
Abstract
Jellyfish have been increasing at a global scale in recent years. These blooms not only have deleterious effects on marine ecosystems, they also increase the risk of jellyfish stings and accompanying envenomation. Here, we report a fatal case of pulmonary edema caused by jellyfish envenomation in a child in Korea. The patient died 4 h after envenomation despite cardiopulmonary resuscitation. Nemopilema nomurai was the suspected species of jellyfish encountered by the patient, although we are unable to confirm this. With this case report, we aim to inform on the serious issue of toxicity associated with jellyfish species that bloom mainly along Korean, east Chinese, and Japanese shores and to discuss appropriate first aid methods in case of jellyfish stings.
Keywords
Introduction
Globally, the jellyfish population has increased in recent years, 1 and Korea has not escaped this trend. Jellyfish populations fluctuate widely with shifts in the ocean climate, and a sudden outburst is known as a “bloom.” The reasons for the recent population explosion have not been identified but may include warmer sea water temperatures consequent to global warming, the overfishing of natural predators, or industrialization. 2 Jellyfish blooms not only deleteriously affect the marine ecosystems, they also increase the risk of jellyfish sting and accompanying envenomation. The Korea National Health Insurance system has reported an elevated number in patients requiring medical treatment of jellyfish stings, with an increase from 436 cases in 2009 to 1122 cases in 2013. 3 Here, we report a fatal case of pulmonary edema presumed to be caused by Nemopilema nomurai stings in a child in Korea.
Case Report
In August 2012, an 8-y-old girl with no previous medical history screamed and fell down while swimming in the Yellow Sea of Korea at 1126. Her mother immediately ran to attend the girl, who reported that she had stepped on a jellyfish and felt a sudden stinging sensation as it enwrapped her legs. She complained of intense pain in her legs. A lifeguard at the beach flushed the wound with seawater, sprayed vinegar, and transported the patient to a local clinic. Upon arriving at the clinic, the patient was alert and oriented and was given acetaminophen for pain control. No tentacles were observed on her leg wound, which the physician disinfected with alcohol at 1235. An hour later, the patient began vomiting and was transferred to our emergency medical center.
In the ambulance, she complained of chest pain and began to lose consciousness. Her oxygen saturation dropped, leading the paramedic to apply an oxygen mask. Upon arrival at the emergency medical center at 1433, she was unresponsive to pain and her blood pressure and oxygen saturation levels were uncheckable. Her pulse was 35 beats⋅min-1, and her body temperature was 35°C. Her lips were cyanotic, and she was foaming at the mouth. Multiple linear erythematous lines were visible all over her legs. These lines, which exceeded 20 cm in length, were found on the dorsal and ventral surfaces, and appeared as whip marks encircling her legs. Violaceous petechial hemorrhages were also observed over the lines. The Palmer method was used to estimate an area of contact comprising 36% of her total body surface area.
Chest auscultation indicated widespread coarse inspiratory and expiratory crepitations. An arterial blood gas analysis revealed the following: pH, 6.92; arterial carbon dioxide partial pressure, 45 mm Hg; arterial oxygen partial pressure, 52 mm Hg; bicarbonate, 8 mEq⋅L-1; and oxygen saturation, 60%. The patient was intubated, and profuse amounts of frothy sputum were continuously suctioned from the endotracheal tube. Cardiopulmonary resuscitation (CPR) was commenced because of the lack of a palpable pulse; however, pulse was recovered after 5 min. At that time, the patient's blood pressure was 103/81 mm Hg, and her pulse was 178 beats⋅min-1. A chest radiograph showed haziness in both lung fields that was compatible with pulmonary edema without cardiomegaly, and an electrocardiogram revealed tachycardia with a right axis deviation (Figure 1). The laboratory findings are shown in Table 1.
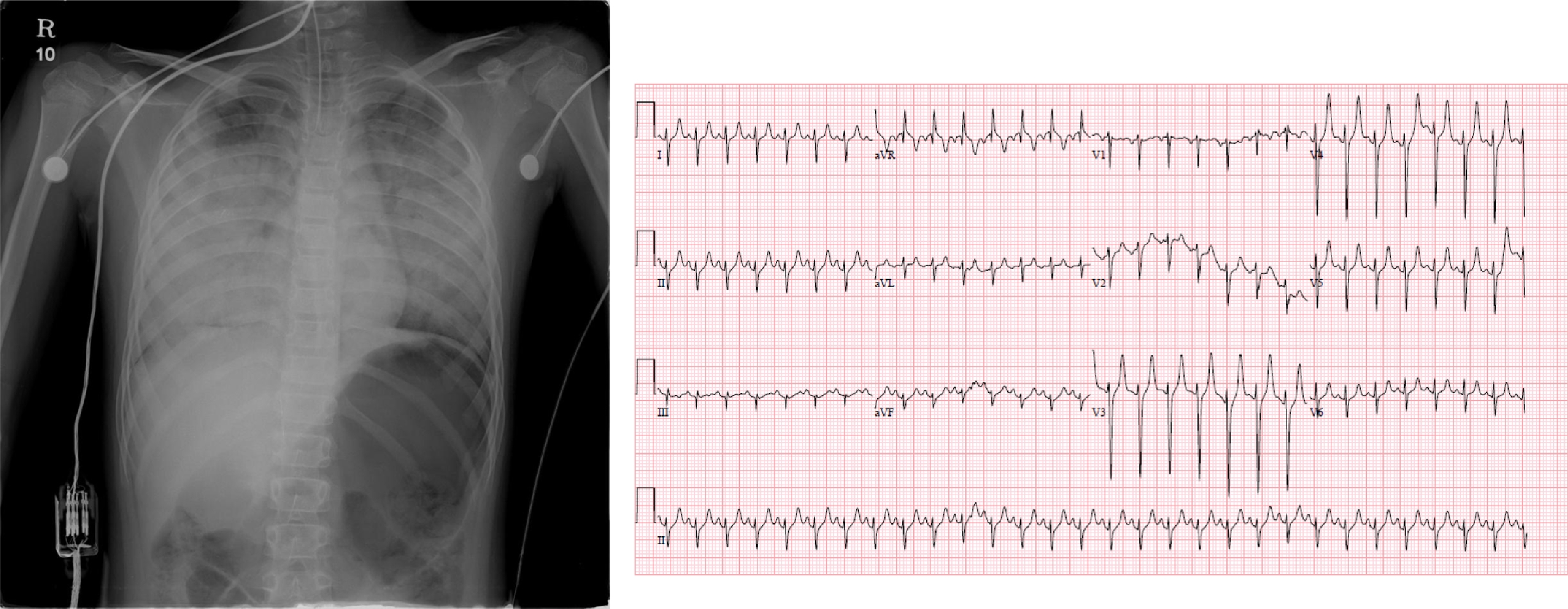
Chest radiograph and electrocardiogram.
Laboratory findings
CRP, C-reactive protein; AST, aspartate aminotransferase; ALT, alanine aminotransferase; BUN, blood urea nitrogen.
Upon observing asystole via cardiac monitoring, CPR was restarted. The patient was administered various drugs including multiple doses of intravenous epinephrine and sodium bicarbonate. She also received biphasic defibrillation at a dose of 100 J after detection of ventricular fibrillation during CPR. Although CPR was performed for 45 min until 1558, the patient could not be resuscitated. Her death occurred 4 h after envenomation. After the incident, the regional coast guard was dispatched to remove jellyfish swarms from the area on the same day, finding 5 N nomurai and no other species (Figure 2A)

A, The regional coast guard was dispatched to the area where the patient was wounded on the same day and found Nemopilema nomurai while removing the jellyfish swarms (this picture was provided by the regional city hall). The 2 dominant jellyfish species mainly found in Korea during the first half of August 2012: B, Nemopilema nomurai; C, Aurelia aurita.
Discussion
In recent years, jellyfish blooms have been observed along the coast of South Korea. According to the weekly reports from the Korean jellyfish monitoring network, N nomurai and Aurelia aurita were the 2 most frequently detected species in Korea during the first half of August 2012 (Figures 2B and C) (
We were unable to confirm the species of jellyfish encountered by the patient in our case. However, as the fatal N nomurai was the predominant species caught at the beach at the time of her injury, we assume that this species was the most likely culprit, consistent with Kang et al. 11 Still, other species present in the region sporadically or in smaller numbers might also have caused this case of envenomation.
The cardiovascular effects and cytotoxic and hemolytic activities of N nomurai venom in rodent models have been previously reported.2,12 The venom exhibits selective cytotoxicity against cardiac tissues and induced hypotension and bradycardia in a dose-dependent manner. Choudhary et al 13 also found a dramatic dose-dependent decrease in the force and rate of spontaneous atrial contractions in response to N nomurai venom. Moreover, Lee et al found that S meleagris could induce severe kidney and liver damage, as well as pulmonary edema and malignant pleural effusion. 14 They concluded that acute renal failure may be among the most important factors contributing to death after a severe sting.
Our case details were consistent with those of previous studies. 12 –14 The observed shock with bradycardia and pulmonary edema, normal-sized heart on chest radiograph, and increased level of creatinine kinase suggest that the patient very likely experienced acute heart failure caused by the venom. The patient's large body surface area and extensive area of contact with the jellyfish would have contributed to her fatal outcome. Given her laboratory results, which indicated severe metabolic acidosis, hyperkalemia, a reversed calcium:phosphorus ratio, and low albumin, acute renal failure might also have played a role in cardiac arrest, despite a normal creatinine level. We further suggest that increased vascular permeability may be as a contributing factor. The patient exhibited severe pulmonary edema, as indicated by the profuse frothy sputum ejected from the endotracheal tube, and her laboratory results indicated hemoconcentration and a decreased serum albumin level.
Finally, we believe that this case eludicates a very important point regarding the administration of first aid after jellyfish stings. In this case, several types of topical solutions, including vinegar, sea water, tap water, and alcohol, were applied to our patient's wounds. There has been much scientific debate regarding which substances should and should not be used administered during first aid after a jellyfish sting. 15 –17 This issue is important because different species of jellyfish are present in different regions, and the venom compositions differ widely among these species. In a recent study on first aid for N nomurai stings, 15 vinegar, ethanol, and isopropanol were found to exacerbate nematocyst discharge, whereas seawater and lidocaine were recommended as a first aid rinsing agent and pain relief substance, respectively. Emergency medical personnel should be aware of the jellyfish species-specific systemic toxicity and the choice of first aid measures.
Footnotes
Author Contributions
Case concept (SBH); drafting of the manuscript (JHK); critical revision of the manuscript (AD); and approval of final manuscript (JHK, AD).
Financial/Material Support
This study was supported by Inha University Research Grant (55767-01).
Disclosures
None.
Supplementary materials
Supplementary data associated with this article can be found in the online version at
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.