
Abstract
Introduction
Exertional heat stroke is a life-threatening emergency necessitating immediate treatment with rapid body cooling. A field-expedient alternative may be tarp-assisted cooling, requiring only water and a tarp. The objective of this study was to compare core temperature (Tc) cooling rates of tarp-assisted cooling using the limited resources available to a wildland firefighter and the current standard care provided in wilderness settings.
Methods
This cross-over, randomized control trial of 17 healthy individuals consisted of exercise in a 42±1°C, 32±4% relative humidity environment while wearing wildland firefighter attire, followed by cooling. Body cooling consisted of either pouring 11 L of 25±1°C water over the torso while lying supine on a tarp configured to hold water close to the individual (Tarp) or dousing the water on the participant followed by lying supine with a light breeze, current standard care in the wilderness (Current Care). Cooling occurred until Tc reached 38°C.
Results
Participants walked until a similar Tc was achieved in Tarp (39.59±0.04°C) and Current Care (39.55±0.22°C; P=0.36). Core temperature cooling rate was not different between Tarp (0.076±0.042°C·min−1) and Current Care (0.088±0.046°C·min−1; P=0.41).
Conclusions
In hyperthermic individuals, Tarp did not provide a faster cooling rate compared to the current exertional heat stroke care provided in the wilderness, and both provided a slower cooling rate than that provided by the traditional method of cold water immersion (>0.20°C·min−1) to treat exertional heat stroke patients.
Introduction
Wildland firefighting consists of long-duration, high-intensity work with heavy equipment (eg, hiking, building fire lines, chainsaw work, brush removal) in a hot environment, placing wildland firefighters at risk of exertional heat stroke (EHS). 1 -5 Exertional heat stroke is a life-threatening emergency commonly induced by high-intensity physical activity leading to a dangerously high body temperature and potentially resulting in endotoxemia, multiorgan dysfunction, and death if not treated immediately with rapid body cooling. 6 Core temperature (Tc) reduction to <39°C (102°F) within 30 min of collapse results in 100% survival and positive outcomes and prognosis. 7 -10 While temperature reduction is easily achieved with whole-body cold water immersion, this modality is not feasible in the wilderness unless a cold natural body of water is nearby. When it is unavailable, the current recommendation by the Wilderness Medical Society is to remove excess clothing, douse the patient with any available water, and provide fanning while evacuating the patient to advanced medical care. 9 While certainly an option, this cooling strategy results in a suboptimal cooling rate, 11 and evacuation could take well over an hour, as the meeting point could be miles away from the incapacitated patient. Considering these limitations, EHS patients with extreme hyperthermia can experience adverse long-term health consequences when survival is possible.
A field-expedient EHS cooling method that has been implemented in outdoor settings is tarp-assisted cooling, requiring only water and a tarp. Briefly, the EHS patient lies supine on a tarp with the sides held vertically to ensure that the water remains near the torso. Cooling rates of hyperthermic individuals when this method is implemented are promising, indicating that large volumes (76–151 L) of cold water (2–9°C) allow for cooling rates of 0.14 to 0.17°C·min−1. 11 -13 Tarp-assisted cooling implemented in a military setting with a large volume (80 L) of temperate water (27°C) has shown a greater cooling rate compared to that achieved with whole-body fanning while wearing or not wearing a wet T-shirt. 14 While these results are promising, implementing tarp-assisted cooling using only the supplies available in the wilderness has not yet been attempted. While initial wildland fire tasks do not include water availability through a hose line, wildland firefighters carry drinking water and a space blanket or fire shelter that can be used as a tarp.
The life-threatening nature of EHS warrants investigation into the efficacy of tarp-assisted cooling with the limited resources available in the wilderness. Without this critical information, a potentially effective wilderness EHS treatment strategy may go unexplored, resulting in preventable adverse health outcomes. Therefore, the purpose of this study was to compare Tc cooling rates of tarp-assisted cooling using the limited resources available to a wildland firefighter and the current standard care provided in wilderness settings.
Methods
Participants
Seventeen participants (Table 1) were enrolled in this cross-over, randomized control trial. All participants provided informed consent prior to data collection, and the study was approved by the University at Buffalo institutional review board (STUDY00003727) and is registered at
Participant characteristics
Data presented as mean±standard deviation.
P≤0.05 compared to males.
Experimental Trials
Participants abstained from food 1 h before and from exercise, caffeine, and alcohol 12 h before arrival at the laboratory in the morning after drinking 500 mL of water the night before testing and 250 mL of water the hour before testing. Hydration status was confirmed by a urine specific gravity of <1.025 in all participants (Atago, Bellevue, WA). Females were tested during the first 10 d following self-identified menstruation or during the placebo phase of their oral contraceptives, with a negative pregnancy test confirmed before continuation of the trial. Experimental trials were separated by at least 48 h. Six to 8 h prior to each experimental trial, participants swallowed a telemetry pill to measure Tc (HQ, Inc, Palmetto, FL). Participants were instrumented with an HR monitor (Polar Electro, Kempele, Finland) and donned a T-shirt, shorts, wildland firefighting personal protective equipment (Lakeland Industries, Huntsville, AL), athletic shoes, and an 18 kg backpack, a common pack weight carried during wildland fire suppression. 16
Participants stood for 10 min to equilibrate to the environmental chamber (42±1°C, 32±4% relative humidity) that simulated the approximate environment during wildfire suppression.16,17 Participants did not consume food or fluid throughout the trials. Participants briskly walked on a treadmill until one of the exercise termination criteria was met: 1) Tc reached 40.0°C; 2) HR exceeded the age-predicted maximum (208−[0.7×age]) for 5 continuous min; 3) signs and/or symptoms of heat illness; or 4) volitional fatigue (Tarp, N=15; Current Care, N=14).
Upon completion of exercise, participants exited the environmental chamber and entered a warm room (26.7°C, 37% relative humidity), removed all gear and clothing except for undergarments and shorts, and were cooled in a randomized, counterbalanced order: 1) Tarp or 2) Current Care. Tarp consisted of participants lying supine on a plastic tarp with the head and feet elevated and 11 L of 25±1°C water poured on top of the torso. This is the approximate volume and temperature of drinking water that a 5-member wildland firefighting team would have available (conversation with Sanger Fire Department personnel) if EHS occurred 2 h into work (the most likely timeframe) 18 and if all individuals hydrated according to best practice recommendations. 19 Current Care consisted of dousing the participant with water of the same volume and temperature, followed by lying on a cot with a light breeze (0.5 m·sec−1), simulating current standard care. 9 Fan speed was chosen to represent the hiking speed of carrying the EHS patient to advanced medical care. Subjects were removed from cooling when Tc reached 38.0°C (Tarp: N=12, Current Care: N=14) or plateaued for 4 consecutive minutes, determined by a ≤0.01°C reduction in Tc (Tarp, N=3; Current Care, N=0).
Core temperature and HR were recorded throughout exercise and cooling. Perceptions of thermal sensation on a 1 (Cold) to 7 (Hot) scale with 0.5 increments 20 were recorded during cooling and immediately after cooling. Nude body mass after toweling dry was measured before and after the trial to calculate sweat rate and percent body mass loss during exercise.
Statistical Analysis
Fifteen individuals completed both trials; however, among these 15 participants, 2 trials (1 Tarp, 1 Current Care) resulted in a Tc of <39°C at the onset of cooling and 1 trial (Tarp) had a mistakenly high water temperature, leading to not using these data. Additionally, 2 participants completed only the Tarp trial before dropping from the study. Therefore, this article includes 15 Tarp and 14 Current Care trials included in group means, with data from the 12 participants who completed both trials included in paired analyses. The study was underpowered to compare responses of males and females; therefore, trends and effect size (ES) for each sex are reported separately. Effect size determined the magnitude of difference of comparisons using Hedges’ g equation and was interpreted as small (0.00–0.49), moderate (0.50–0.79), or large (>0.80).
Two-way (treatment by time) repeated measures analysis of variance was used to compare Tc throughout cooling. Paired samples t tests were used to compare physiological responses to exercise and cooling. Two-min cooling rate epochs were calculated and compared between treatments to quantify changes in rates throughout cooling. Perceptual responses to cooling were analyzed using Wilcoxon signed-rank tests. Pearson’s product-moment correlations were run to determine relationships between cooling rate and physical characteristics. Data are presented as mean±SD. Statistical analyses were performed using SPSS software (version 26, IBM SPSS Statistics, Chicago, IL) with α=0.05.
Results
Exercise
Participants began the trials hydrated (urine specific gravity: Tarp, 1.013±0.009; Current Care, 1.012±0.008; P=0.49) with similar body mass (Tarp, 69.57±14.02 kg; Current Care, 69.19±13.29 kg; P=0.49) in Tarp and Current Care. Upon exercise commencement, Tarp and Current Care Tc (Tarp, 37.42±0.23°C; Current Care, 37.35±0.24°C; P=0.22), HR (Tarp, 120±14 b·min−1; Current Care, 115±9 b·min−1; P=0.11), and thermal sensation (Tarp, 5±1; Current Care, 5±1; P=0.10) were not different. Participants walked (Tarp, 69±13 min; Current Care, 74±13 min; P=0.09), with end of exercise Tc (Tarp, 39.59±0.04°C; Current Care, 39.55±0.22°C; P=0.36), HR (Tarp, 180±11 b·min−1; Current Care, 178±11 b·min−1; P=0.33), and thermal sensation (Tarp, 7±0; Current Care, 7±0; P=0.66) not different between Tarp and Current Care. Sweat rate (Tarp, 1.1±0.5 L/h; Current Care, 1.0±0.5 L/h; P=0.09) and percent body mass loss (Tarp, 2±1%; Current Care, 2±1%; P=0.63) were not different between Tarp and Current Care.
Cooling
Participants began cooling in a similar physiological state, with Tc (Tarp, 39.59±0.17°C; Current Care, 39.50±0.18°C; P=0.06) (Figure 1), HR (Tarp, 118±13 b·min−1; Current Care, 123±17 b·min−1; P=0.25) (Figure 2), and thermal sensation (Tarp, 5±1; Current Care, 5±1; P=0.26) not different between Tarp and Current Care. Core temperature was reduced over time (P<0.01) but was not different between trials (P=0.45). Core temperature cooling rate (Tarp, 0.076±0.042°C·min−1; Current Care, 0.088±0.046°C·min−1; P=0.41) (Figure 3) was not different between Tarp and Current Care. Males trended toward a greater cooling rate and displayed a moderate ES with Current Care (0.107±0.059°C·min−1) compared to Tarp (0.076±0.044°C·min−1; P=0.07, ES=0.71). Females did not have a difference in cooling rate and had a small ES between Tarp (0.086±0.050°C·min−1) and Current Care (0.070±0.020°C·min−1; P=0.51; ES=0.26). Cooling duration from cooling commencement until Tc reached 38.0°C was 25.6±10.5 min (Tarp) and 21.2±11.1 min (Current Care) (P=0.31). Change in Tc from start of cooling to 10 min (Tarp, 1.04±0.41°C; Current Care, 1.04±0.40°C; P=0.98) and 15 min (Tarp, 1.49±0.66°C; Current Care, 1.46±0.49°C; P=0.83) of cooling and total change in Tc (Tarp, 1.57±0.15°C; Current Care, 1.50±0.18°C; P=0.08) were not different between Tarp and Current Care. Females trended toward a greater change in Tc and had a large ES with 10 min of cooling in Tarp (1.20°C) compared to Current Care (0.86°C; P=0.09; ES=0.81). Thermal sensation was warmer at the end of cooling in Current Care (4.0±0.5) compared to Tarp (3.5±0.5; P=0.01).
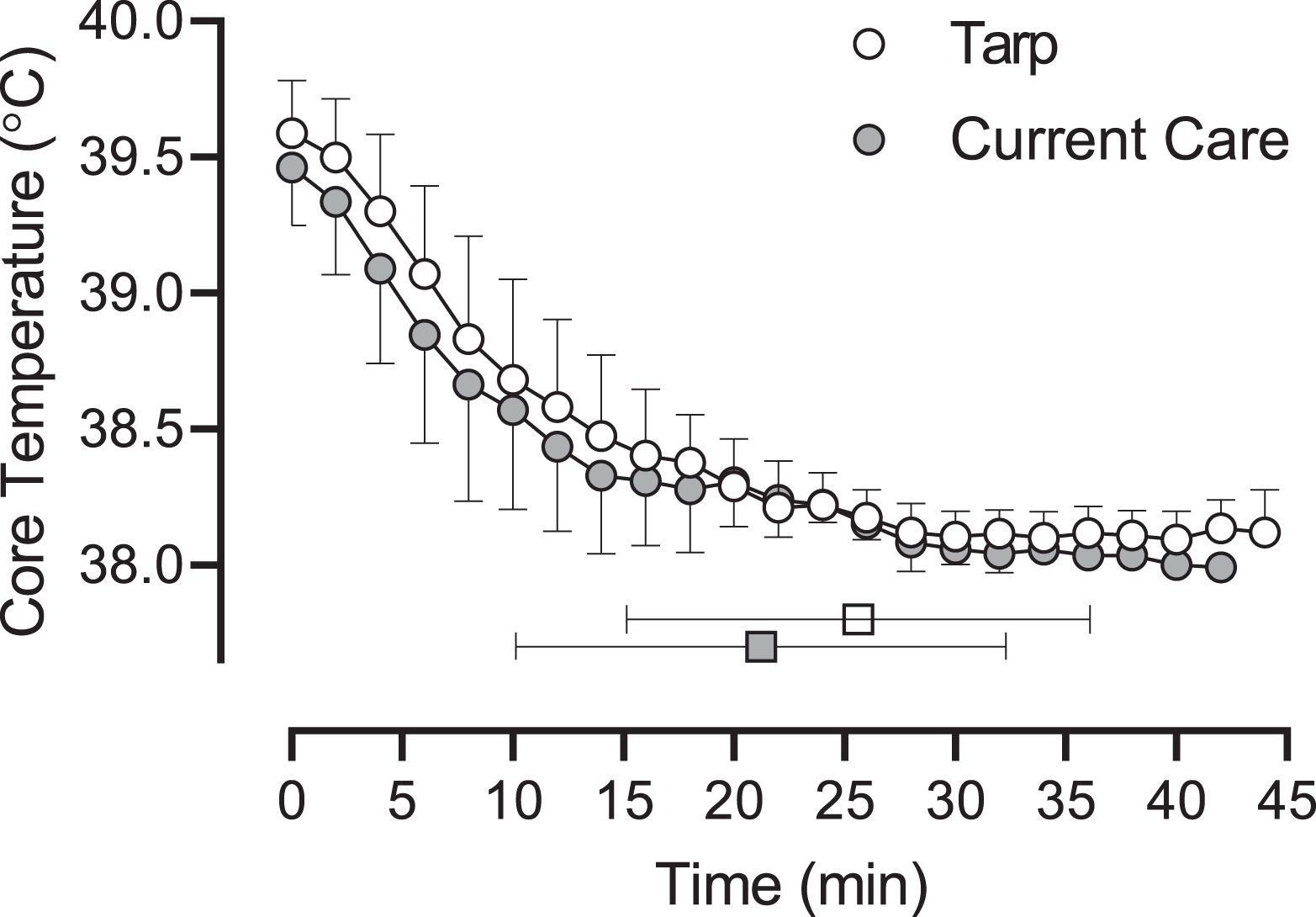
Core temperature during cooling using tarp-assisted cooling (Tarp) or Current Care. White and gray squares indicate average time to cool to 38°C in Tarp and Current Care, respectively.
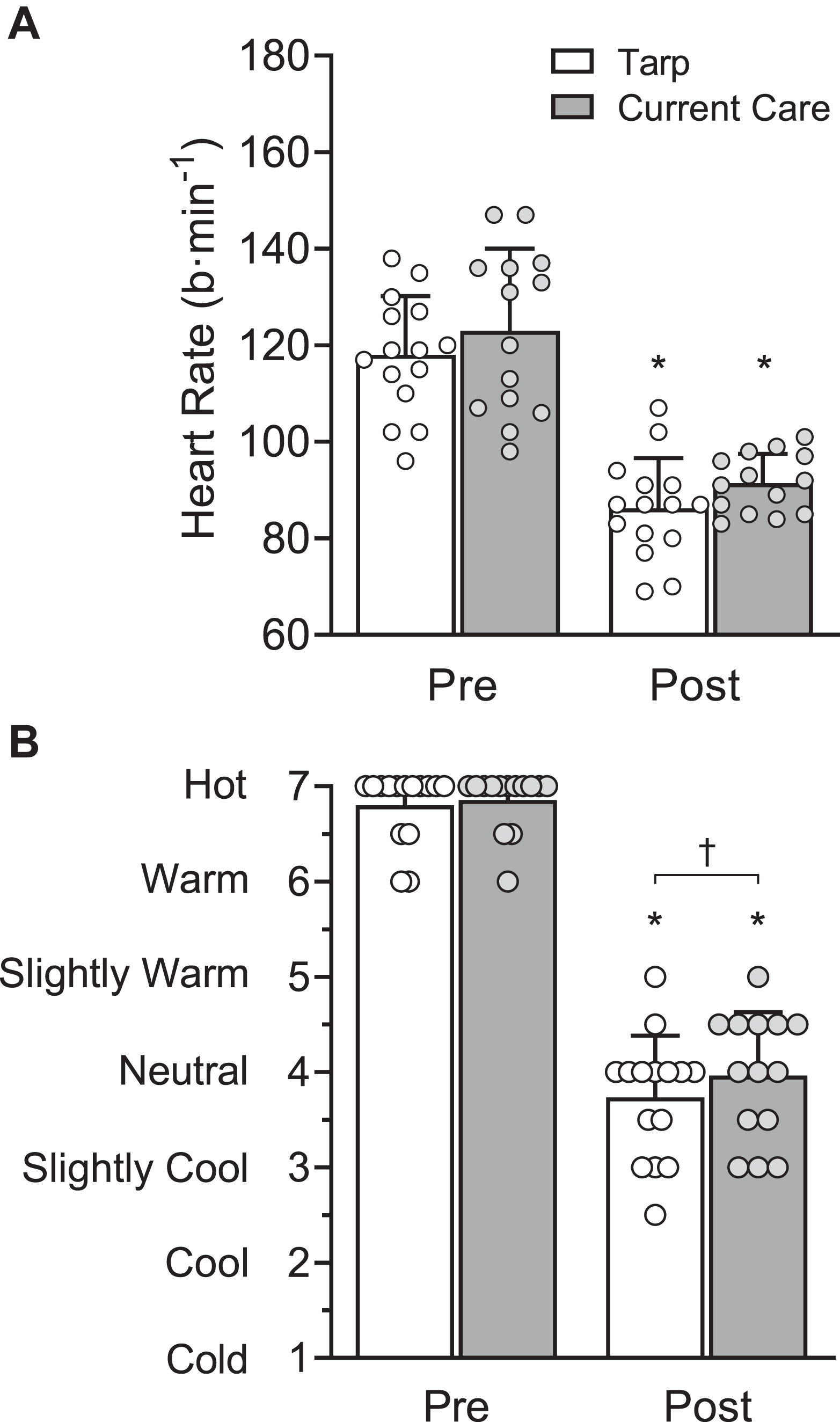
A, Heart rate before (Pre) and after (Post) cooling. B, Thermal sensation Pre and Post cooling. Tarp, tarp-assisted cooling. ∗P≤0.05 compared to Pre. †P≤0.05 between groups.
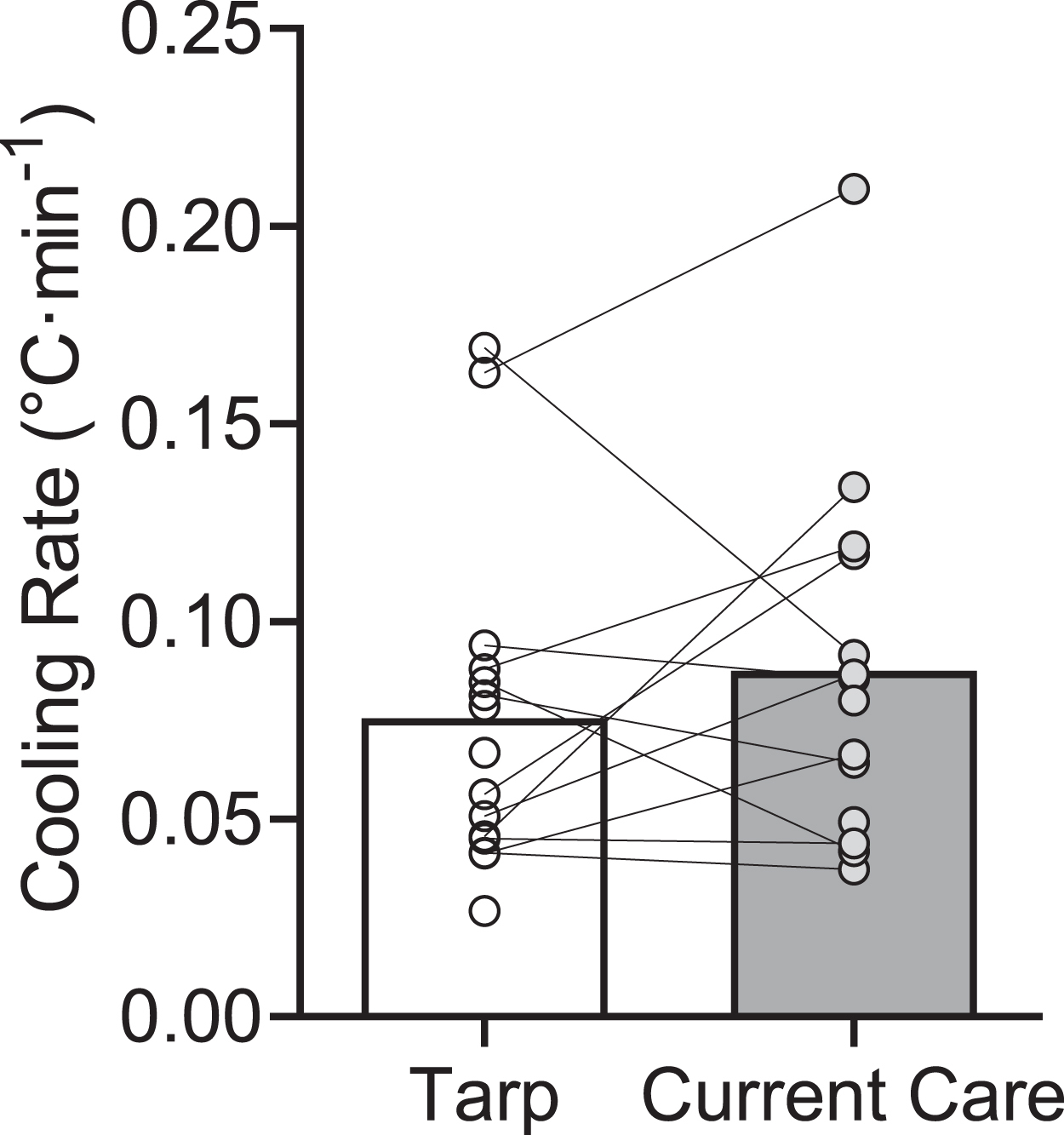
Cooling rate using tarp-assisted cooling (Tarp) or Current Care.
When Tc cooling rate was analyzed using 2-min epochs, cooling patterns were different between Tarp and Current Care (P=0.05). Epoch cooling rates were similar between Tarp and Current Care at all time points (all P>0.05). Within Tarp, Tc cooling rate was greater (all P<0.05) during min 2 to 12 compared to min 0 to 2 of cooling (0.044±0.037°C·min−1), with a maximum of 0.120±0.067°C·min−1 from min 6 to 8 (Figure 4). Within Current Care, Tc cooling rate was greater (all P<0.05) during min 2 to 6 compared to min 0 to 2 of cooling (0.063±0.070°C·min−1), with a maximum of 0.123±0.067°C·min−1 from min 2 to 4. In females, the epoch cooling rate from min 0 to 2 trended greater and had a larger ES in Tarp (0.078±0.044°C·min−1) compared to that in Current Care (0.033±0.026°C·min−1; P=0.06; ES=0.95).
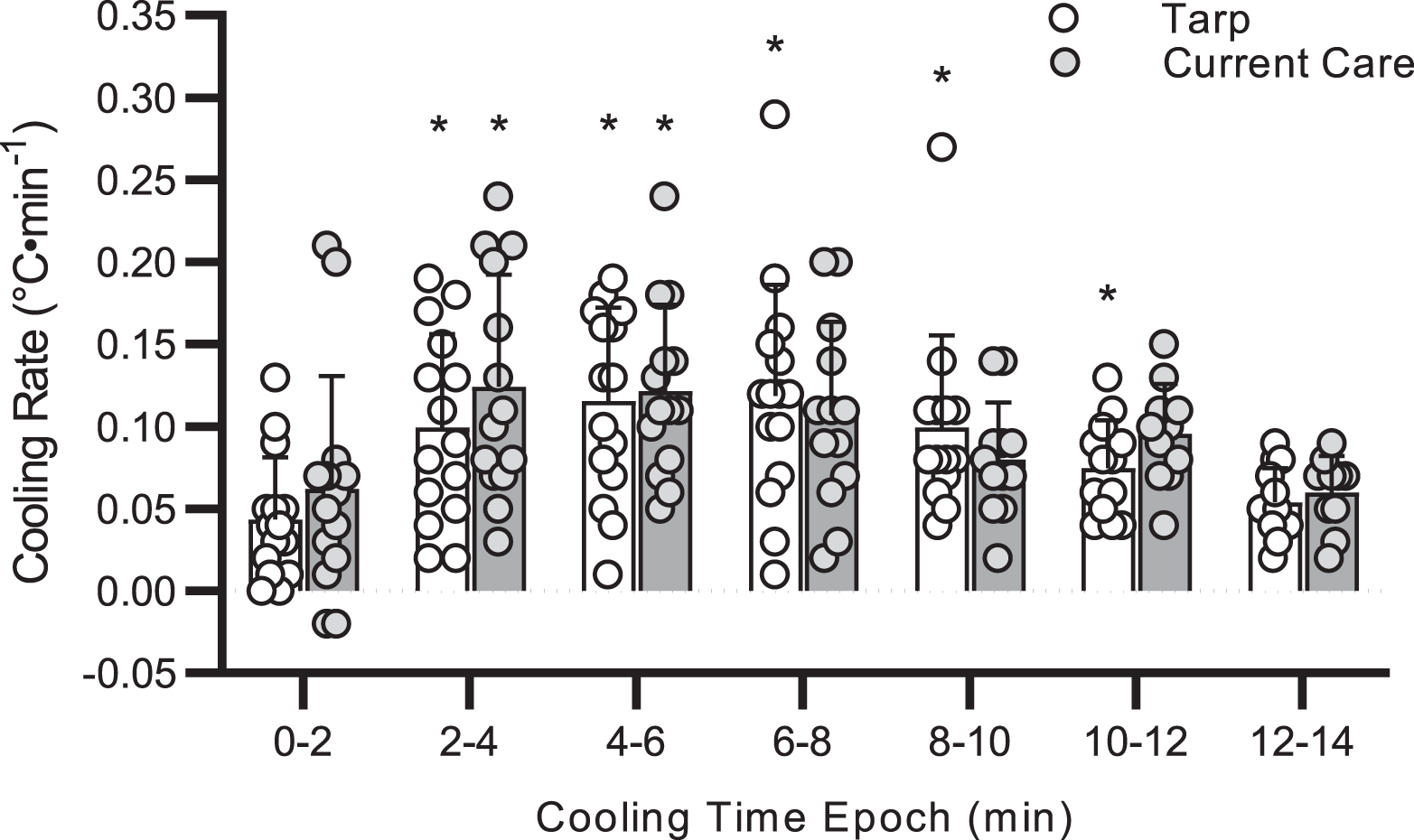
Cooling rate across 2-min epochs using tarp-assisted cooling (Tarp) or Current Care. ∗P≤0.05 compared to 0 to 2 min.
Body mass (Tarp, r=−0.12, P=0.68; Current Care, r=0.29, P=0.32), body surface area (Tarp, r=−0.07, P=0.80; Current Care, r=0.33, P=0.25), body surface area–to–mass ratio (Tarp, r=−0.02, P=0.96; Current Care, r=−0.30, P=0.30), and body mass index (Tarp, r=−0.01, P=0.98; Current Care, r=0.21, P=0.47) were not correlated to cooling rate in either Tarp or Current Care (Figure 5). In females, the relationship between body surface area and cooling rate during Current Care trended toward significance (r=0.80; P=0.06), indicating greater cooling rates with greater body surface area. No other relationships within sex were found to be significant (all P>0.05).
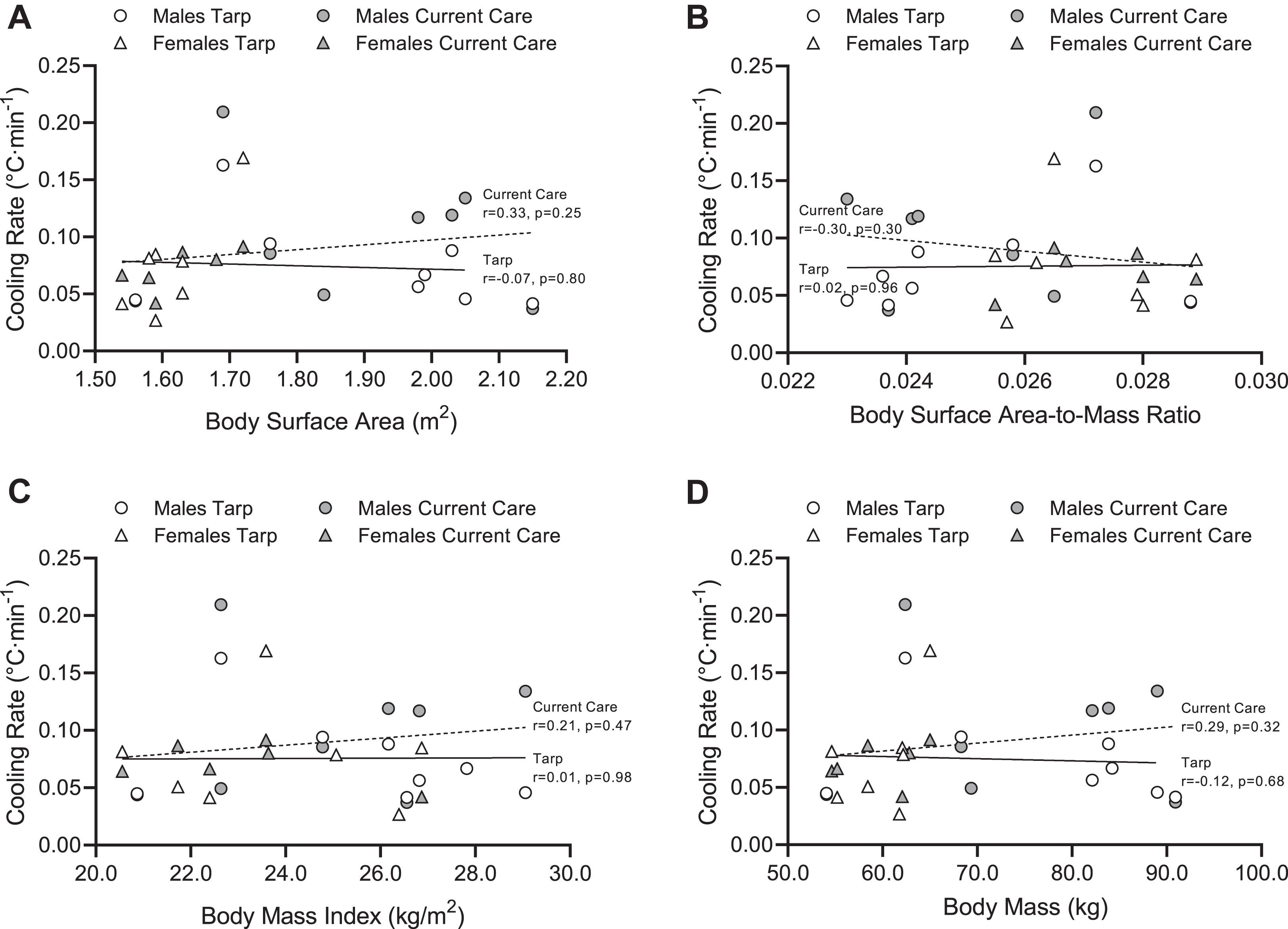
Relationships among cooling rates and physical characteristics: A, body surface area; B, body surface area–to–mass ratio; C, body mass index; and D, body mass. Tarp, tarp-assisted cooling.
Discussion
Cold water immersion is the gold standard for treatment of an EHS patient 21 ; however, this treatment is not always feasible in wilderness settings due to a lack of natural resources. The purpose of this study was to compare Tc cooling rates of tarp-assisted cooling using the limited resources available to a wildland firefighter and the current standard care provided in wilderness settings. To our knowledge, this was the first study to compare these cooling modalities, which determined no difference in cooling rates. When cold water immersion is not available in a wilderness setting, care provided to an EHS patient should continue to be dousing the patient with any available water and hiking them out to advanced medical personnel who can continue cooling with the most effective cooling modality available.
An EHS patient should be cooled to a body temperature of less than 40°C within 30 min of collapse or diagnosis of EHS to ensure survival and positive patient outcomes.22,23 This has been confirmed in a field setting with 274 EHS patients at a warm weather road race experiencing 100% survival and 93% of patients cleared for home discharge when whole-body cold water immersion reduced Tc to 38.8°C following EHS diagnosis. 10 Based on this concept and the plausibility of EHS patients having a Tc of up to 43°C at the onset of care, modalities with fast cooling rates are necessary considering the onset of cooling can be delayed after collapse.21,23 Along this line of thought, neither Tarp, with the limited resources available in the wilderness (0.076°C·min−1), nor Current Care (0.088°C·min−1) achieved an adequate cooling rate for EHS patient care. In the absence of a natural body of water to use as a field-relevant cold water immersion modality, EHS patients should be treated with the current standard care of dousing the person with water followed by hiking them out to the nearest road so as to not delay potential cooling opportunities provided by advanced medical care. 9 Perhaps an alternative is to hike the patient to a cleared field if a helicopter is available for transport in a timely manner. In a small case series, Poulton and Walker 24 found that 3 EHS patients had a cooling rate of 0.10°C·min−1 when placed under spinning helicopter rotary blades, allowing for another potential cooling option in the wilderness. Nevertheless, in this unique remote situation and depending on lack of availability of cooling resources, it may be prudent to disregard the mantra “cool first, transport second” and to prioritize transport. However, if colder and/or a larger volume of water is available, cooling before transport is likely the best option.
Tarp-assisted cooling has previously been successful in rapidly cooling hyperthermic individuals. Using large volumes (76–151 L) of cold water (2–9°C) results in cooling rates of 0.14 to 0.17°C·min−1,12,13 indicating its use for EHS patients. 11 Luhring et al 13 implemented tarp-assisted cooling with a large amount (151 L) of very cold water (2°C) to achieve a cooling rate of 0.14°C·min−1. Participants were partially immersed to the iliac crest, leaving the torso and arms exposed to air. To compare a smaller volume and warmer water, Hosokawa et al 12 demonstrated that tarp-assisted cooling utilizing 114 L of 9°C water requires 10 min to cool a hyperthermic individual, compared to 43 min of passive cooling, achieving an adequate cooling rate of 0.17°C·min−1. These participants lay supine in the tarp, fully covering their torso and legs, to achieve a greater cooling rate than that in the Luhring et al 13 study despite the warmer and smaller volume of water. 12 Implementing tarp-assisted cooling with resources available in a military setting (80 L of temperate water [27°C]) helped achieve a cooling rate of 0.12°C·min−1, a faster rate than that achieved with whole-body fanning while either wearing or not wearing a wet T-shirt. 14 The present study took this idea a step further by implementing similarly temperate water but of a smaller volume (11 L) to test a wilderness-relevant scenario. While the water remained close to the participants’ body, a cooling rate of only 0.076°C·min−1 was achieved. Future studies should determine the minimum volume of temperate water needed to create faster cooling rates for EHS patients considering that water available in the wilderness will likely be neutral in temperature if a natural source of cold water is not immediately available.
As indicated in Figure 3, there was a wide range of cooling rates among participants for both Tarp and Current Care, with 50% of participants having a faster cooling rate in Tarp than in Current Care. Although the present study was underpowered to directly compare males and females, males trended toward a greater cooling rate with Current Care while females had a slightly faster cooling rate with Tarp, although not significant. Others exploring sex differences and cooling of hyperthermic individuals have reported greater cooling rates in females completing cold water immersion compared to males when either matched for body surface area–to–mass ratio 25 or not matched based on physical characteristics. 26 Interestingly, the current study did not reveal meaningful relationships between physical characteristics and cooling rate with Tarp or Current Care when assessing all participants together. However, when separately looking at males and females, females had a strong relationship (r=0.80) between body surface area and cooling rate in Current Care. Greater body surface area allows for enhanced convective cooling as air moves across wet skin and heat transfer takes place from the individual to the environment, such as wind moving across the body while the patient is hiked to advanced medical care. Interestingly, body surface area was not related to cooling rate in males despite a wide range of this measure among participants. Additionally, there was not a strong relationship between body surface area and Tarp cooling rate (r=−0.07, P=0.80), likely due to the small volume of water in the tarp not allowing for full coverage over the body. Instead, most individuals rested in water that covered approximately the posterior half of the torso, not allowing for a larger body surface area to enhance cooling.
Unique challenges of wildland firefighting include prolonged exposure to extreme heat with potentially limited availability of shade opportunities, inclusion of heavy intensity work, limited access to potable water, wearing protective gear while carrying equipment, and a remote setting should an emergency occur. 1 -3,16,27 While heat illnesses in this profession are not widespread, they do occur and can be life-threatening,3,28 supporting the need to continue to evaluate the efficacy of prevention and intervention strategies. 29 Wildland firefighters should be educated on appropriate cooling techniques to be implemented in wilderness settings should someone experience EHS, including seeking a natural body of water to be used for immersion. 30 Administrations should ensure that a heat illness emergency action plan is in place and rehearsed annually to encourage rapid assessment and treatment of heat illnesses in the field. 8
Future studies on this research topic are warranted despite not measuring differences in cooling rate between Tarp and Current Care. The present study tested the use of Tarp with 11 L of 25°C water. Implementation of this method using slightly larger water volumes or slightly colder water temperatures represent less severe resource restrictions in the wilderness but could be applicable to other wilderness scenarios of larger groups of individuals with a larger volume of available water, potentially revealing a more effective field cooling strategy than currently implemented. There are many additional knowledge gaps regarding EHS treatment best practices warranting future study, including the optimum body cooling endpoint, factors influencing cooling rate, and the necessary time frame during which a person should be cooled to optimize patient outcomes. 31
Limitations
There are multiple limitations to the results of this study. First, for ethical reasons, participants did not reach a Tc >40°C, allowing the study of hyperthermic individuals but not EHS patients. Previous research has shown similar cooling rates between hyperthermic research participants and EHS patients when cold water immersion is implemented. 11 Still, it remains possible that EHS patients could experience greater cooling rates than those measured in this study with Tarp due to a greater thermal gradient between skin temperature and water temperature. 32 However, this larger gradient would also hold true while water is poured on the patient during Current Care, potentially increasing cooling rate in both groups. Second, due to physical constraints, participants exercised in a hot room but cooled in a warm room, which likely would not happen in a patient scenario in which cooling would occur in the hot setting. While this could affect absolute cooling rates, the impact would likely be similar for both Tarp and Current Care, allowing for direct comparison. Third, our participants were relatively homogenous regarding demographics, including young, healthy, fit individuals. Future research should sample from a more diverse population to determine if Tarp with limited resources is beneficial to any subpopulation of individuals in a field setting. Lastly, our Current Care results indicate trends toward significance for relationships between cooling rate and body surface area in females. This study was underpowered to determine differences between sexes. Perhaps greater heterogeneity of participants with a wide range of physical characteristics would show more conclusive results regarding subpopulations. 33
Conclusions
Cold water immersion remains the gold standard for treatment of EHS. 21 The purpose of this study was to compare the cooling rate of hyperthermic individuals using Tarp with the limited resources available in the wilderness setting with the current standard care provided in this setting, assuming the absence of cold water immersion availability. The current study does not support the use of Tarp for body cooling of hyperthermic individuals when implemented with the limited resources available to wildland firefighters due to the slow cooling rate (0.076°C·min−1). When cold water immersion is unavailable, patients should be cooled using the current standard care provided in a wilderness setting of dousing the patient with any available water and hiking them out to advanced medical care.
Footnotes
Acknowledgements
Acknowledgments: The authors thank Jackie Schwob for her technical assistance; Keiona Nance for her dedication; and the Hydration, Exercise, and Thermoregulation Lab students for their data collection efforts.
Author Contributions: study concept and design (RRP, KH); data acquisition (RRP, KH, TF, JJS); data analysis (RRP); drafting and critical revision of the manuscript (RRP, KH, TF, JJS); and approval of final manuscript (RRP, KH, TF, JJS).
Financial/Material Support: The project was funded by the 2019 Wilderness Medical Society Peter Hackett–Paul Auerbach grant, supported by the Academy of Wilderness Medicine®.
Disclosures: None.
Presented at the Wilderness Medical Society Summer Conference, August 3, 2022, Snowmass Village, CO.