
Abstract
Introduction
The dermatological effects of box jellyfish envenomation among stinging victims in Thailand are not well reported, particularly concerning chronic effects. For first aid, different recommendations indicate the necessity for the removal of tentacles in life-threatening situations. This study aimed to describe the dermatological effects of box jellyfish envenomation and propose recommendations regarding first aid for victims in urgent care or life-threatening situations.
Methods
Surveillance systems and Toxic Jellyfish Networks were established to improve detection and investigation. The networks investigated all severe victims of jellyfish envenomation. A retrospective study was conducted, and victims of stinging by box jellyfish investigated from 1999 to 2021 were included.
Results
One hundred and twenty-four victims were recorded. The majority of victims were males (55%), tourists (69%), and Thai nationals (49%). Direct contact had more severe consequences than indirect contact. Dermatological effects included edema, erythematous caterpillar track–like rash, blistering, bullae, papular eruption, necrosis, digital gangrene, recurrent dermatitis, dermal hypersensitivity, numbness, lichenification, hyperpigmentation, keloids, and scarring. Suffering and healing continued from several weeks to many years. Victims with multiple-tentacle box jellyfish stings had papular eruptions and greater severity of skin issues. All fatally envenomed victims collapsed within a few minutes and received incorrect/no first aid. The proposed first aid for life-threatening box jellyfish stings is continuous irrigation of the wound with vinegar for at least 30 s and initiation of cardiopulmonary resuscitation if there is no respiration or heartbeat. Tentacles often detach spontaneously, and removal is not always necessary, thus saving time.
Conclusions
The findings provide input for improving diagnosis and treatment guidelines.
Introduction
Fatal box jellyfish stings were initially denied by the general population and experts in Thailand. Two medical epidemiologists from the Ministry of Public Health and Faculty of Medicine, Chiang Mai University (author), started to investigate the issue and have amassed evidence to verify the existence of lethal box jellyfish envenomation in Thailand.1,2 The most severe envenomation occurrences in Thailand have been caused in the majority of victims by multiple-tentacle and single-tentacle box jellyfish (Class Cubozoa). The multiple-tentacle box jellyfish, Chironex spp, has caused many fatal and near-fatal incidences. 3 -8 Single-tentacle box jellyfish stings are known to cause Irukandji syndrome and Irukandji-like syndrome. Small carybdeid jellyfish, specifically Carukia barnesi, are considered to be the main cause of Irukandji syndrome. 9 Other Australian carybdeid jellyfish are Morbakka spp and Morbakka fenneri.10,11 In Thailand, different species of single-tentacle box jellyfish may cause Irukandji-like syndrome with different clinical manifestations. 11 -14 Jellyfish stings frequently cause immediate local skin reactions; however, although rare, envenomation can cause a delayed allergic reaction. 6 -8,13,15-17 A case of recurrent dermatitis was reported as lasting over a year after stings had been reported. 15 Other local pathologies that were reported after victims were in jellyfish contact lasted for a few minutes to several weeks and included linear plates, vesicles, papular vesicles, blebs, blisters, widespread papulonodular eruption, pruriginous rash, recurrent dermatitis, dermal hypersensitivity, urticaria, gangrene, and vasospasm. 5 -8,13-20 Chronic dermal manifestations included localized fat atrophy, hyperhidrosis, hyperpigmentation, lichenification, lymphadenopathy, contracture, keloid, and scarring.4,6-8,13,18,21,22 Few victims of recurrent eruptions and delayed eruptions have been reported.16,17 Inappropriate treatment and wound care may lead to complications.6,8,14,18 Of concern is that in Thailand, the official medical school curriculum does not cover deadly box jellyfish envenomation in detail. Physicians and health professionals might not know or be unaware of delayed or recurrent dermal reactions and have not detected skin reactions in the past or have misdiagnosed or underreported the conditions. The latest clinical practice guidelines available in 2020 do not cover all aspects of wound care. 23 The dermatopathology of box jellyfish envenomation and particularly chronic effects are not well reported or clearly differentiated from those caused by other marine stings in Thailand. Part of the explanation for this is the difficulty in collecting data due to the severity of victims attending the emergency room and, until relatively recently, the unavailability of cameras in Thailand. There is also a controversy among both the general public and the medical community regarding the use of food grade vinegar (4–6% acetic acid) as a first aid treatment for these stings. Furthermore, there are different recommendations concerning the necessity for the removal of tentacles in life-threatening situations.22,24,25
Dr Siriarerayaporn from the Ministry of Public Health and Professor Dr Thaikruea from the Faculty of Medicine of Chiang Mai University initiated this investigation. They have established clear evidence that the deadly box jellyfish exists in Thailand.1,2,5,7,8,13,14 They formed a professional team and established Toxic Jellyfish Networks in 2008. These networks include a task force and expert and community groups.1,2 The surveillance of toxic jellyfish was established to detect victims, develop knowledge about jellyfish envenomation, implement prevention and control measures, and establish effective treatment guidelines. The Toxic Jellyfish Networks have detected many victims of jellyfish envenomation, and all severely injured victims detected by the networks were investigated prospectively and retrospectively.1,2,5-8,14,26-28
This study aimed to describe the dermatological effects of box jellyfish envenomation and the impact of medical interventions in victims in Thailand. Recommendations regarding first aid in urgent victims are also proposed. This study provides evidence and useful information for the improvement of both practical diagnosis and clinical practice guidelines. 23
Methods
This retrospective study was conducted by reviewing all cases of presumed box jellyfish stings from 1999 to 2021. Data collected included age, gender, occupation, nationality, details of the incident, description of clinical manifestation, treatment outcome, and photographs of the affected areas. Only photographs with available verified consent forms are shown in this study.
Data Analysis
Descriptive analysis included median (range), mean (standard deviation), and proportion (percentage) depending on data distribution.
Ethics Approval
The review and approval by the research ethics committee of the Faculty of Medicine, Chiang Mai University, were waived for this study due to the secondary nature of the data (no. exemption 8072/2021 of study code: COM-2564-08072 / research ID: 8072).
Results
Single-tentacle box jellyfish means 1 tentacle extending from a pedalia attached to each corner of the bell. Multiple-tentacle box jellyfish means many tentacles extending from a pedalia attached to each corner of the bell.
The criteria for identifying the envenomation as caused by box jellyfish in this study were as follows: Multiple-tentacle box jellyfish stings
Individuals who had a history of exposure to jellyfish and developed the following: Any one of the following signs: tentacle mark, necrosis, local soft-tissue edema, blister, swelling of affected organs/areas, digital gangrene, near-collapsed, and collapsed. Any one of the following symptoms: respiratory distress, chest pain, pain at the wound, burning pain at the wound, and itching/irritation at the wound.
Multiple-tentacle box jellyfish found in Thailand included Chironex indrasaksajiae Sucharitakul, Chironex sp A, and Chironex sp C.3,12,27-29 Single-tentacle box jellyfish
Individuals who had a history of exposure to jellyfish and developed the following: Any one of the following signs: tentacle mark, necrosis, local soft-tissue edema, blister, swelling of affected organs/areas, abnormal heartbeat, abnormal blood pressure, digital gangrene, near-collapsed, and collapsed. Episodes of any one of the following symptoms: itching/irritating at the wound, wound pain, burning pain at the wound, abdominal pain, back pain, leg pain, muscle pain, chest pain, body ache, heartache, pain at other parts of the body, respiratory distress, chest tightness, nausea, vomiting, cramping of abdomen or limb, fatigue, tremor, sweat, agitation, anxiety, and restlessness.
Single-tentacle box jellyfish found in Thailand included Morbakka sp A, Morbakka sp B, Morbakka sp C, and Carukiidae sp (indescribable because it was examined and was a previously undescribed species).12,14,27,28,30
Demographic Data And First Aid Of Box Jellyfish Envenomation Victims
Envenomation in 124 victims was reported as being caused by box jellyfish stings from 1999 to 2021. The median age was 25 y (range, 2–68 y). The majority of victims were males (55%), tourists (69%), and Thai nationals (49%) (Table 1). The victims who received appropriate or late appropriate first aid totaled 46% and those receiving inappropriate first aid 38% (Table 1). Of 9 fatal victims, 5 received incorrect first aid, and 4 did not receive first aid. Eight fatal victims collapsed at the scene after between 1 and 5 min, and in 1 case, the exact time could not be determined but was between 1 and 10 min.1,4,8
Demographic data of box jellyfish envenomation victims
First aid: appropriate is defined as continuous pouring of vinegar over the wounds for 30 s and performed within 5 min of the incident without other chemical or physical application; late appropriate is defined as appropriate but took place more than 5 min after sting; and inappropriate is defined as physical or chemical application with/without vinegar pouring.
Characteristics Of The Dermatological Effect Of Box Jellyfish Envenomation
Twenty-nine and 92 victims were stung by single-tentacle and multiple-tentacle box jellyfish, respectively. For another 3 victims, there were limited data for determining whether the stings were from single- or multiple-tentacle box jellyfish.
Direct Contact Effect
For analysis of the effect on the skin, 4 victims with multiple-tentacle box jellyfish stings were excluded. Almost all victims had tentacle marks that appeared like the caterpillar tracks of a tank (caterpillar track–like) (90–100%) (Table 2). For the victims who had been given appropriate first aid (vinegar immediately poured over the wound for 30 s), tentacle marks were reported to be white or pale before turning to red (Figure 1A and B). The erythematous rash usually appeared after stings (Figure 1C). The color of the tentacle marks turned to dark brown within 1 to 2 d after stinging (Figure 1D). Around the seventh day, the wounds developed black scabs (Figure 1E).
The dermatological effect on skin after the acute stage
For analysis of the effect on skin after the acute stage, 4 victims who had eaten multiple-tentacle box jellyfish were excluded. Nine fatal victims were excluded from blister and papulonodular eruption analyses due to there being no reaction after death. Additional victims with a follow-up time of less than 3 d were excluded from analysis of papulonodular eruption.
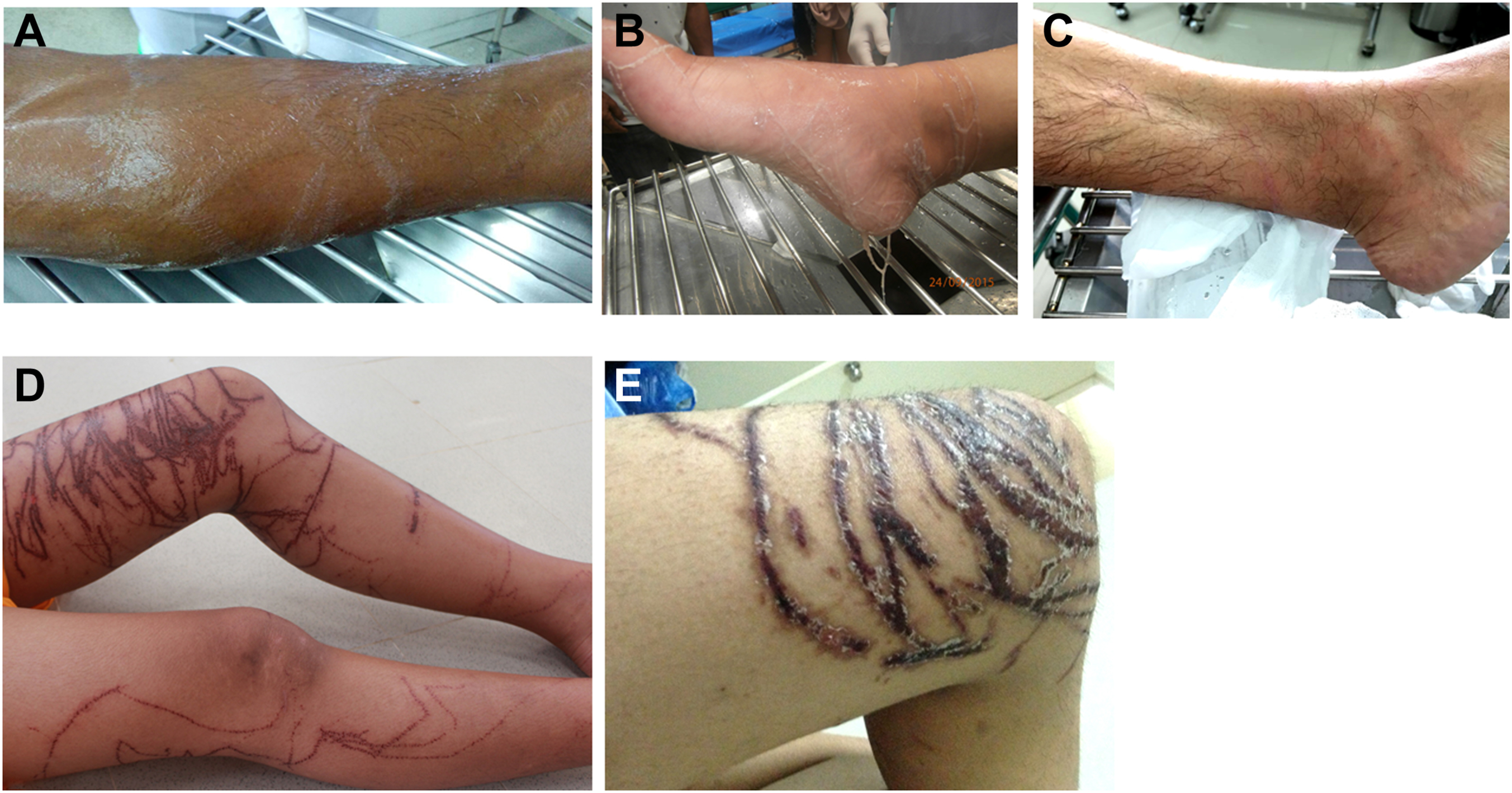
Direct contact effect of box jellyfish envenomation on skin. A, Single-tentacle box jellyfish: white tentacle marks appeared like caterpillar tracks. B, Multiple-tentacle box jellyfish: pale tentacle marks appeared. Tentacles fall off after appropriate vinegar pouring treatment. C, Multiple-tentacle box jellyfish: erythematous rashes appeared. D, Multiple-tentacle box jellyfish: dark brown rashes appeared like caterpillar track of the tank. E, Multiple-tentacle box jellyfish: wounds developed black scabs.
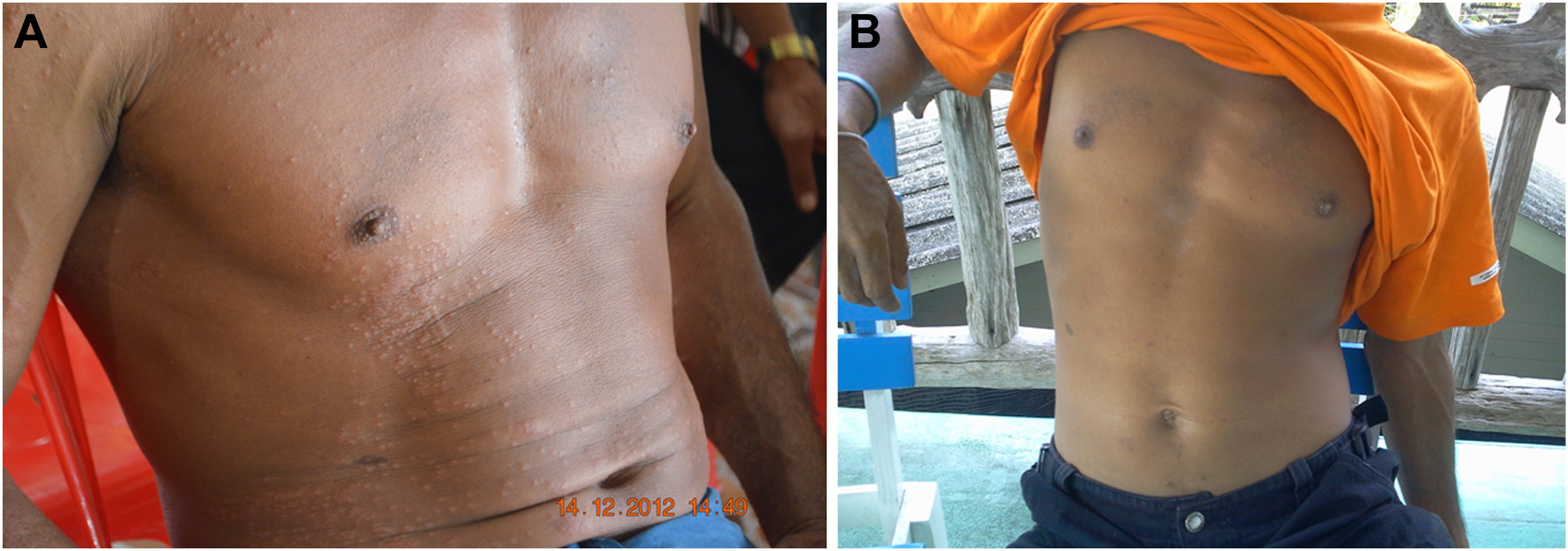
Around the third to the sixth day, papular eruptions with mild to severe itching developed in a few victims (Figure 2A). One victim had recurrent papulonodular eruptions 1 to 3 times a year for 4 consecutive years. The frequency of papulonodular eruption and severity of itchiness decreased over time (Figure 2B).
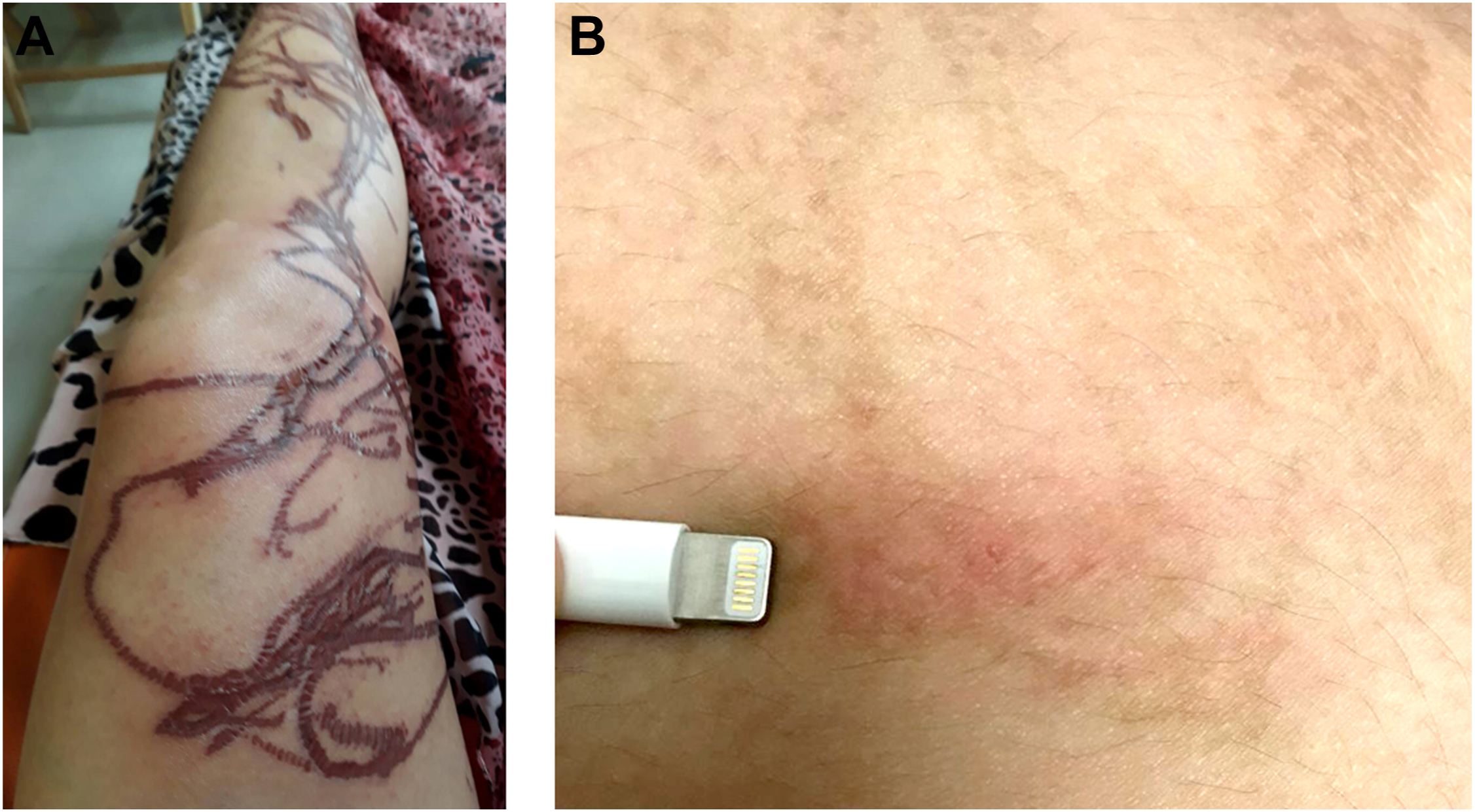
Papular eruption and recurrent papular eruption among victims stung by a multiple-tentacle box jellyfish. A, Papular eruption. B, Recurrent papulonodular eruption.
In the cases with a history of inappropriate first aid, the tentacle marks had blurred rims with vesicles at the rims (Figure 3A) or large bullae (Figure 3B). Blisters or bullae also developed on the first day among the victims in whom there had been extensive contact with tentacles (Figure 3C).
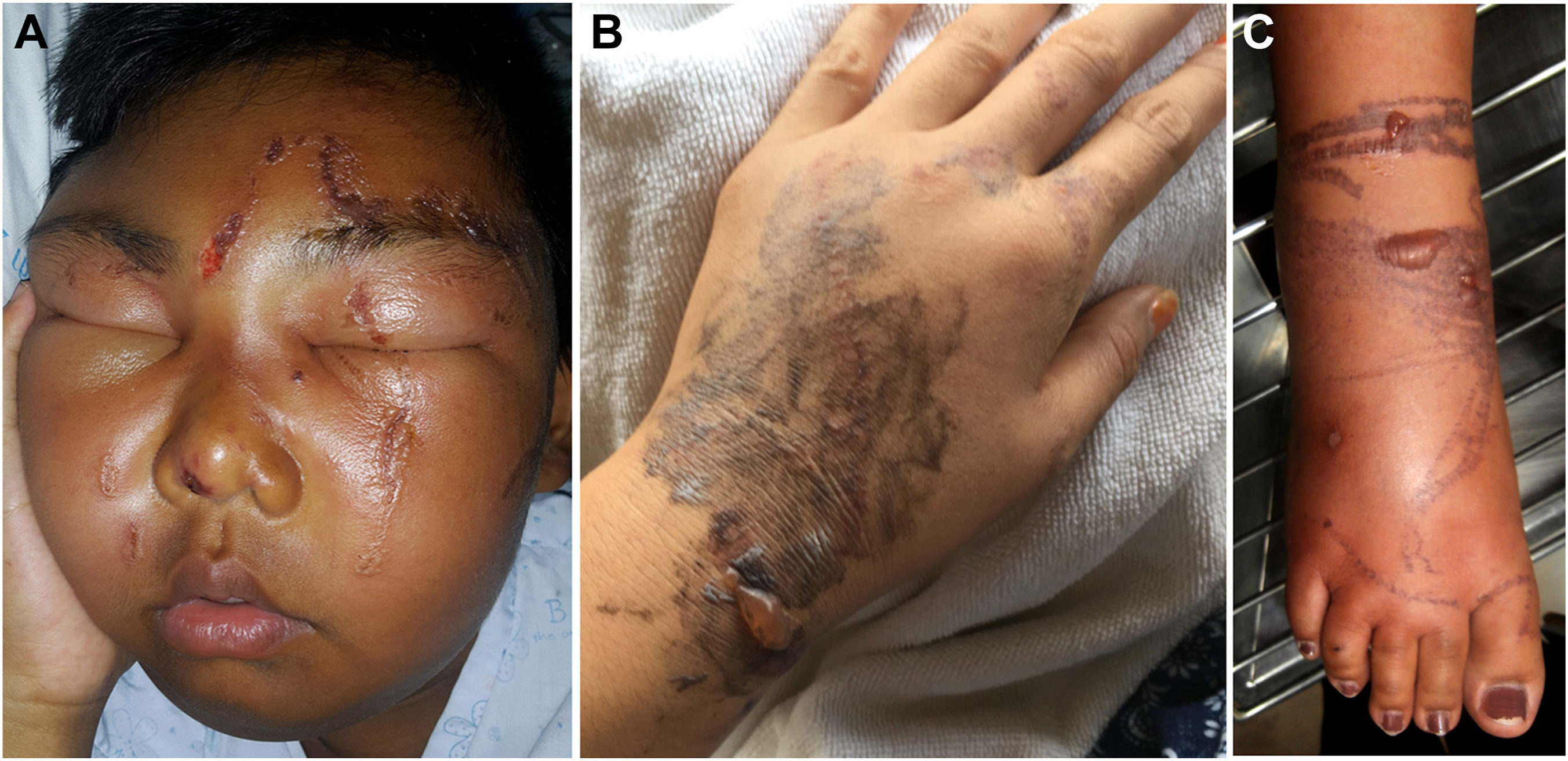
Development of vesicle, blisters, and bullae among victims stung by box jellyfish. A, Victim rubbed soap and fresh water on his face after stings. The wounds had blurred rims and blisters on the rims. B, Victim was rubbed with sand after stings. The wounds had small blisters and large bullae. C, Moderate to large bullae on the dense tentacle marks.
For those who had gangrene, skin started to decompose in the middle of the wounds around the second week. The skin turned black (Figure 4A). In the victims in whom there was wound infection, yellowish liquid appeared at the rims with erythematous skin (Figure 4A). One victim developed digital gangrene around the fifth day (Figure 4B).
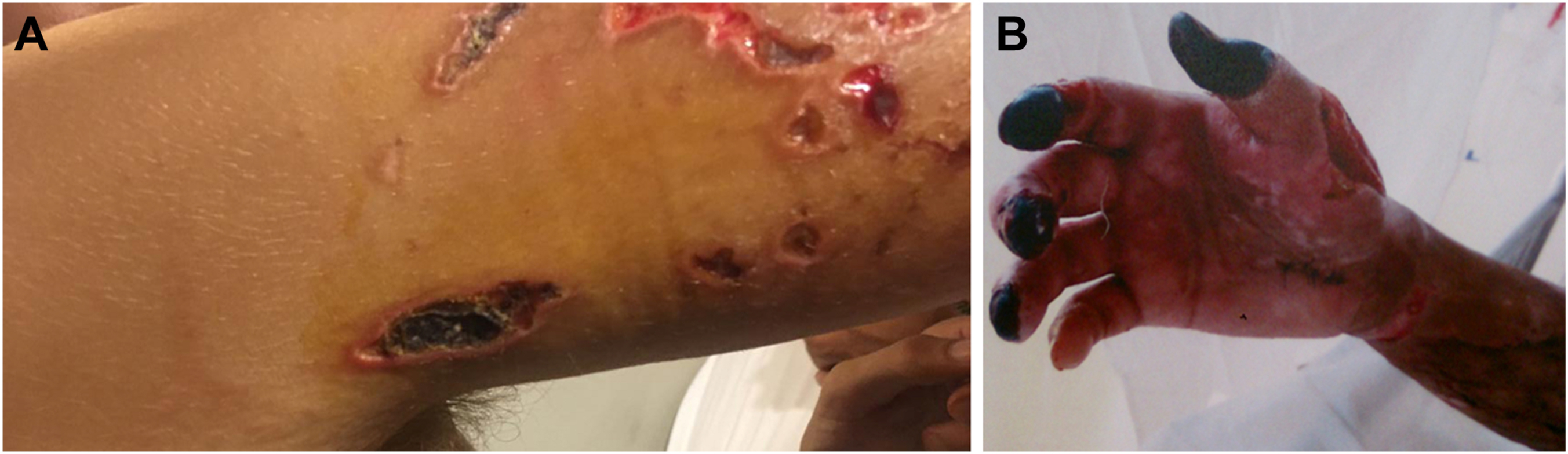
Gangrene and infection occurrence among victims stung by box jellyfish. A, Skin turned black and gangrenous, and some wounds were infected. B, Victim had digital gangrene.
One victim stung by single-tentacle box jellyfish had sweat on the affected hand 18 h after the stinging incident (Figure 5).

Victim stung by single-tentacle box jellyfish had sweat on the affected hand.
For victims without infection or gangrene and who had appropriate first aid and timely treatment, the wound usually left no scarring and no keloid. In this group, hyperpigmentation of the tentacle marks faded over time and disappeared in a few years (Figure 6A and B). Victims with histories of inappropriate first aid or inappropriate treatment had scarring, keloid, or suture marks (Figure 6C and D).
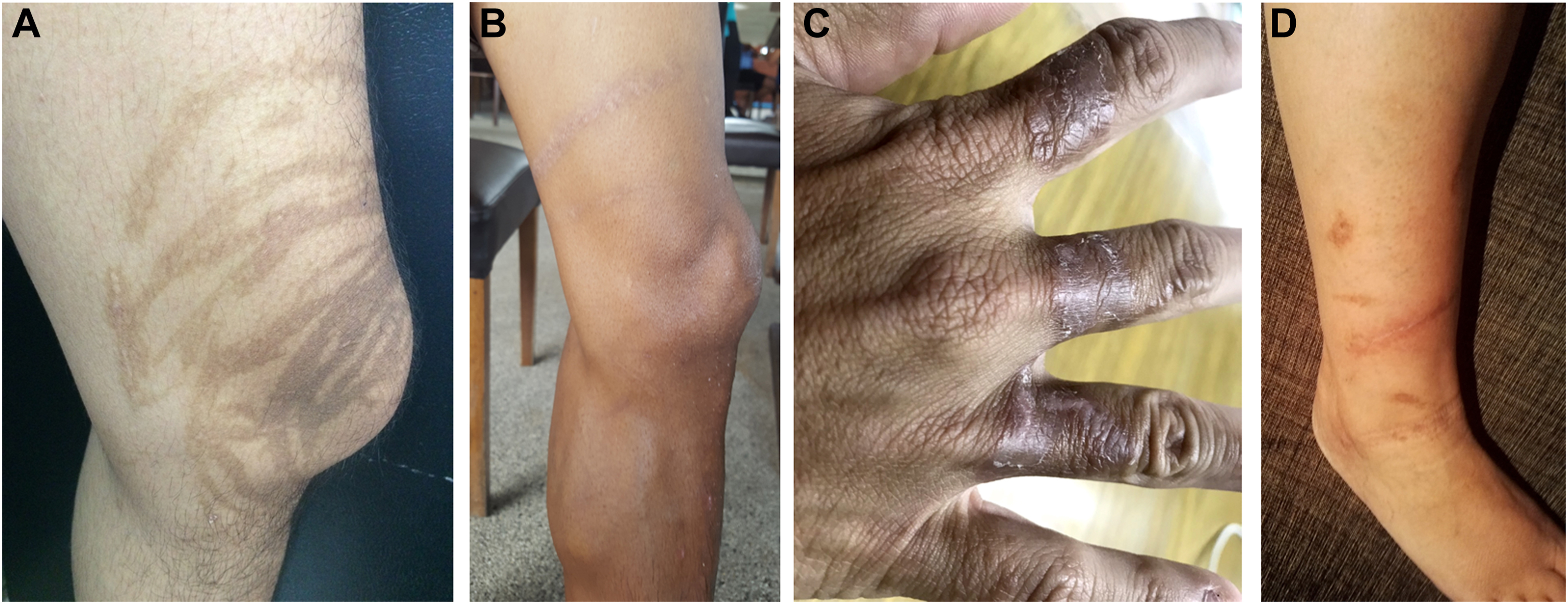
Characteristics of healing wounds among victims stung by box jellyfish. A, Hyperpigmentation remained 3 y after stinging by multiple-tentacle box jellyfish. B, Hyperpigmentation remained 1 y after stinging by single-tentacle box jellyfish. C, Victim with a history of rubbing tentacles off during pouring vinegar for less than 30 s had scarring. D, Victim with a history of flushing wounds with water had operation and suture marks.
Indirect Contact Effect
Indirect contact with box jellyfish tentacles happened when the individuals were exposed to box jellyfish tentacles that were attached to other objects, such as the skin of other victims during rescue attempts, wetsuits, leaves floating in the sea, or fishing nets, while catching fish. All of them had minor injuries, such as small erythematous rash, small erythematous nodules, and erythematous papules. Small erythematous papules appeared on the contact areas after stings (Figure 7A). There was no blistering, gangrenous skin, or appearance of caterpillar track–like rash. The wounds usually healed without scarring in the long term (Figure 7B).
Indirect contact effect of box jellyfish envenomation on skin. A, Small erythematous papules appeared on the contact areas after stings. B, No scarring left around 1 mo after sting.
One of 4 victims who ate boiled multiple-tentacle box jellyfish spicy salad had an erythematous soft palate and tongue after eating, with the injury turning brown on the next day. This victim also had an irritated throat, palpitations, and high blood pressure (Figure 8).

Victim who ate boiled multiple-tentacle box jellyfish spicy salad developed an erythematous soft palate.
Characteristics Of The Dermatological Effects Of Single- And Multiple-Tentacle Box Jellyfish Envenomation
All 3 victims who had limited data to determine whether stinging was by single- or multiple-tentacle box jellyfish had tentacle marks that looked like tank caterpillar tracks (Table 2). For analysis of the effects on the skin after the acute stage in the multiple-tentacle box jellyfish group, 4 victims who had eaten multiple-tentacle box jellyfish were excluded from the analysis of caterpillar track–like rash, and the additional 9 fatal victims were excluded from the blister and papular eruption analyses (due to no reaction after death). Twenty-nine and 83 victims stung by single- and multiple-tentacle box jellyfish, respectively, were subsequently followed up. The median duration of follow-up was 7 d (range, 2–2920 d). Blisters developed in around one-fifth of victims (Table 2).
The papular eruption occurred a few days later; thus, 46 victims who were followed up for at least 3 d were included in the analysis. No victim of papular eruption was reported among 12 victims stung by single-tentacle box jellyfish. However, 4 of 34 (12%) victims stung by multiple-tentacle box jellyfish presented with an eruption (Table 2).
One interesting case was a Finnish woman aged 48 y. The patient was a healthy nurse without any underlying disease. On January 22, 2016, a jellyfish approximately 30 to 40 cm in diameter touched her right thigh. The patient kicked it, but the jellyfish landed on the leg and ankle, and she flushed her leg with water from the shower at the beach. The contacted skin turned white and was surrounded by erythematous skin (Figure 9A). On the second day, the central part of each area turned dark brownish black, and on the fourth day, blisters developed (Figure 9B). From the 4th through the 19th day, the patient had severe itching around the wounds and slight swelling. On the 17th to 20th day, wound infection occurred with yellow liquid and the wounds became very red and itchy around the edges (Figure 9C). On the 31st day, there was a very hard white substance in the bottom of the lesions without any sensation of open wounds. On the 37th day, the affected skin on the thigh, leg, and ankle turned reddish. The patient had excruciating pain in the metatarsal area, had difficulty moving the toes, and could not extend her ankle. During the 38th to 42nd days, the patient underwent daily wound debridement using a curette under sedation. The patient reported severe pain in the wound site and hyperesthesia sensation in the affected leg. Approximately 2 mo after the stings, a proportion of the wounds had closed and the patient reported severe pain in the remaining open wounds (Figure 9D). Fifteen and a half mo after being stung, the patient needed suturing to close some open wounds (Figure 9E), and it took 22 mo for the majority of the wounds to close (Figure 9F). The patient had itchy and hard scars, which she described as “like the sole of a shoe.”
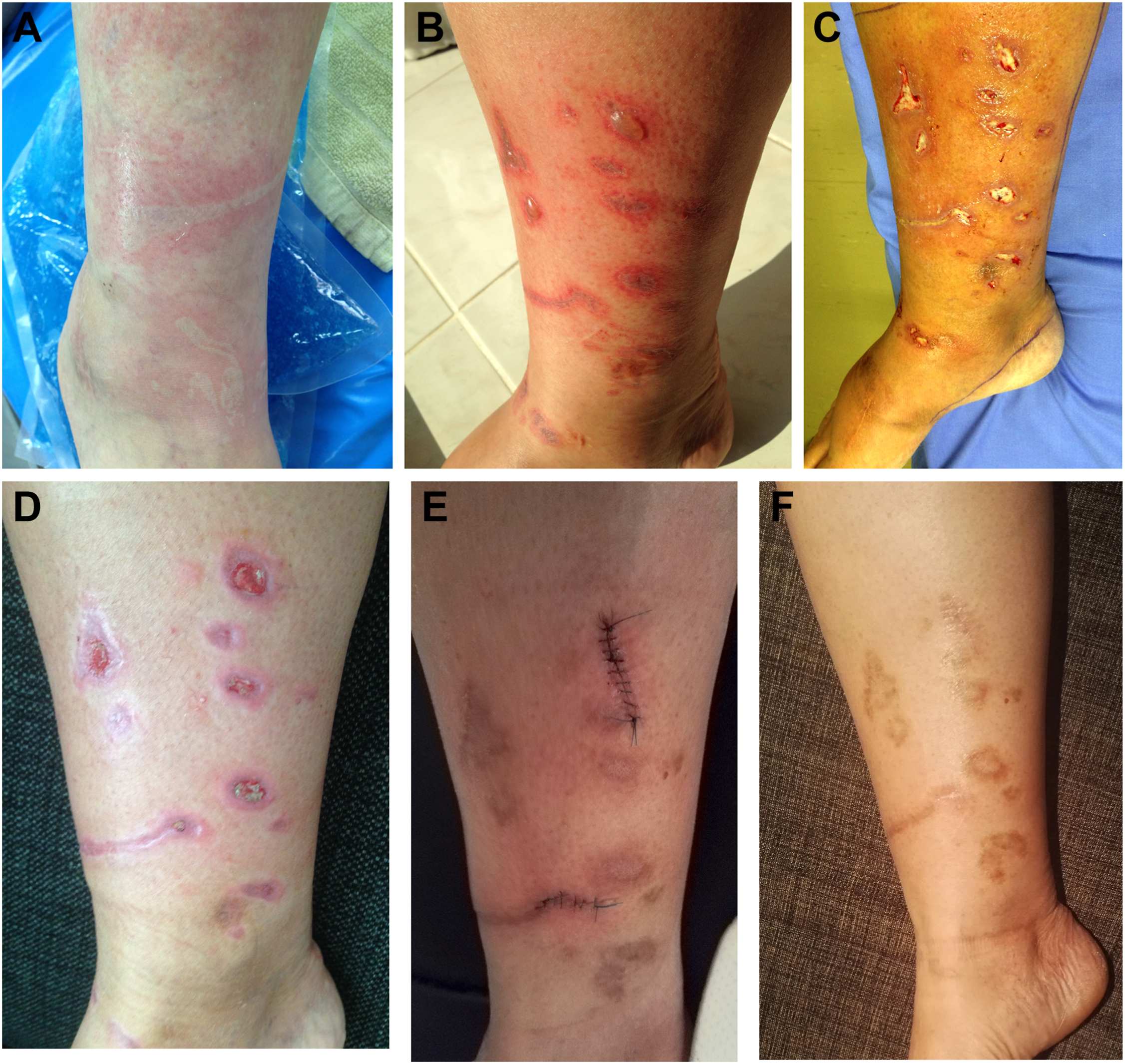
Chronic effect on the skin of a victim stung by a multiple-tentacle box jellyfish. A, Skin became white and surrounded by erythematous skin, with tentacle marks appearing as light brown tank caterpillar tracks. B, Blisters developed. C, Wounds became infected. D, Some of the wounds closed. E, Suturing needed to close some open wounds. F, The majority of the wounds closed.
Discussion
Identification of the jellyfish species and the toxins is difficult because of unavailability of routine tests for these stings, and, in many instances, the difficulty of collecting the species responsible for the envenoming. Giavedoni et al 16 reported jellyfish sting victims with cutaneous eruptions off the Carolina beach in the United States, and the suspected causative species was Physalia physalis. In Thailand, there is ongoing research into identifying the different species of box jellyfish, and at least 1 species of lethal multiple-tentacle box jellyfish has been reported, C indrasaksajiae Sucharitakul.3,29 There is a common belief in Thailand that foreigners are allergic to jellyfish and the illness is due to an allergic reaction, not the venom.1,13 This study found that almost half of the reported victims were Thai people. These victims had symptoms and wounds that support the existence of the effects of the toxins rather than allergic reactions.
Characteristics The Of Dermatological Effect
This study found that direct contact had more effects than indirect contact. It might be due to tentacle attachment. The more extensive the contact between the tentacles and the skin, the greater the firing of the nematocysts, increasing injury and leaving more marks. Indirect contact was more likely to result in scattered nematocysts from loose tentacles that had become detached from the body of the box jellyfish. The firing rate decreased after the jellyfish died. 31 Thus, there was no blistering, gangrenous skin, or appearance of caterpillar tracks among these victims, and the wounds usually healed without scarring in the long term. It is worthwhile noting that the pale or white color of tentacle marks on the skin is rarely seen among direct contact victims because the recording of such incidents needs both appropriate first aid and rapid photography. Papular eruptions developed in a few victims, while another study reported half of the victims having these. 32 It might be underreported in this study because only half of the victims had been followed up and approximately 41% had a follow-up period of at least 3 d, particularly tourists or foreigners. Blisters or large bullae developed around the fourth or fifth day among the victims with appropriate first aid but on the first day among the victims in whom contact was with more tightly grouped or dense tentacles. Dense contact with tentacles might result in the extensive firing of nematocysts, transferring more toxins to a relatively small area of skin. The victims who received inappropriate first aid also had blisters or large blebs on the first day. These physical and chemical exposures triggered greater nematocyst firing, which resulted in victims receiving more toxins.31,33,34
Other skin effects that were reported after contact with jellyfish from within few minutes to several weeks included vesicles, papular vesicles, bleb, blisters, widespread papulonodular eruption, pruriginous rash, recurrent dermatitis, dermal hypersensitivity, urticaria, gangrene, and vasospasms. 5 -8,13-20 This current study also found similar results. The effect of box jellyfish envenomation on oral mucosa has never been reported in Thailand. This victim (Figure 8) presented with an erythematous soft palate and tongue. This supports the idea that there are nematocysts located in other organs of the jellyfish. 35 This finding is useful for improving public education and risk communication.
For the victim with severe chronic effects on the skin, almost 2 y were required to complete the treatment to give a good outcome. This patient suffered a great deal. Chronic dermal manifestations, also reported by other studies, included localized fat atrophy, hyperhidrosis, hyperpigmentation, lichenification, lymphadenopathy, contracture, keloid, and scarring.4,6-8,13,14,18,21,22
First Aid In Urgent Victims
Immediate first aid is a crucial adjunct to the survival of injuries. A 4 to 6% concentration of vinegar is very effective in inactivating unfired nematocysts.18,22,23,34 This study found that approximately half of the victims received incorrect or no first aid. Incorrect first aid induced nematocyst firing, leading to more severe effects both on the skin and clinically, such as infection, necrosis, gangrene, keloid, and scarring.6,18,23,36,37 In urgent or life-threatening situations, a few critical steps are important for preventing death.8,18,23,34,37 Based on the author’s experiences, vinegar needs to be poured immediately and continuously over the whole wound for at least 30 s. Tentacles often detach spontaneously, and removal is not always necessary, thus saving time. 18 In addition to vinegar poles/stations on the beaches, cooking vinegar is available in convenience stores, restaurants, and resorts along the beach in Thailand and other countries with similar contexts. If victims with severe injuries receive the vinegar pouring technique after stinging within 15 min, they could survive. 18 Based on these findings and the author’s experience over a decade, the majority of the victims who received appropriate first aid and survived for at least 10 min at the scene had good recovery rates in the hospital. 5 -8,13,14,18
Medical Intervention
There are changes over time in knowledge, perception, and practice. The changes include the development of guidelines (prevention, first aid, and treatment) and, therefore, increased the scientific and applied knowledge necessary for dealing with box jellyfish stings. The educational materials cover jellyfish envenomation, clinical manifestations, diagnosis, nematocyst, first aid, treatments, clinical practice guideline, complications, surveillance, prevention, and control. Training courses also cover the same topics. Communities’ capacities have been increased. Practical innovations include a vinegar station, educational warning sign, vacuum sticky tape technique, stinger net, and stinger net sign. People have used vinegar instead of sea morning glory for first aid. Knowledge sharing and distribution are benefiting not only people in Thailand but also people from other countries.1,2,5,6,14,18,23,26,38
Limitations
The main limitations of this study were that some data were not available due to this being a retrospective study and the assigned cnidarians was presumed because identification was not formally established by qualified verification of the taxon responsible for the sting. However, only 3 victims had limited data about the class of box jellyfish. Data pertinent to the effects on the skin were complete. The advantage of this study was inclusion of the largest number of victims occurring during the past 2 decades in Thailand. What was reassuring was that all victims were investigated by the trained personnel involved in the Toxic Jellyfish Networks under the national surveillance system, indicating that the system is starting to have an impact.
Recommendation
There are different first aid recommendations regarding the steps of removing tentacles.22,24,25 However, any unnecessary steps in the first aid process in life-threatening situations may waste time and increase the probability of death. Thus, the author would like to recommend the following critical first aid steps for suspected lethal jellyfish injury: 1) pour vinegar over the wound continuously for at least 30 s (do not use fresh water and do not rub); 2) if the patient is unconscious and is not breathing/has no pulse, start cardiopulmonary resuscitation; 3) if there is more than 1 rescuer, the other rescuer should call for help/ambulance and calm the injured person; and 4) do not waste time or increase risk by removing tentacles.
Conclusion
Dermatological effects of box jellyfish envenomation included edema, erythematous caterpillar track rash, blistering, bullae, papular eruption, necrosis, digital gangrene, recurrent dermatitis, dermal hypersensitivity, numbness, lichenification, hyperpigmentation, keloid, and scarring. Suffering and healing continued and lasted from several weeks to many years. Direct contact with tentacles had more impact than indirect contact. All fatal victims collapsed within a few minutes, and they also received incorrect or no first aid. The proposed first aid steps for life-threatening box jellyfish stings are the pouring of vinegar over the wound continuously for at least 30 s and starting cardiopulmonary resuscitation if the victim has no respiration or pulse. Tentacles often detach spontaneously, and removal is not always necessary, thus saving time. The findings of this study are useful for health professionals and provide input for improving diagnosis and treatment guidelines.
Footnotes
Acknowledgments
The author would like to thank the Chief and staff of the Department of Community Medicine and the Dean of the Faculty of Medicine, Chiang Mai, for administrative support. This work acknowledges the role of the Toxic Jellyfish Networks for their contribution to the surveillance system.
Financial/Material Support: None.
Disclosures: None.