
Abstract
Toxicodendron dermatitis is an underappreciated disease seen in the emergency department. Although self-limiting, symptoms can be distressing and can last for weeks if untreated, particularly with re-exposure. Continuing research has improved our understanding of specific inflammatory markers that are associated with exposure to urushiol—the compound responsible for Toxicodendron dermatitis—although consensus for treatment remains varied and poorly supported. Owing to the lack of recent primary literature on the topic, many providers rely on historical precedent, expert opinion, and personal experience when treating this disease. This article provides a narrative review of the literature currently available on the effects of urushiol on key molecular and cellular functions and the prevention and treatment of Toxicodendron dermatitis.
Introduction
Contact dermatitis is defined as “inflammation of the skin caused by irritants or allergic sensitizers.” 1 This can result from either direct contact with an offending agent or contact between an exogenous agent and mucous membranes. Contact dermatitis generally falls into 2 categories: irritant or allergic. Although irritant contact dermatitis is confined to the area of contact, allergic contact dermatitis (ACD) extends beyond the areas of contact and can additionally cause systemic involvement. 1 In the United States, Toxicodendron dermatitis is among the more common causes of ACD, particularly in the forestry and agriculture industries and in rural populations. 2
Toxicodendron dermatitis is caused by direct exposure to urushiol—a small, lipophilic molecule found in the sap of Toxicodendron genus plants, such as poison ivy, poison oak, and poison sumac. 2 It is characterized by a linear weeping, pruritic rash that appears over the first hours to days after exposure, although in susceptible individuals without treatment, symptoms can last for up to 6 wk. 2 Given the potentially prolonged course of illness and general lack of organized recommendations, this review will discuss the epidemiology of, basic pathophysiology of, and treatment recommendations for Toxicodendron dermatitis, particularly as it relates to the emergency medicine provider, with a focus on pre-exposure prophylaxis and postexposure treatments.
Methodology
The articles were selected by the study authors with a focus on English-language articles based in the United States and published between 1991 and 2016, using PubMed to access and obtain the selected articles, and using the keywords “Toxicodendron,” “poison ivy,” “poison ivy treatment,” and “urushiol” to obtain our results. This search was supplemented with searches in Embase, UpToDate, and Google Scholar. We narrowed our review focus primarily on studies that discussed methods of prevention of ACD as well as articles comparing various treatments of ACD. Given the dearth of available studies, we chose to include studies with smaller sample sizes to maximize the available data for review. We did, however, exclude studies that focused on other categories of ACD unless they specifically discussed ACD secondary to Toxicodendron species. In our treatment section, we chose to evaluate over-the-counter and prescription medications commonly available in the United States.
Epidemiology
Dermatologic-related complaints account for more than 7.1 million clinic visits in the United States each year, with allergic urticaria accounting for 2.08% of these conditions.2,3 Toxicodendron exposure alone results in an estimated 43,000 visits to the emergency department (ED) and more than 100,000 clinic visits each year. 4 In 2020, poison ivy was the sixth most common plant exposure reported to the Poison Control Centers and the third most frequent plant exposure where positive plant identification was made. 5
It is estimated that 75% of the American population is allergic to the urushiol found in Toxicodendron species, with children of allergic parents being 80% more likely to be sensitive themselves.2,6 The national 12-month prevalence for occupational dermatitis is 1700 per 100,000 workers, with a particular predilection for agricultural and forestry industries, making contact dermatitis the second leading type of occupational disease in the United States. 7
Although the 3 primary species of Toxicodendron plants—poison ivy, oak, and sumac—vary somewhat in their physical appearance, the molecular differences in their oils vary only minimally and cause similar reactions. Poison ivy is a vine consisting of 3 broad, tear-shaped leaves (see Figure 1). Poison oak grows as a vine or shrub with broad leaves. Poison sumac is a shrub or small tree consisting of long, tapered leaves with smooth edges and pointed tips.2,8,9

Poison ivy (Toxicodendron radicans) in the spring at Mohawk Park, Tulsa, Oklahoma. Photo by author R. Massey.
Although the morbidity of this disease process is low and can often be managed at home, some cases can elicit severe and occasionally prolonged reactions, warranting the involvement of healthcare providers and supporting the need for thoughtful treatments.
Pathophysiology
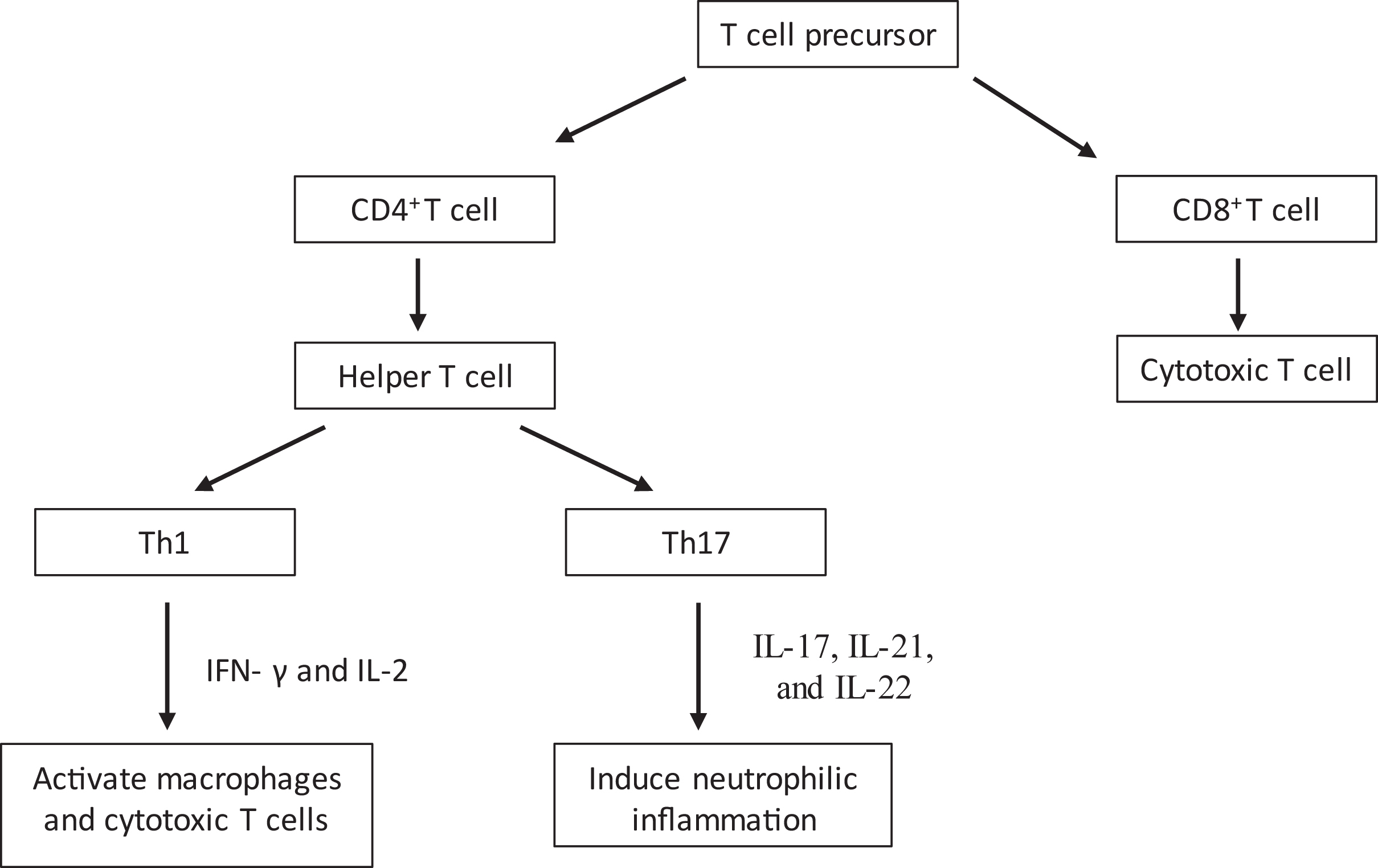
Toxicodendron species contain the lipophilic oleoresin urushiol, which can be absorbed into the skin within 30 min of contact and may result in a T cell–mediated type IV hypersensitivity reaction.2,10,11 The activation of 2 cascades propagates tissue injury by T cell–mediated cytotoxicity and a cytokine-induced inflammatory response. 10 The first mechanism releases proinflammatory cytokines via effector CD4+ cells that have sensed a foreign antigen presented by macrophages, whereas the second pathway involves cytotoxic CD8+ T cells directly destroying target cells and releasing additional inflammatory cytokines (see Figure 2 for details).10,12
Treatment
Sensitization after initial exposure to urushiol primes the immune system to respond with the classic hypersensitivity reaction upon repeat exposure. The goals of therapy for ACD include exposure prevention, decontamination, and treatment of symptoms. 1
Exposure Prevention
Prevention of ACD is rooted in individuals with a history of Toxicodendron-induced dermatitis taking precautions to prevent re-exposure. Prevention is focused on avoiding disease-causing vegetation or protecting oneself by dressing in dry, loosely woven fabrics and the use of vinyl gloves.2,13 Moisture-wicking fabrics can absorb the urushiol oil and can remain active on clothing for years; therefore, decontamination with washing is needed to prevent sustained exposure. Wash exposed clothing and equipment in soap and water within 30 min of exposure before the urushiol oil is fully absorbed.1,2 Unfortunately, many are unaware they have been exposed to the oil, are unable to readily wash the affected area, or are unaware that vigorous washing may expand the area of exposure, resulting in the need for decontamination or treatment of symptoms.2,13
Protection Against Exposure And Decontamination
Several commercially available products act by either preventing exposure or decontaminating skin after exposure. Grevelink et al 14 conducted a low-powered study (n=20) comparing the efficacy of 7 different barrier creams against Toxicodendron dermatitis. Each cream was added to a small area on the forearm, leaving 1 area untreated. Patients were then exposed to Toxicodendron plant extracts, and reactions were monitored. The 3 patients with areas that remained asymptomatic had been treated with barrier creams that utilized a water-repellant base. 14 Several other marketed agents (eg, IvyX, Ivarest) have not been subjected to standardized testing but are postulated to relieve symptoms with ingredients such as pramoxine. 15
Only a few products have been independently tested. In 2000, Stibich et al 16 studied a small cohort of medical students (n=20) exposed to urushiol and reported that Tecnu, a waterless cleansing solution, provided 70% protection from erythema, vesiculation, and induration, compared with control. Davila et al 17 (2003) reported that application of Zanfel, a product that reportedly inactivates urushiol by binding and removing it, significantly improved Toxicodendron-induced ACD when compared with placebo, although this report is limited by its small sample size (n=24) and lack of peer review 18 . With the paucity of literature that exists, more well-designed and appropriately powered studies are needed to determine the efficacy of commercially available products.
Unfortunately, protection or decontamination may not occur in time to prevent symptoms, leading us to reactively manage symptoms of ACD.
Symptom Management
Discharge and pruritus associated with ACD may respond to the use of an astringent such as aluminum acetate, which exerts its main effect through vasoconstriction. This product decreases inflammation, reduces exudates, and allows new tissues to maturate underneath the protective coat formed by the protein precipitate. 13
Medical Management Of Clinical Effects
Topical steroids (eg, hydrocortisone cream 1%) are available over-the-counter options for the treatment of pruritus but may be ineffective because of their low potency. 2 Higher-potency topical steroids are available by prescription and vary widely in formulation. 19 Disadvantages of topical steroids are their impracticality for large body surfaces, genitalia, and face as well as the risk of causing thinning skin, discoloration, and adrenal suppression.1,2
Typically, patients who present to the ED have tried over-the-counter treatments with minimal relief. In the ED, systemic corticosteroids are inexpensive and often prescribed for moderate to severe Toxicodendron dermatitis, although such treatments are based on anecdotal evidence and provider preference. Steroids can be administered orally, intramuscularly, or intravenously, all with similar expected bioavailabilities but with varying relative potencies. Emergency department providers most often will prescribe prednisone or methylprednisolone as a first-line treatment, with durations ranging from 1 to 13 d, which is shorter than the recommended duration, leading to subsequent visits to healthcare providers. 4 Oral prednisone dosing is typically 1 to 2 mg/kg/d, but with urushiol-induced dermatitis, longer tapered dosing is necessary to avoid rebound symptoms. 20 Tapers typically last 12 to 21 d, with a gradual decrease in dose every 2 to 3 d. 20 Prepackaged methylprednisolone exists but may not be as efficacious given that the comparable dosage strength is subtherapeutic for treating ACD. 2 Triamcinolone can be administered intramuscularly, but patients should be educated on potential rebound dermatitis and potential soft tissue atrophy. 20
Conflicting evidence exists when researching systemic steroids. When 89 patients with a diagnosis of Toxicodendron dermatitis were studied, the combination of a systemic corticosteroid plus a high-potency topical corticosteroid shortened the duration of itching. 21 Unfortunately, none of the treatment strategies showed reduction in the duration of erythema, papules, or vesicles. 21 Another study comparing the efficacy of a 5-d steroid burst and a 15-d steroid taper in 49 patients showed that those prescribed a taper were less likely to utilize other medications for added symptom relief, but adherence, rate of rash return, medication side effects, and healing time in severe poison ivy dermatitis did not statistically differ between the groups. 22
Because there are many successful treatments available, topical antihistamines are not recommended. 1 A first-generation oral antihistamine can be used to lessen pruritus, but topical ointments can cause drug-induced dermatitis superimposed on the existing ACD. 1 Urushiol-induced ACD works via a histamine-independent mechanism, further supporting that antihistamines are ineffective at treating pruritus related to ACD. 6
Although there are many factors that go into the treatment of ACD caused by Toxicodendron species, provider and patient preference play a large role. Home treatments, such as aluminum acetate and hydrocortisone, are readily available and generally inexpensive. Decontamination treatments are accessible but expensive. With more severe cases of ACD, providers may consider prescribing topical, oral, and/or injectable steroids depending on the severity of symptoms.
Summary
Allergic contact dermatitis is a common yet poorly studied skin condition in the United States and is classified as a T cell–mediated type IV hypersensitivity reaction to the urushiol oil found in Toxicodendron species. Although avoidance is ideal, strategies exist for pre-exposure prophylaxis and postexposure treatment; however, once symptoms develop, treatments differ based on severity of reaction. The emergency medicine provider should consider education on prevention of Toxicodendron exposure, decontamination, as well as symptom management. Prescriptions to consider include topical steroids for mild to moderate cases, systemic steroids at appropriate durations for moderate to severe cases, or combination therapy including a systemic corticosteroid and high-potency topical corticosteroid for the most severe cases. Ultimately, patients and providers can utilize shared decision-making strategies in determining the appropriate treatment necessary.
Footnotes
Acknowledgements
Author Contributions: study concept and design (AQL, KAM, KAA); data acquisition (KAA, RCM, SKL, KAM); data analysis (KAA, RCM, SKL); literature review (KAA, RCM, SKL); drafting and critical revision of the manuscript (KAA, RCM, SKL, KAM, AQL, JMH); all authors approved the final manuscript.
Financial/Material Support: None.
Disclosures: None.