
Abstract
Introduction
Point–of-care ultrasound (POCUS) is used in wilderness medicine and could potentially be the only imaging modality available. Cellular and data coverage is often lacking in remote areas, limiting image transmission. This study evaluates the viability of transmitting POCUS images from austere environments using slow-scan television (SSTV) image transmission methods over very-high-frequency (VHF) hand-held radio units for remote interpretation.
Methods
Fifteen deidentified POCUS images were selected and encoded into an SSTV audio stream by a smartphone and transmitted over a VHF radio. A second radio and smartphone 1 to 5 mi away received and decoded the signals back into images. The original images and transmitted images were randomized into a survey graded by emergency medicine physicians using a standardized ultrasound quality assurance scoring scale (1–5 points).
Results
The difference in mean scores between the original image and transmitted image showed a 3.9% decrease in transmitted image scores, with P <0.05 on a paired t test; however, this is not likely a clinically significant decrease. Comparing transmitted images using different SSTV encodings and distances ranging up to 5 mi, 100% of survey respondents determined the images to be clinically usable. This dropped to 75% when significant artifacts were introduced.
Conclusions
Slow-scan television image transmission is a viable option for transmitting ultrasound images in remote areas where more modern forms of communication are unavailable or not practical. Slow-scan television may have potential as another data transmission option in the wilderness, such as electrocardiogram tracings.
Keywords
Introduction
Ultrasound in the wilderness and austere environment is feasible 1 and has practical field indications such as assessment of extremity injuries, pneumothorax, abdominal injuries, intracranial pressure, cardiac trauma, and high-altitude pulmonary edema, among other conditions. 2 Studies have shown that point-of-care ultrasound (POCUS) in remote settings can dramatically change the management and treatment of patients in the field. 3
The aim of this study was to validate the feasibility and clinical reliability of transmitting POCUS images from austere environments over slow-scan television (SSTV) radio signals for remote interpretation and diagnosis. Slow-scan television, also referred to as narrow-band television, is an image transmission method using audio tones to encode image data. Slow-scan television is a protocol that can be used anywhere that radios are used. Certain radio frequencies are regulated; however, the protocol is universally applicable. These SSTV tones can be transmitted over any audio transmission method that can transmit voice and only take 3 kHz of bandwidth compared with a standard analog television signal that uses 6 MHz of bandwidth. The tradeoff for the low bandwidth is longer transmission times, taking between a few seconds to several minutes to transmit a single still image. This low-bandwidth transmission method made SSTV a staple of the early space race in the 1960s and 1970s, including transmitting the first images of the far side of the moon and transmitting images from the Apollo missions.
Slow-scan television uses varying frequencies of audio tones in order to encode data. The first part of the transmission identifies the signal as an SSTV-encoded signal. The second part identifies the mode of transmission. There are multiple different signaling modes that encode an image at different rates and qualities. 4 Slow-scan television was chosen for this study as a simple analog protocol that does not require specialized equipment when compared with digital transmission. Slow-scan television can be used over various modalities, ranging from low-bandwidth radio frequency to analog hardwired communication lines used in cave rescues. This allows it to be adapted to equipment that is already being used for voice communications in the rescue setting where digital or satellite communication options are not available or are not practical. Slow-scan television has the potential to be used over high frequencies and can be transmitted thousands of miles using ionospheric propagation.
Although rescuers carrying a portable ultrasound probe into austere environments may be comfortable and familiar with image interpretation, transmission of the image to a higher level of care or more experienced clinicians may be necessary. With globally increasing cellular data, multimedia messaging services, and satellite internet, there are a multitude of ways to send medical images and data from the field. These methods, however, are not ubiquitous. In rescue operations, very-high-frequency (VHF) radio remains a predominant method of communication and is generally limited to audio-only transmissions. The use of SSTV encoding of medical images, such as ultrasound images, as discussed in this study, could be a viable way of transmitting data via VHF radio or other means out of the field or rescue setting for further diagnosis or care in higher settings.
This study was designed as a proof of concept that POCUS images can be transmitted over SSTV protocol and to assess whether or not the images remain clinically useful. A literature search found no current research on use of SSTV transmission of medical images.
Methods
The Carilion Clinic Institutional Review Board has given an exemption for this research due to no involvement of human subjects.
A selection of 15 POCUS images was chosen from a bank of anonymized ultrasound images obtained from our emergency medicine department faculty. All images were obtained with the original version of the Butterfly IQ portable ultrasound probe. A diverse selection of images was chosen, including vascular, musculoskeletal, obstetric, and abdominal images. High-quality still ultrasound images were preselected to eliminate operator variability (Figure 1). The original size of these images was 632×1080 pixels. Dynamic images or clips were not investigated. The goal of this study was to assess the clinical relevance of still images transmitted over this protocol.
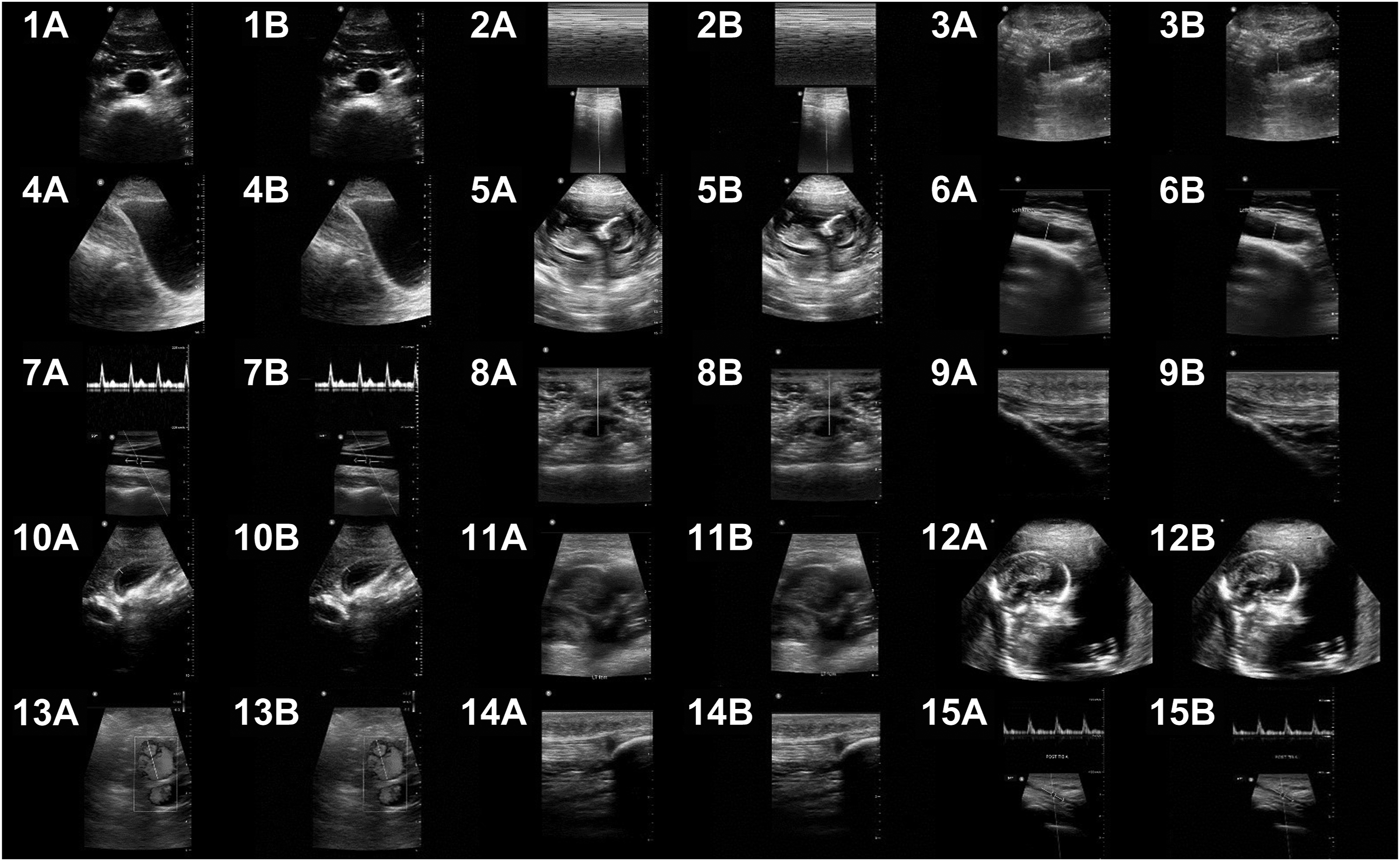
All 15 images. A, Original resized images. B, Transmitted images: 1) aorta; 2) lung; 3) appendix; 4) bladder; 5) fetal; 6) knee; 7) carotid Doppler; 8) nerve; 9) tendon; 10) gallbladder; 11) deep vein; 12) fetal; 13) vascular flow; 14) musculoskeletal; 15) tibial artery.
Two Baofeng hand-held amateur band (HAM) radios were attached to 2 smartphones via an automatic reporting system (APRS) cable that is used for transmitting data or audio from a smartphone or computer to a HAM radio (Figure 2). This APRS cable was used to transmit SSTV-encoded audio signals from the transmitting smartphone’s headphone jack to the radio’s microphone input and from the receiving radio’s output to the microphone jack on the receiving smartphone. This allowed audio to be sent directly between the smartphones and the hand-held radios without interference from ambient noise. The smartphones had applications installed for encoding and decoding SSTV signals (“SSTV Encoder” by Olga Miller and “Robot36 - SSTV Image Decoder” by Ahmet Inan, respectively).5,6 These applications are built for Google’s Android operating system; however, equivalent iOS applications exist for Apple devices.
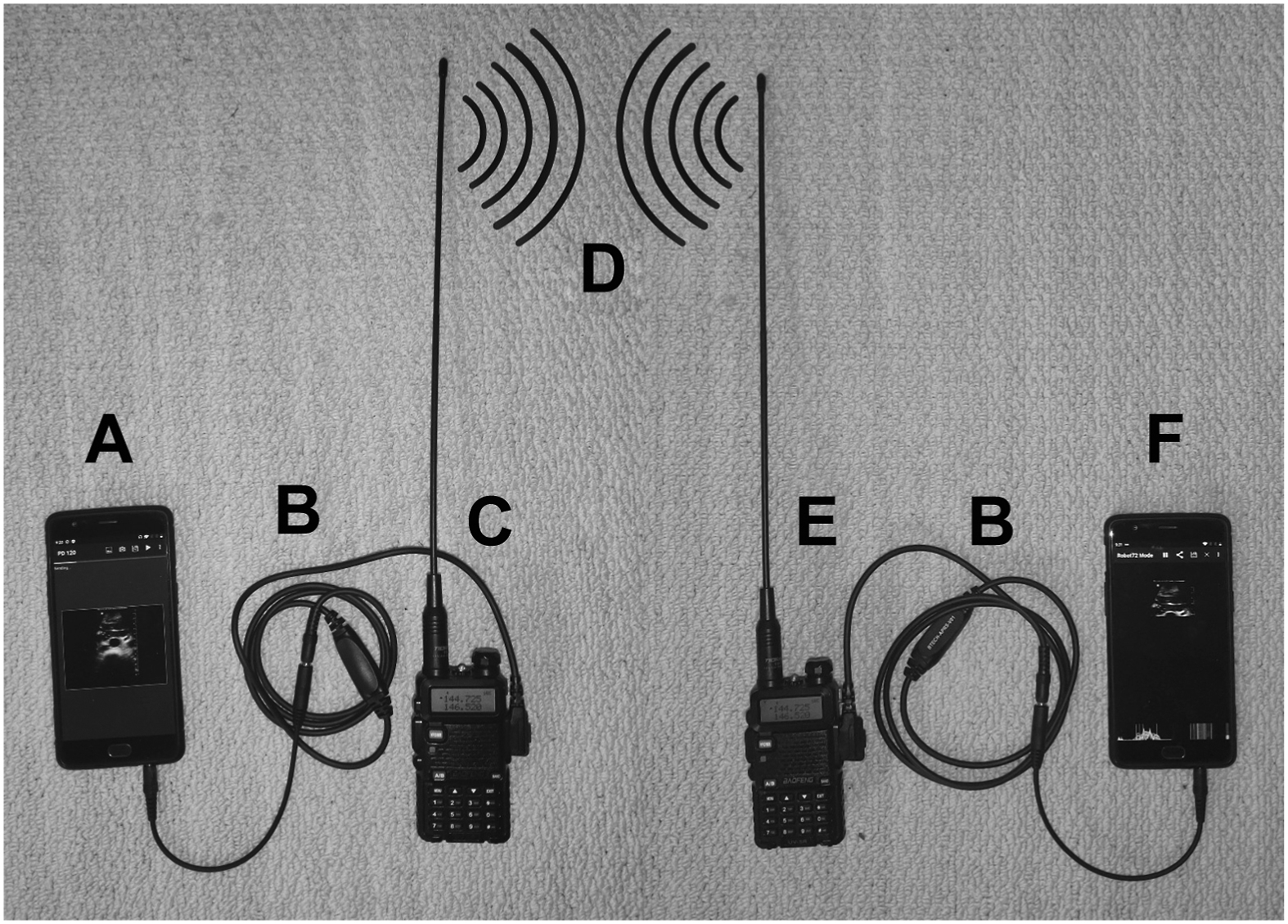
Photograph of the transmission setup. A, Transmitting smartphone running the SSTV Encoder application; B, automatic reporting system cables; C, transmitting radio; D, illustration of radio waves; E, receiving radio; F, receiving smartphone running the Robot 36 application.
Slow-scan television encoding can be accomplished by multiple different encoding protocols or modes. We selected the Robot 72 mode. The Robot 72 mode is one of the quicker methods of transmitting an image, taking just 72 s to send the required data, as the name suggests, with reasonable quality. The received Robot 72 images are 320×240 pixels regardless of original image size.
The 15 original POCUS images were loaded onto the transmitting phone’s internal storage. The second receiving phone and radio setup were positioned approximately 1 mi away in the line of sight. The Robot36 application was launched on the receiving phone (Figure 2f) and immediately started listening to the audio output from the radio, waiting to detect an SSTV start signal. The SSTV Encoder application on the transmitting smartphone was opened, and 1 of the 15 ultrasound images was selected (Figure 2a). The application converted the image into SSTV-encoded audio that was then directed to the HAM radio’s input jack and transmitted on a 144-MHz band (Figure 2c and d).
The receiving radio (Figure 2e) was monitoring the same channel on the 144-MHz band and transmitting the audio to the receiving smartphone over the second APRS cable (Figure 2b). Once the Robot36 application detected the SSTV start signal and signals identifying the mode of encoding, it automatically started decoding the audio signal back into an image (Figure 2f). When the end-of-transmission tones were detected, the application automatically saved the images as a JPEG file on the second smartphone’s internal storage.
This process was repeated 15 times for the 15 selected POCUS images. All original images and transmitted images were stored and sorted (Figure 1). This study was performed on a clear day during daylight hours.
Once the initial test had been completed, 1 POCUS image of an aorta was selected for a quality comparison test of different protocols and distances (Figure 3). We obtained the following quality comparisons: A Robot 72 image obtained without using the APRS cable at a range of 1-mi line of sight. For this setup, the first smartphone’s speaker was playing the SSTV audio signal while the operator held the HAM radio adjacent to it and held down the radio transmit button. The second radio received the transmitted SSTV signal and played it over the built-in speaker while the second operator held the receiving smartphone’s microphone adjacent to the radio so it could listen and decode the signal. This setup had potential for ambient noise (wind, cars, birds, etc.) interference on both the transmitting end and receiving end. This was the only image obtained without using the APRS cable, thus introducing the potential for interference from ambient noise (Figure 3a). Faster 36-s encoding mode “Robot 36” at 1-mi line of sight (Figure 3b). The same Robot 72 encoding at 1 mi that was used for the above 15 comparison images (Figure 3c). The Robot 72 mode at approximately 3.5-m line of sight (Figure 3d). The Robot 72 mode at approximately 5 mi, no longer line of sight (Figure 3f). A slower but higher-quality 120-s “PD 120” mode at 1-mi line of sight (Figure 3g). An even slower but higher-quality 240-s “PD 240” mode at 1-mi line of sight (Figure 3h). A Robot 72 mode at about 5 mi, with multiple obstructions between transmitter and receiver, to demonstrate a worst-case scenario (Figure 3i).
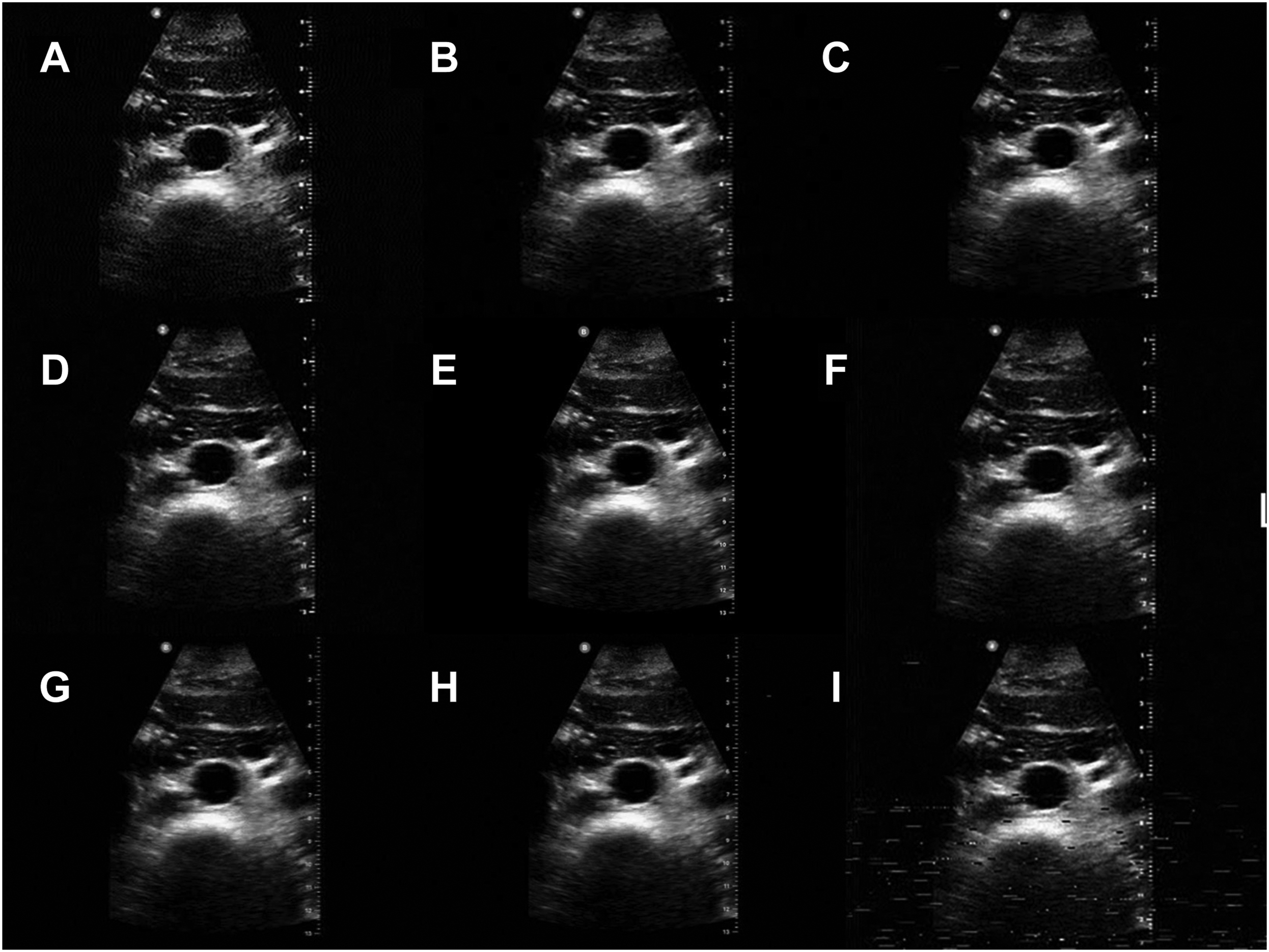
Nine quality comparison for point-of-care ultrasound (POCUS) images of an aorta. A, Robot 72 encoding without using an audio cable (with ambient noise interference) at 1 mi; B, Robot 36 encoding at 1 mi; C, Robot 72 encoding using an audio cable at 1 mi; D, Robot 72 encoding at 3.5 mi; E, original POCUS image using the Butterfly IQ probe before transmission; F, Robot 72 encoding at 5 mi; G, PD 120 encoding at 1 mi; H, PD 240 encoding at 1 mi; I, Robot 72 encoding while the transmitter was driving through the city between buildings and under bridges.
All these images were recorded and cataloged. Both the original and transmitted images were converted to a resolution of 640×480 pixels to prevent bias between different image sizes (Figure 1). No enhancement or any other changes to the images were made.
A survey was developed using a standardized image quality assurance scale using Telexy Qpath software, which is commonly used in emergency ultrasound programs.7,8 This scale allows reviewers to rank images on a 5-point scale (Table 1).
Point-of-care ultrasound image scoring criteria
The 15 resized original images and the 15 resized transmitted images were randomized into the first 30 questions of this survey. The image of the aorta was included twice—2 original images and 2 transmitted images—to validate consistency of responses between identical images, making for a total of 32 randomized images. These 32 images were placed in the survey with the scoring system listed in Table 1 as response choices.
The final question of the survey included a grid of 9 images that included the resized original POCUS image (Figure 3e) of the aorta along with the 8 quality comparisons described above (Figure 3). The survey asked respondents to select every image in the grid that they considered high enough quality for clinical use.
Respondents were also asked to select their primary specialty, additional ultrasound training, and years of ultrasound training when completing the survey.
This survey was distributed to the emergency medicine faculty at our hospital and to colleagues at partnering facilities. Responses were recorded in a spreadsheet.
The responses for each image were averaged for the 32 initial images. The responses for the 2 identical original aorta images were averaged together, as were the 2 transmitted aorta images, resulting in 30 total averages on the 5-point scale. The difference between the original image and transmitted image for each of the 15 POCUS image pairs was obtained to eliminate bias of the respondents’ perception of the original POCUS image quality. This difference between scores for each of the 15 image pairs was statistically analyzed using the paired t test. A P value was obtained from the paired t test.
The scores of the 2 original aorta images and those of the 2 transmitted aorta images were compared using paired t tests to validate respondent consistency between identical images. A P value was obtained from both of these paired t tests.
Results
There were a total of 16 survey respondents. One hundred percent of respondents were emergency medicine physicians, with 44% of respondents having no additional ultrasound training beyond their emergency medicine training, 12% reporting additional ultrasound training (other than fellowship, not specified), and 44% being fellowship trained in ultrasound. The majority of respondents (63%) reported >8 y of experience reading and interpreting ultrasound images (Figure 4).
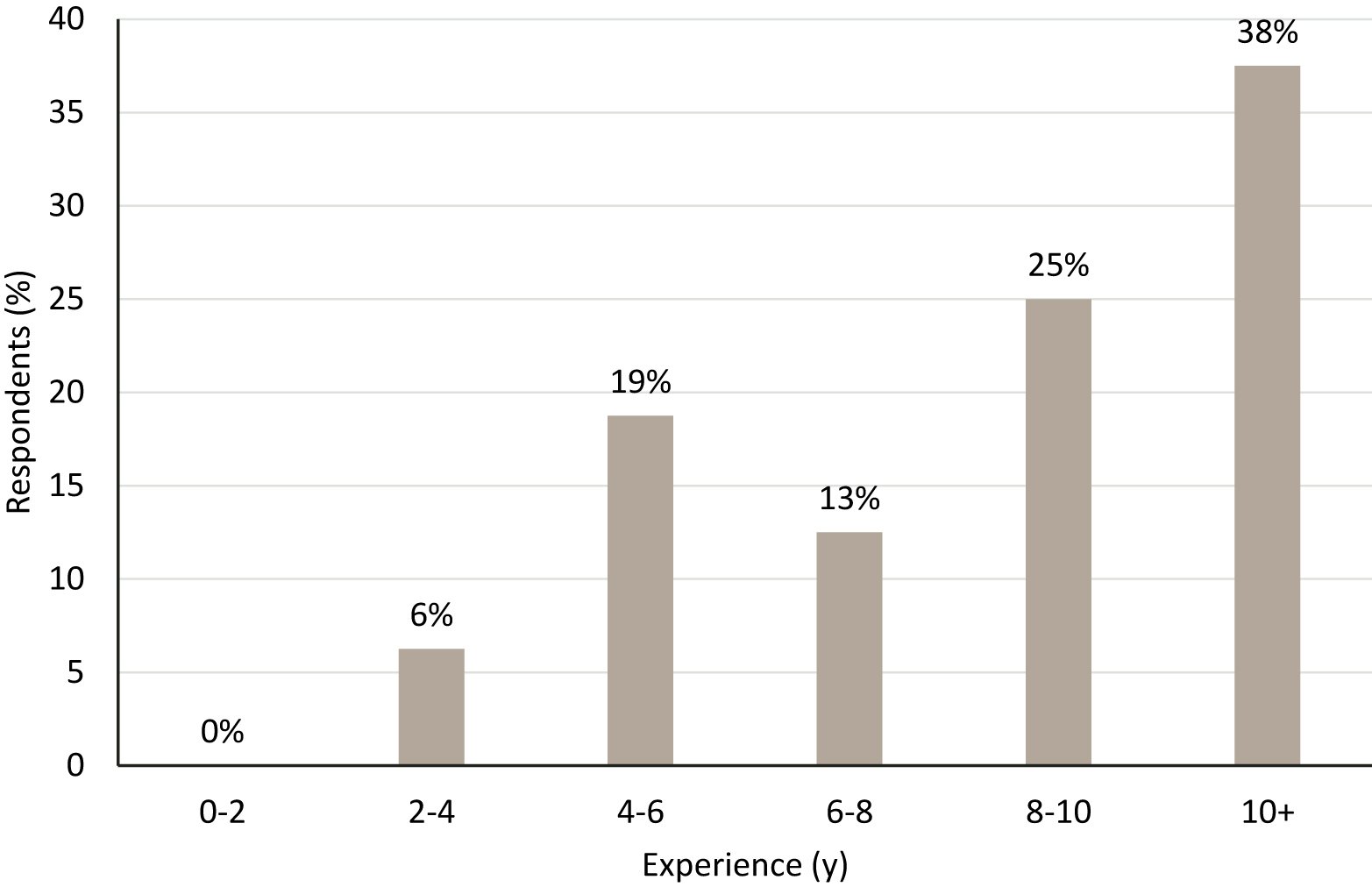
Ultrasound experience (in years) of survey respondents (n=16).
The difference between the original image score and transmitted image score on the 5-point scale ranged from 0 to 0.38 out of 5. The average difference in scores showed a 3.9% decrease in transmitted image scores. A paired t test showed a statistical difference in average scores between the original and transmitted images (P<0.05), indicating that the original images were, on average, statistically clearer (average mean score, 3.74; SD, 1.01) than the transmitted images (mean, 3.60; SD, 1.05) (Table 2). Although statistically significant, the differences in mean scores would not likely be clinically significant.
Paired t test analysis using mean difference between resized original point-of-care ultrasound image and resized image after being transmitted over radios with Robot 72 slow-scan television encoding
Eight of the 9 comparison images of the aorta (Figure 3) were marked as having high enough quality for clinical use by 100% of respondents. These 8 images were as follows: the original image before transmission, Robot 36 encoding at 1 mi, Robot 72 encoding at 1 mi, Robot 72 encoding not using the APRS cable at 1 mi, PD 120 encoding at 1 mi, PD 240 encoding at 1 mi, Robot 72 encoding at 3.5 mi, and Robot 72 encoding at 5 mi. The ninth image was Robot 72 encoding at 5 mi while the transmitter and receiver were separated by multiple obstructions that caused more transmission artifacts. This last image was used to simulate transmission from a wilderness environment to an urban environment with a more definitive provider. Only 75% of the respondents marked this last image as having high-enough quality for clinical use.
The difference between the 2 identical original aorta image scores was analyzed using the paired t test, which produced a P value of 0.43, indicating that there was no difference in the average image scores between the 2 original aorta images. Similarly, the P value for the paired t test between the 2 identical transmitted aorta images was 0.68, also indicating that there was no difference in the average image score between the 2 transmitted aorta images.
Discussion
Images transmitted over HAM radio via SSTV encoding only showed a 3.9% decrease in transmitted image scores compared with original POCUS image scores. Although this result was statistically significant, this difference on a 5-point grading scale would likely not be clinically significant, as any score of ≥3 on the scale indicates that the image could be useful clinically for diagnosis. This proof of concept for image transmissions indicates that despite some image degradation, there is potential for clinical application of this method in environments lacking other data transmission options.
Although cellular service and internet connectivity are growing, there remain many areas of the world without reliable data service. Satellite communication is likely a superior option if available, although the downsides are higher cost and the need to have a subscription.
The radios used in this study were entry-level radios transmitting on a short-wavelength band over short distances. Although not studied in this preliminary trial, it can be hypothesized that with proper equipment and use of existing infrastructure of radio repeaters, these radio signals may be able to transmit images over extended distances. Further study demonstrating this would be beneficial.
In order to utilize this system, preparation is required. First, the application for encoding SSTV images needs to be installed on a compatible smartphone, as downloading the application would not be possible in remote environments with no data signal. Second, someone with ultrasound image interpretation skills would have to be monitoring for image transmission. This can be utilized when ultrasound images are obtained by an individual trained in basic ultrasonography but without the skills for or knowledge of interpretation. Examples could be an emergency medical service rescue squad or remote ranger station with a medical responder. Although an APRS cable was used to transmit audio in this example, it is not required. The benefit of using a cable is eliminating audio interference from ambient noise, thus improving image quality. All of the respondents agreed that the image sample transmitted without the APRS cable was clinically usable; however, in noisy environments, this could lead to significant image artifacts, resulting in unusable images. The process of sending images via cable or audio tone is simple and could easily be replicated by anyone comfortable using a hand-held radio and a smartphone.
Images in this study were transmitted in optimal conditions between 1 and 5 mi away from the line of sight on a clear sunny day. Rescue environments are generally less than ideal. Weather, obstructions, radio transmission, and receiving power are all factors that can affect clarity of audio transmissions and, thus, image quality. The image that was transmitted over 5 mi while the receiving radio was separated by multiple obstructions (Figure 3i) was rated the lowest by respondents of the survey, with only 75% stating that it had high-enough quality for clinical use.
Although SSTV allows images to be transmitted to a nearby receiving radio from an austere environment, often, this is not the end destination of the image. This may be a useful intermediate step to get the image to a location with internet or cellular data coverage so that it can then be sent to the destination, such as a physician or radiologist. With widespread cellular coverage, it is often a short distance, such as from the bottom of a valley to a ridgeline. Our study distance of up to 5 mi reflects this predicted use.
Limitations
This method and study have some limitations. Images transmitted over radio can be decoded by anyone able to receive the signal by using SSTV decoding software such as that used in this study. Patient privacy considerations should be accounted for, as images are not encrypted. Limiting the amount of patient-specific data that are transmitted in images or via voice communications may help protect patient privacy. Privacy concerns are not unique to SSTV image transmissions, as rescuers must consider what is transmitted over traditional voice communications. Encryption methods might be possible but were not tested in this study, and further investigation would be needed to determine viability of encrypted images.
This study was performed in a rural setting over short distances as a proof of concept. Further validation over longer distances and in more remote locations should be performed. Varying weather conditions should be further explored, as this study was conducted with clear skies and during daylight hours. Future studies could assess the ability to make a diagnosis and evaluate image quality for more subtle pathologies. This protocol only sends static images. Dynamic ultrasound examinations cannot be transmitted using this method, making some diagnoses more challenging.
There were only 16 physicians who rated the images. All of the raters were emergency physicians with variable levels of additional training; however, all respondents routinely interpret POCUS images as part of their clinical practice. They represent clinicians who could potentially interpret transmitted images through online medical control. Another limitation is that a complete eFAST examination was not used, and more challenging images could be introduced and compared in the future.
This study only examined transmission of POCUS images over SSTV; however, any image can be sent via this method. There is potential for other clinical uses in the backcountry, such as transmission of patient injury images, EKG tracings, and other patient data, to assist in remote medical management and rescue planning. Research into viability for other clinical uses can be further investigated.
Conclusion
As POCUS has become more widely available, the use of hand-held radio and SSTV encoding presents a low-cost and accessible option to transmit clinically useful images from austere locations to more definitive communication methods or to an end destination of providers trained in their interpretation. Images transmitted using this technique over short distances are of sufficient quality to be utilized for clinical diagnosis by emergency medicine physicians or other experienced ultrasound diagnosticians. Further investigation can be completed to assess transmission quality in less optimal terrain and weather conditions. Use of publicly available repeaters to cover extended distances can be explored.
Footnotes
Acknowledgements
Author Contributions: conception of idea and organization of study (CMH); literature review (CMH, SAL); experiment and data collection (CMH, SAL, CPW); statistical analysis (ERL); drafting and editing of manuscript (CMH, SAL); review, edit, and approval of final manuscript (all authors).
Financial/Material Support: None.
Disclosures: None.