes in frontal CBF were detected only during WCST activation and were most apparent during early postmenopausal years.
Keywords
Introduction
Symptoms of depression are common in postmenopausal women (Pan et al, 2002). Estrogen deficiency may be involved in postmenopausal depression, and hormone replacement therapy (HRT) may improve mood and cognition (Birkhauser, 2002). In healthy menopausal women, HRT increases cerebral blood flow (CBF), both global and regional, and cognitive function (Resnick et al, 1998; Greene, 2000). However, it is not clear how HRT changes CBF in depressed menopausal women.
Functional brain imaging using Tc-99m hexamethyl propylene amine oxime (Tc-99m HMPAO) and single photon emission computed tomography (SPECT) is used to assess regional CBF and to understand regional brain function (Kocmur et al, 1998). Many SPECT studies have shown a decreased frontal CBF in depressed patients, and some have suggested an association between decreased frontal CBF and decreased cognitive function in depressed patients (Bench et al, 1995; Bonne et al, 1996; Hornig et al, 1997; Kocmur et al, 1998).
In a previous study (Yao et al, 2008), we showed a decrease in frontal CBF in depressed postmenopausal women. In this study, we investigated whether HRT improves frontal CBF, mood, and cognitive function in depressed postmenopausal women and, if so, how such improvements are related.
Materials and methods
Patients
Written informed consent was obtained from each participant before the study began. All protocols were approved by the Human Experiment Ethics Committee of our hospital. A total of 21 depressed postmenopausal women, aged between 42 and 65 years, referred from our hospital's Department of Obstetrics and Gynecology were included in this study. Individuals with a history of seizure, major head trauma, cerebral vascular disease, cardiovascular disease, or neurologic disorder were excluded, as were those who had received HRT or were currently taking neuroleptic, analeptic, or anticonvulsant drugs. The postmenopausal condition was defined as the absence of menses for 12 months or the absence of menses for 6 months, but with plasma levels of >40 IU of the follicular stimulating hormone (FSH) and <30 pg/mL of estradiol (E2) (Kocmur et al, 1998; Alptekin et al, 2001).
A total of 14 postmenopausal women with various degrees of depression underwent HRT for 9 months. Seven age- and symptom-matched controls not undergoing HRT were selected for comparison. The HRT consisted of the administration of conjugated estrogens (Premarin, Wyeth Pharmaceuticals, Philadelphia, PA, USA) (0.625 mg) and medroxyprogesterone acetate (5 mg) daily.
Clinical Assessment
A magnetic resonance image of each patient's brain was taken. Each participant was tested for plasma FSH and E2 levels and was subjected to brain SPECT studies before and after HRT. All participants received a semi-structured diagnostic interview on the basis of the Taiwanese version of the SCAN (Schedule for Clinical Assessment in Neuropsychiatry), and a diagnosis of depression was made according to the criteria of the DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, 1994). The Wisconsin Card Sorting Test, computer version 2 (WCST-CV2), was used to activate frontal CBF. The MMSE (Mini-Mental Status Examination) was conducted to evaluate cognitive function, and the Hospital Anxiety and Depression (HAD) scale was used to evaluate depression.
Measuring Plasma Estradiol and Follicular Stimulating Hormone Levels
Plasma E2 levels were determined using a solid-phase radioimmunoassay estradiol kit (Diagnostic Products Corporation, Los Angeles, CA, USA) with a detection limit of ∼8 pg/mL. Plasma FSH levels were determined using an immunoradiometric assay kit (Diagnostic Products Corporation) with a detection limit of ∼0.06 mIU/mL.
Wisconsin Card Sorting Test
The WCST was used to study frontal activation. During the WCST, all participants were required to match response cards to four stimulus cards along with one of three dimensions (color, form, or number) on the basis of verbal feedback (correct or wrong) without giving any information about the dimensions. Once the subject sorted a series of 10 cards by one category, the subject was asked to sort the cards again by a different category. There were 64 cards in this test. All definitions of indices are described in the WCST manual (Heaton et al, 1993).
Magnetic Resonance Imaging
A magnetic resonance imaging brain scan was taken (Magneton 1.5 T Scanner; Siemens Medical Systems, Iselin, NJ, USA) to detect any structural abnormalities and for image registration. On the magnetic resonance images, we found no structural abnormalities—e.g., brain atrophy or cerebrovascular disease—that might have influenced the interpretation of CBF measurement.
Tc-99m HMPAO SPECT Imaging
We conducted two Tc-99m HMPAO SPECT assessments, at rest and in the activated state, both before and after HRT. All patients were assessed between 0830 and 1030 hours. For the resting SPECT measurement, patients were injected with Tc-99m HMPAO while recumbent in a quiet, darkened room with their eyes open and ears unoccluded. For the activation measurement, patients were injected with Tc-99m HMPAO while they were undergoing WCST-CV2, and imaging was carried out immediately after WCST was conducted. To determine regional CBF, a dose of 740 MBq (20 mCi) of Tc-99m HMPAO (Ceretec, Nicomed-Amersham, Marlow, Buckinghamshire, UK) was injected into each patient's antecubital vein. Single photon emission computed tomography imaging was initiated using a triple-headed rotating gamma camera (Multispect3; Siemens) with a fan-beam collimator, which yields an image resolution of ∼8.5 mm FWHM (full with at half maximum). SPECT data were acquired over a 360° rotation, 120 steps, 30 secs per step, in a 128 × 128 × 16 matrix. Data were then processed using filtered back projection with Butterworth and Ramp filters to reconstruct the transverse, coronal, and sagittal images. Chang's method of attenuation correction was used. The reconstructed transverse images were aligned parallel to the canthomeatal line. The slice thickness of each transverse image was 2.89 mm.
Semi-Quantitative Analysis
The SPECT images were standardized and registered to a SPECT template image set using Statistical Parametric Mapping (SPM’99; London, UK) (Yao et al, 2008), after which frontal regions of interest were quantified.
To analyze the anterior frontal activity, we composed six registered transverse images, best depictions of the anterior frontal lobe. An independent technician, blinded to clinical information with regard to the patients, drew the regions of interest on the anterior frontal lobe. The average counts of the anterior frontal lobe were then calculated. The same regions of interest were used as templates to analyze the anterior frontal activity for the remainder of the study.
We chose the cerebellum as the reference region for normalizing frontal CBF, because the cerebellum is not pathologically involved in depressed patients and because it provides the best detection of CBF abnormalities (Talbot et al, 1994; Staffen et al, 2009). To analyze cerebellar activity, six consecutive transverse images at mid-cerebellum levels were composed. The average counts of each cerebellum were then calculated. The average anterior frontal counts normalized to cerebellum counts (frontal/cerebellum ratio, F/C ratio) were used to represent relatively anterior frontal CBF.
Clinical assessment, plasma E2 and FSH levels, and Tc-99m HMPAO SPECT were repeated after HRT and 9 months later for the group not administered HRT.
Statistical Analysis
Data were analyzed using a commercial software package (SPSS version 10; SPSS, Chicago, IL, USA). A paired-sample t-test was used to compare parameters before and after HRT. A Mann–Whitney U-test was used to compare differences between those administered and not administered HRT. Pearson's correlation coefficients were used to determine whether CBF was correlated with MMSE, depression scores, E2 levels, and years after menopause.
Results
The HRT and control groups showed no differences in demographic data (Table 1). After HRT, plasma E2 (P=0.001) and FSH (P <0.001) levels were increased (Table 2). Mini-Mental Status Examination scores also increased from 25.6 to 27.2 (P=0.045) (Table 2), but depression and anxiety scales did not (Tables 2 and 3).
Demographic data of participating patients
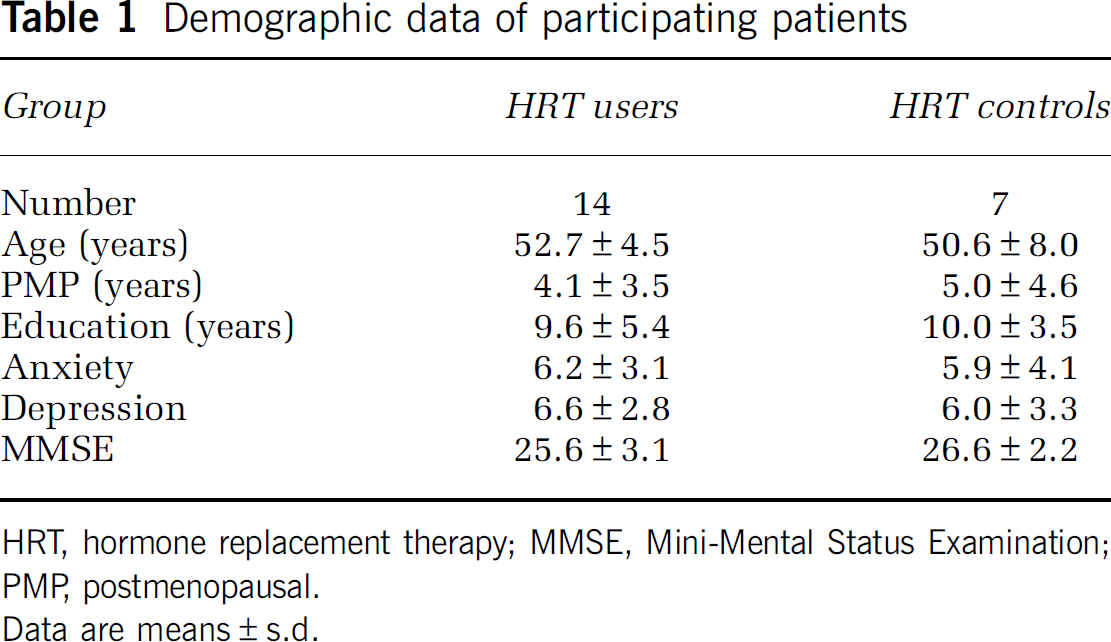
HRT, hormone replacement therapy; MMSE, Mini-Mental Status Examination; PMP, postmenopausal.
Data are means±s.d.
Clinical assessments and endocrine data in patients who underwent hormone replacement therapy (HRT)
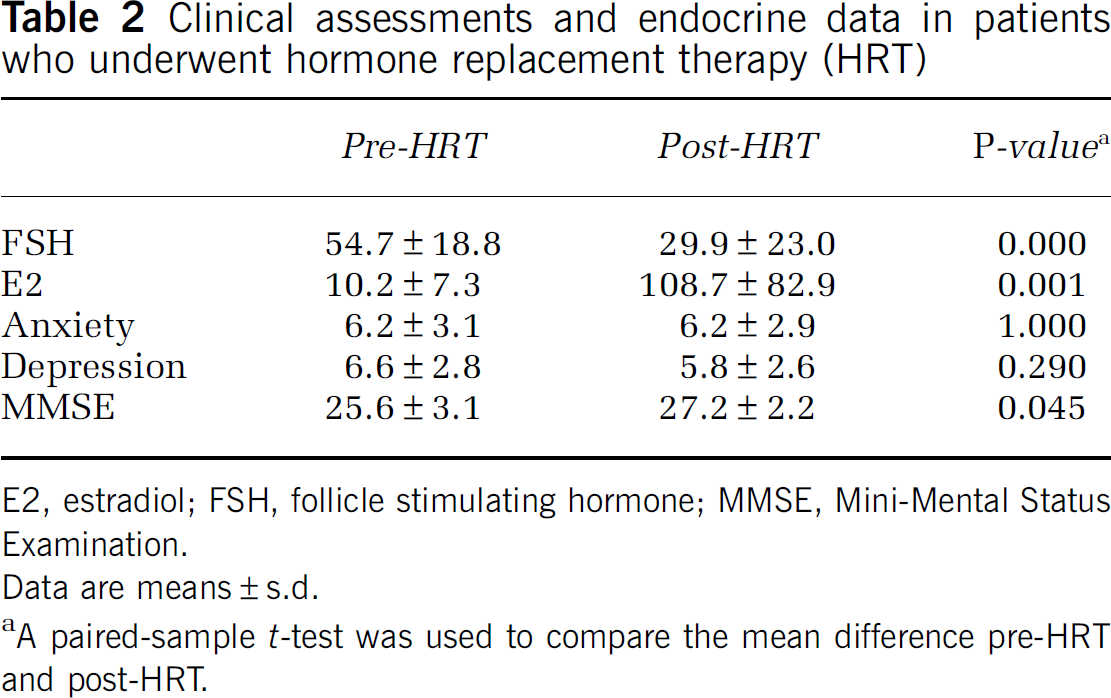
E2, estradiol; FSH, follicle stimulating hormone; MMSE, Mini-Mental Status Examination.
Data are means±s.d.
A paired-sample t-test was used to compare the mean difference pre-HRT and post-HRT.
Clinical assessments and endocrine data in controls
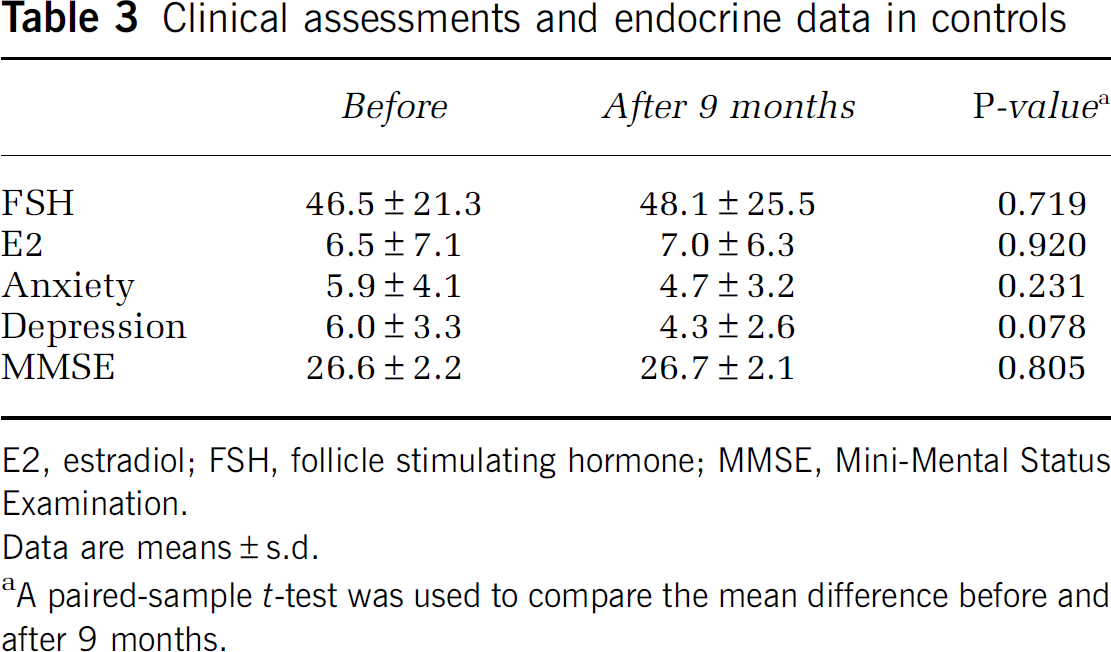
E2, estradiol; FSH, follicle stimulating hormone; MMSE, Mini-Mental Status Examination.
Data are means±s.d.
A paired-sample t-test was used to compare the mean difference before and after 9 months.
After HRT, resting frontal CBF remained unchanged. However, the activated frontal CBF was increased (F/C ratio from 0.890±0.06 to 0.924±0.04, P=0.006) and was higher than that in controls (F/C ratio 0.853±0.05, P=0.007) (Table 4). Furthermore, the change in activated F/C ratio was inversely associated with years since menopause (r=−0.573, P=0.032) (Figure 1). There was no significant change in resting or activated frontal CBF in controls after 9 months.
Comparison of baseline and activation frontal cerebral blood flow (F/C ratio) using Tc-99m HMPAO SPECT in participating patients
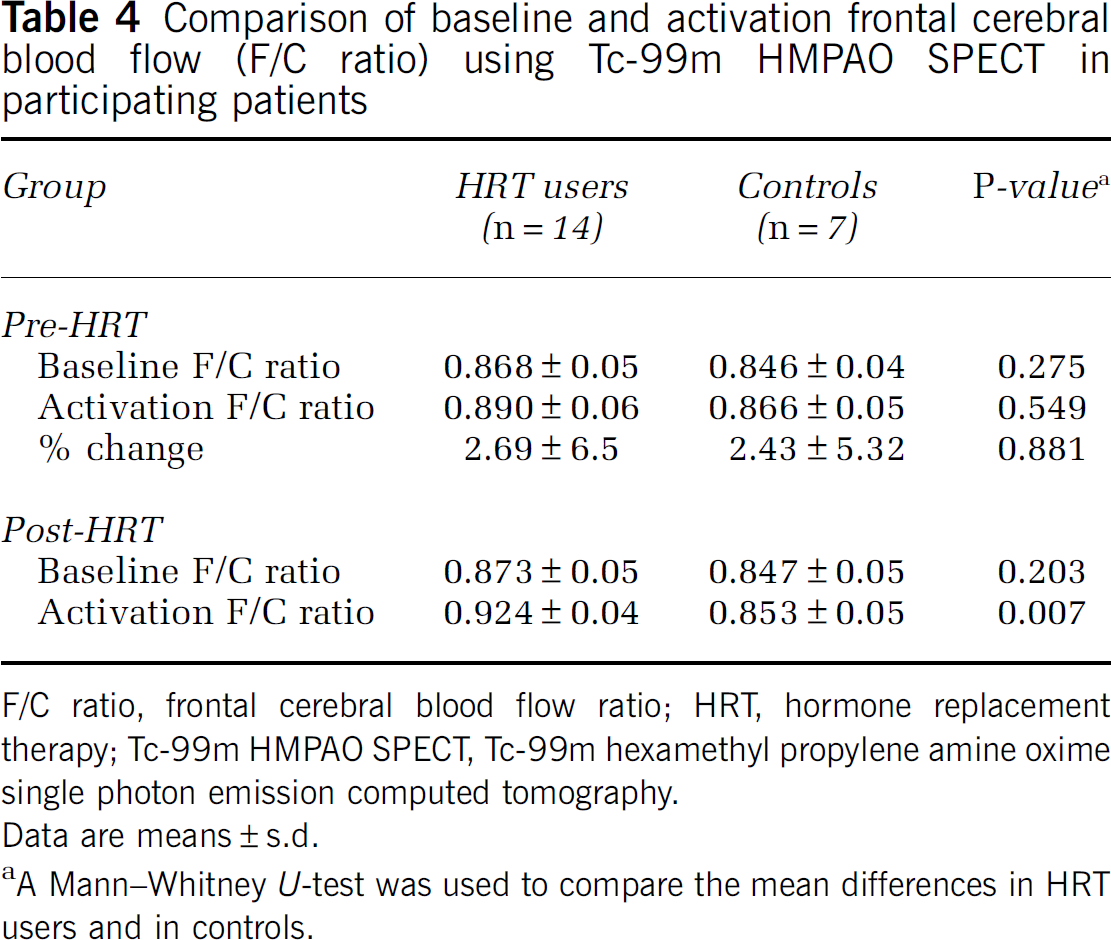
F/C ratio, frontal cerebral blood flow ratio; HRT, hormone replacement therapy; Tc-99m HMPAO SPECT, Tc-99m hexamethyl propylene amine oxime single photon emission computed tomography.
Data are means±s.d.
A Mann–Whitney U-test was used to compare the mean differences in HRT users and in controls.
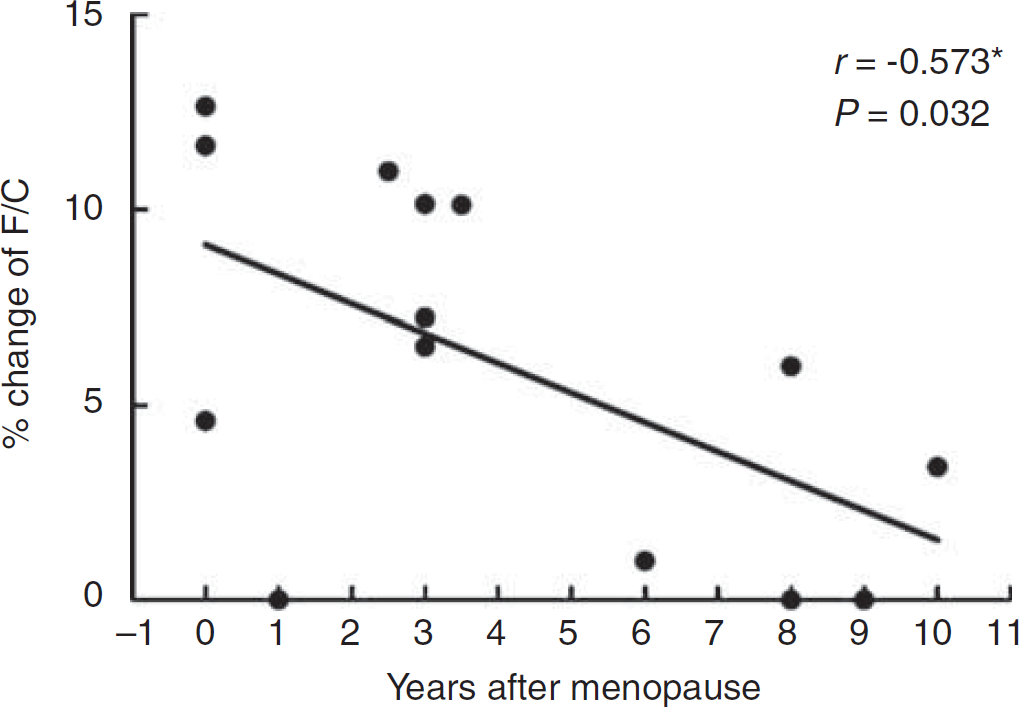
Association of years after menopause with the percentage change in frontal cerebral blood flow in patients who underwent hormone replacement therapy (% change of F/C=(F/C after HRT−F/C before HRT)/F/C before HRT × 100%).
Discussion
Using Tc-99m HMPAO SPECT imaging, we showed that HRT improved frontal CBF and cognitive function but not depression in postmenopausal women.
It is well known that depressed patients have several abnormalities in regional CBF and glucose metabolism in various brain regions, including the prefrontal cortex and the anterior cingulated cortex (Kalia, 2005). In addition, several studies (Marenco et al, 1993; Yang et al, 2003; Ortuno et al, 2006) have shown that in healthy individuals and in schizophrenic patients, the frontal lobe is physiologically activated above baseline levels when they are taking a cognitive test. Although the neurobiology of depression and cognitive function remains unclear, changes in frontal CBF are the common pathway during mood swings and activating cognitive tests. On the basis of these findings, we speculated that increasing frontal CBF would improve both cognitive function and mood in these menopausal participants.
The mechanism through which HRT increased frontal CBF remains unclear. Estrogen has been reported to increase CBF and reduce vascular resistance (Belfort et al, 1995; Jesmin et al, 2003). In addition, high concentrations of intraneural estrogen receptors were found in the frontal lobe (Thomas et al, 1999). Therefore, because HRT replaces estrogens, it is reasonable to expect the procedure to increase frontal CBF, as shown in this study.
Although other studies (Sorensen et al, 2001; Birkhauser, 2002) showed hormone-related increases in blood flow in healthy elderly women at rest, this study showed HRT-related increases in frontal CBF only during the WCST activation test, but not at rest. To the best of our knowledge, there are no reports on HRT-related CBF in an activated state. This finding emphasizes the importance of the activation test when investigating frontal CBF. Wisconsin Card Sorting Test activation of the frontal cortex during task performance is more sensitive for detecting minor differences in frontal CBF than in a resting state.
The effect of HRT on frontal CBF was negatively correlated with number of years since the onset of menopause and was most apparent within 4 years of the onset. These findings provide evidence of a critical period for HRT-related neuroprotection, and support the notion that the earlier that HRT is initiated in menopausal women, the better will be their cognitive improvement. The popularity of HRT users has decreased after the Women's Health Initiative (WHI) report of breast cancer risk (Chlebowski et al, 2003). However, the biggest concern is that the women in the WHI were much older and started HRT too late in life. On the basis of the results of our study, and with regard to the WHI results, we suggest that HRT is effective for relief of menopausal symptoms and should be individualized on the basis of the needs of each woman. Second, HRT should be used early in menopausal years with short duration. Finally, HRT users should undergo an annual breast examination with either mammography or breast ultrasound.
Consistent with previous reports (Ohkura et al, 1994; Hogervorst et al, 2002), we found an improved cognitive function in menopausal women after HRT. Recent animal studies have suggested biologic mechanisms through which estrogen may maintain neuronal function (Dubal and Wise, 2001). Several community-based studies (Binder et al, 2001; Carlson et al, 2001) also showed the beneficial effects of HRT on cognitive function in elderly women with and without Alzheimer's disease. Our finding strengthens the idea that using HRT to maintain high levels of estrogen in postmenopausal women might protect them from cognitive decline. The mechanism of this protective effect remains unknown. It might be the neural, metabolic, or vascular benefits of estrogen (Collins, 1996). This study showed that HRT increased both frontal CBF and cognitive function, suggesting that increased frontal CBF is associated with improved cognitive function.
Using HRT to treat depression in menopausal women is still controversial (Whooley et al, 2000). Although some studies (Zweifel and Obrien, 1997; Miller, 2003) suggest that HRT augments serotonergic activity and facilitates the improvement of clinical depression and the efficacy of antidepressants, other studies (Pearce et al, 1997) do not report an antidepressant effect from HRT. This study showed that HRT alone did not alleviate depressive symptoms in menopausal women.
Although the sample size was small, statistical power was above 80% because of a small inherent variability of the primary outcome variable. No placebo was used in the control group. The placebo effect of administering antidepressants may not be entirely ruled out. The significance might be eliminated had the placebo effect been controlled in the design phase.
In conclusion, we showed that 9 months of HRT improved frontal CBF and cognitive performance but did not alleviate depression in postmenopausal women. The change in CBF was detected only during the activation brought about by the WCST and was most apparent during early postmenopausal years.
Footnotes
Acknowledgements
The authors gratefully acknowledge the financial support from the National Science Council of Taiwan (NSC 90-2314-B-006-098).
The authors declare no conflict of interest.