
Abstract
The past few decades of military experience have brought major advances in the prehospital care of patients with trauma. A focus on early hemorrhage control with aggressive use of tourniquets and hemostatic gauze is now generally accepted. This narrative literature review aims to discuss external hemorrhage control and the applicability of military concepts in space exploration. In space, environmental hazards, spacesuit removal, and limited crew training could cause significant time delays in providing initial trauma care. Cardiovascular and hematological adaptations to the microgravity environment are likely to reduce the ability to compensate, and resources for advanced resuscitation are limited. Any unscheduled emergency evacuation requires a patient to don a spacesuit, involves exposure to high G-forces upon re-entry into Earth’s atmosphere, and costs a significant amount of time until a definitive care facility is reached. As a result, early hemorrhage control in space is critical. Safe implementation of hemostatic dressings and tourniquets seems feasible, but adequate training will be essential, and tourniquets are preferably converted to other methods of hemostasis in case of a prolonged medical evacuation. Other emerging approaches such as early tranexamic acid administration and more advanced techniques have shown promising results as well. For future exploration missions to the Moon and Mars, when evacuation is not possible, we look into what training or assistance tools would be helpful in managing the bleed at the point of injury.
Introduction
Space is a remote and hazardous environment, and over the years, space exploration has led to 21 fatalities from 5 events. 1 Most mishaps that involved injuries have occurred during liftoff or re-entry, including drowning incidents, cabin decompression, and blunt trauma. However, there have also been in-flight incidents that could have required emergency management, such as fires, vehicular collisions, and loss of environmental controls.1,2 While there have not been any evacuations for major trauma injury to this day, the possibility of a resuscitation scenario on future missions cannot be eliminated. 3 -5 Recent modeling for a 923-d standard Mars mission (560 d on the surface) has provided a risk estimate of 5.209% for reaching medical evacuation criteria secondary to traumatic injury, such as burns, musculoskeletal injuries, and bleeding. 5 Among these conditions, traumatic hypovolemic shock accounted for 0.193% and ranked highest for reaching loss of crew life, with an estimated risk of 0.107%. 5 Considering the high impact of these injuries on health and mission success, resuscitation protocols informed by mission attributes and targeted toward realistic interventions will be critical.
Trauma resuscitation in space is limited because of a variety of factors, including microgravity, logistical constraints, and vehicle mass and volume limitations. In the case of life-threatening injuries, the International Space Station (ISS) medical kit currently allows for basic trauma and surgical procedures as well as Advanced Cardiac Life Support,6,7 and astronauts are trained in resuscitation scenarios by the “treat first what kills first” principle: securing an adequate airway and managing ventilation before hemorrhage control. 8
In recent years, however, care standards in prehospital and austere environments have seen a paradigm shift. Based on observations that extremity hemorrhage was a leading cause of preventable death in combat casualties, revision of battlefield trauma care recommendations resulted in the development of Tactical Combat Casualty Care (TCCC) guidelines by US military services. 9 By emphasizing “good medicine with good tactics,” TCCC has focused on treating major external bleeding caused by penetrating injury and delaying the onset of hypovolemic shock through the application of direct pressure and aggressive use of tourniquets and hemostatic gauze—even before attempts at managing the airway and breathing. 10 -12 The successful implementation of TCCC has made important contributions to the highest casualty survival rates in the history of modern warfare and reduced fatal casualties attributed to extremity hemorrhage. 13 -16
Lessons learned from the military have been translated into the civilian sector through initiatives such as the Hartford Consensus,17,18 the White House Stop the Bleed campaign, and the development of TCCC-based courses by the National Association of Emergency Medical Technicians. 10 Evidence-based guidelines from the American College of Surgeons Committee on Trauma and the American Heart Association now encourage the use of tourniquets and hemostatic agents in controlling massive hemorrhage in prehospital trauma care.19,20 The wilderness medicine community is adopting TCCC concepts as well, as early intervention becomes more critical with prolonged evacuation times and constrained resources. 21 -24
Space travel represents the ultimate remote medicine setting, with a lack of medical resources (equipment and personnel), unprecedented autonomy, and limited evacuation possibilities. 25 The extreme environmental conditions and physiological changes associated with microgravity 26 may increase the risk of mortality and morbidity in the case of massive external hemorrhage. With ongoing plans to set foot on the Moon and Mars and an increasing amount of flight opportunities for “space tourists,” a careful re-evaluation of current emergency resuscitation guidelines is necessary. To this end, our aim was to examine massive external hemorrhage control and the applicability of TCCC principles in space.
Methods
A literature review was conducted to identify articles about the management of external bleeding and the use of tourniquets and hemostatic agents in austere environments—in particular, the spaceflight setting. PubMed was searched through June 2022 using Boolean combinations of the following key words and their Medical Subject Heading (MeSH) derivatives: “trauma,” “emergency,” “bleeding,” “hemorrhage,” “advanced trauma life support,” “prehospital,” “tactical combat casualty care,” “tourniquets,” “hemostatic dressing,” “spaceflight,” “weightlessness,” “parabolic flight,” “extreme environments,” “wilderness,” “arctic,” “Antarctic,” “submarine,” and “oil platform.” References obtained were crosschecked, and gray literature was searched for additional relevant publications. One hundred two articles were reviewed, representing techniques, protocols, or challenges in the civilian setting as well as extreme and austere environments, outcomes of TCCC concepts in civilian and military settings, or physiological changes in spaceflight that are relevant to initial resuscitation and external hemorrhage control.
Mechanisms of Injury
For long-duration spaceflight, risk estimates have previously been derived by studying analog populations, such as military pilots, submarine crews, and Antarctic winter-over research teams. 27 -29 However, spaceflight poses unique operational and occupational risks that are different from those on Earth. Significant medical events during spaceflight have generally not been related to orthopedic or surgical trauma, which, in contrast, accounts for more than half of the evacuation events from McMurdo Station in Antarctica.27,28 Morbidity from gravity-based events on Earth and other accidental injuries, such as falls and motor vehicle accidents, are not represented in weightlessness.
Nevertheless, minor trauma already occurs in space. A database of in-flight musculoskeletal injuries and minor trauma in the US space program has documented an incidence of 0.021 and 0.015 per flight day for men and women, respectively, with abrasions and contusions being most prevalent, followed by strains and lacerations. 30 Most of these injuries occurred from impacting structures while stowing or translating equipment, exercise, and extravehicular activity (EVA), with a rate of 0.26 injuries per EVA in microgravity alone.
People and objects still possess mass, which can generate significant force when accelerated. In low Earth orbit (LEO), risk of major blunt and penetrating injuries that could involve life-threatening external hemorrhage would therefore be primarily related to the dynamic stages of flight—launch, landing, and docking—or EVA. 31 Potential mechanisms include impact from micrometeorites or crush-type injuries from movement of high-mass structures during space station construction, vehicle docking, and payload deliveries. Vehicular collisions and near-miss accidents have occurred in flight multiple times. 2 In addition, upcoming exploration-class missions will include surface operations in partial gravity, with increasing amount of EVA and heavy work in a highly dynamic environment. 32 For instance, astronauts may be involved in habitat construction, heavy equipment transfer, human-machine interactions, and rover vehicle operations. Increased fracture risk from osteoporosis in space may further add to risk of blood loss from blunt or penetrating injury,33,34 and above all, with the current intensification of activity in the human spaceflight industry, one must take into account that different and unforeseen emergencies could always arise.
Environmental Challenges
In space, trauma management is not as straightforward as in the emergency department. Especially when an astronaut is exposed outside the spacecraft or space habitat, many of the previously mentioned scenarios would be challenged by prolonged time to reach initial trauma care on board. With concurrent spacesuit or spacecraft damage, for instance, protecting the crew from ongoing environmental hazards would be a priority before starting any resuscitation procedures. In case the injured astronaut reaches his crewmates, prolonged times for suit removal and deployment of stowed equipment could cause further delays, and restraining patients and supplies is complicated without gravity.3,35 Although the performance of most Advanced Trauma Life Support procedures appears to be feasible in microgravity, 7 limited shelf lives during long-duration missions and vehicle constraints of available storage space and electrical power may compromise the availability of adequate equipment, medical supplies, and resuscitation fluids such as blood products. 25 In addition, a crew’s medical expertise is generally limited. For current ISS operations, crew members receive approximately 9 h of medical training preflight that includes basic first aid procedures and cardiopulmonary resuscitation. Further hands-on training is provided to 1 or 2 specially designated crew medical officers, who are not required to be physicians, and in total receive approximately 14 to 40 h of medical training that is mostly oriented toward basic skills that enable them to interface more effectively with a flight surgeon on the ground. 6 With real-time communication interruptions and delays of up to 22 min on missions to Mars, ground-based assistance via telemedicine may not be readily available, further compromising the possibilities for adequate damage control. 36
In case of a medical emergency evacuation from LEO, a spacecraft such as the Soyuz or Crew Dragon could technically undock and land within 3 to 4 h. Yet, even with a preferred, nonballistic landing at one of the primary landing sites, it could take anywhere between 5 and 48 h until the patient reaches a definitive healthcare facility on Earth. This may include up to several hours in the spacecraft in which patient access and the provision of any medical care is severely constrained due to the need for pressure suits and cramped conditions.28,36 Also, crew members would be exposed to approximately 4 +Gx during the landing profile. A hemorrhagic shock model in primates undergoing centrifugation has shown that exposure to re-entry acceleration forces significantly increases shock parameters compared with a normovolemic control condition, with more adverse events when the hemorrhage is severe (class III or IV, or >30% loss of blood volume).8,37 Importantly, because uninjured crew members typically display hypovolemic signs of a class I hemorrhage (15% loss of blood volume) due to microgravity-induced fluid shifts and cardiovascular deconditioning in space, a true class I hemorrhage in space may respond much like a class II hemorrhage (15–30% loss of blood volume) upon return to Earth. 38 In case of massive hemorrhage this could seriously compromise a casualty. The alternative of a ballistic re-entry would cause even higher (8 or 9) G stresses, and unpredictable landing sites would further delay appropriate medical monitoring and intervention. 36 Future deep space exploration missions will be even more challenging. Reaching definitive care may take anywhere from multiple days (eg, 4–5 d from the Moon) to multiple months, or, more realistically, may not even be feasible at all.
Cardiovascular Deconditioning and Hematological Changes
Various circulatory physiological changes occur in space that are likely to reduce the ability to withstand the consequences of massive hemorrhage. In the absence of gravity, fluid is redistributed toward the upper body, and the relative hypervolemia at heart level results in compensatory loss of water and electrolytes and a net decrease in plasma volume.26,39 Astronauts have been found to lose 10 to 23% of circulating blood volume within 24 to 48 h in space to reach a new equilibrium of central blood volume that is similar to that in the upright position on Earth. 39 -41 The low variance in gravitational stimuli resets the autonomic nervous system, resulting in overall blunting of the cardiac chronotropic and baroreflex responses to hypotension. 42 -44 Reductions in systemic vascular resistance do not require large contractility of the heart, 45 and cardiac atrophy of 12% has been observed after 10 d of spaceflight. 46 These adaptations may be appropriate for regular microgravity conditions but will significantly increase the impact of any blood loss and reduce the ability to compensate for hypovolemic stress (Figure 1).47,48
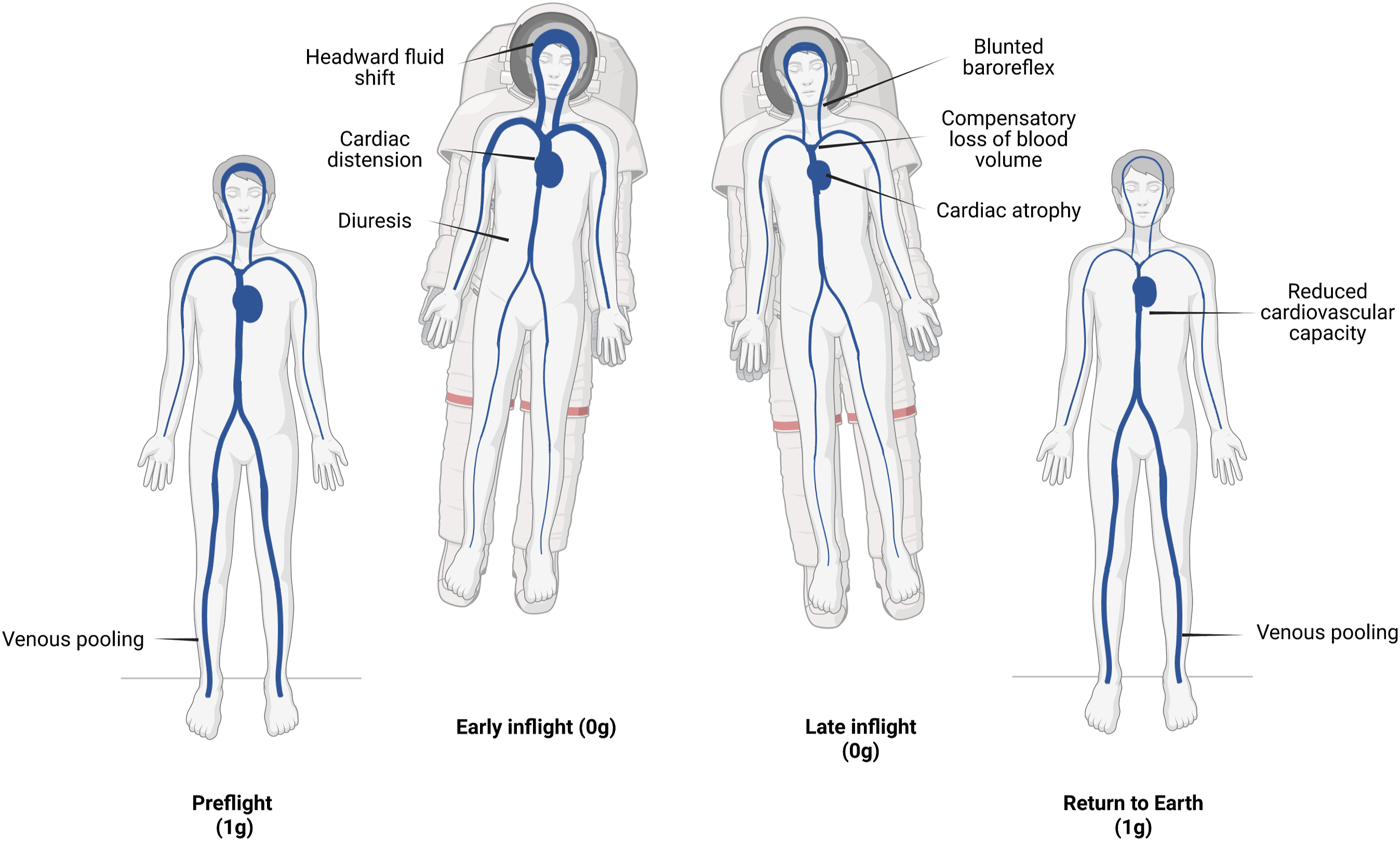
Cardiovascular deconditioning in space. Upon entering the microgravity environment, fluid shifts toward the upper body. After several days in flight, central blood volume is restored to preflight levels through reductions in plasma and red blood cells, and the cardiovascular system adapts to the lower systemic vascular resistance and absence of gravitational stimuli. Upon return to Earth, the normal redistribution of blood volume results in low central blood volume, reduced hematocrit, and an overall reduced cardiovascular capacity to deal with normogravity conditions. Adapted from Charles et al 47 and Gunga et al. 48 Created with BioRender.com.
A decrease in erythrocyte volume of 10% has been found after 1 wk in space, specifically reducing oxygen-carrying capacity in blood circulation. 49 Similar results have been obtained for long-duration missions, with 11% decreases of red blood cell mass after 28, 59, and 84 d compared to preflight,50,51 and nearly half the astronauts showed anemic hemoglobin concentrations after missions longer than 21 d. 52 The severity of this “spaceflight anemia” is likely to increase on longer exploration-class missions, 52 during which this effect may be further amplified by exposure to space radiation. 53
Platelet number and activity have also been shown to be decreased in microgravity conditions. 34 Findings of reduced platelet aggregation and adhesion as well as other altered coagulation systems suggest that hemostasis may be more difficult to achieve in space, 54 despite recent findings of a potentially increased risk for thrombus formation. 55 Systemic vasodilation from high levels of atmospheric carbon dioxide—typically fluctuating between 2.3 and 5.3 mm Hg in spacecraft—may further increase risk of blood loss,56,57 and venous bleeding has also been shown to increase in parabolic flights, possibly because of the lack of venous wall compression. 33
Thus, a massive bleeding—especially as it leads to hypovolemia and coagulopathy in the case of shock—is likely to have a relatively profound impact on the overall outcome of a trauma injury compared with that in the terrestrial setting. The “golden hour”—the period immediately after significant trauma in which intervention has the greatest effect on outcome—may be shorter, 38 and with reduced fluid resuscitation possibilities on board, early hemorrhage control becomes even more critical.25,58
External Hemorrhage Control in Space
Tourniquets
An important factor in the life-saving potential of the TCCC guidelines has been the renewed focus on tourniquet use. While a casualty could administer self-aid by applying direct pressure at the site of bleeding as an effective initial technique, it would preclude a care-providing crew member with limited time and resources from performing other procedures.11,18 With the immediate and correct application of a tourniquet, the crew would have time for conversion to other methods of hemostasis such as hemostatic or pressure dressings.
Well-designed tourniquets can reliably achieve hemorrhage control and have been demonstrated to save lives when applied before the onset of shock,59,60 also in civilian and wilderness settings. 61 -63 Nevertheless, conclusive evidence remains weak.24,64 In terms of safety, tourniquets have remained a controversial topic because of their complications, which are primarily related to ischemia and compression.65,66 Reviews of recent combat and civilian experiences have shown minimal morbidity, but the total tourniquet time in these studies was less than 2 h in most of the casualties. 67 -69 Beyond the 2-h “safe time” limit, slow release of a tourniquet is ideally done in a medical treatment facility with advanced resuscitative capability because prolonged tourniquet time can be associated with life-threatening systemic hyperkalemia and reperfusion injury.11,70,71 If a tourniquet has been in place for more than 6 h, it should not be removed unless close monitoring and laboratory capability are available. 11
No evidence exists of the effectiveness and safety of tourniquet use in space, and risk of complications remains unclear. Although every effort should be made to reassess and convert tourniquets in less than 2 h, prolonged time and impaired medical access in spacecraft during medical evacuation could lead to serious complications. In one military study on 297 limbs, 100% morbidity (amputation or fasciotomy) was recorded after a tourniquet duration of 3 h or more (n=8), even though the contribution of tourniquet time could not be differentiated from other factors such as injury severity or treatment indication. 67 In another study of 14 limb injuries with a tourniquet duration of 3 h or more, significant morbidity was related to compartment syndrome, and rhabdomyolysis was present in all cases. 71
Building upon TCCC, the US military has recently published additional guidelines to prepare personnel for “what to consider next” after all TCCC interventions have been effectively performed, specifically focusing on situations in which evacuation or mission requirements call for prolonged (hours to days) care in austere settings or during long-distance movements. 72 These “prolonged casualty care” (PCC) guidelines state that on-site tourniquet conversion beyond the 2-h mark (but before 6 h) should still be considered by a trained combat medic if needed. Eventually however, the risks from prolonged tourniquet application may need to be deemed an acceptable tradeoff in a spaceflight emergency scenario, in which the consequences of a major bleeding may well necessitate a judgment call favoring “life over limb.”
Another important factor that has been shown to influence outcomes is correct tourniquet application. 73 -75 It is important that any tourniquet selected for use in the space environment can be used in the right place, at the right time, and with adequate training. Ten different commercial limb tourniquets have met the criteria for approval by the Committee on TCCC (CoTCCC) (Figure 2). 76 They should be placed 2 to 3 inches above the wound and tightened until the distal pulse is absent to prevent compartment syndrome. Depending on the width of the tourniquet used, more than one tourniquet may be needed in bigger limbs. 21 Recently, 2 Combat Application Tourniquets (Gen 7) have been added to the ISS medical kit, and a brief familiarization training on their application has been implemented in the 2-y preflight training period for all crew members. In case a tourniquet is used in-flight, the crew is currently required to contact the ground for further support.

Limb tourniquets recommended by the Committee on Tactical Combat Casualty Care (CoTCCC). 76 ∗RMT Civilian models are not recommended by the CoTCCC for military use; ∗∗Pneumatic tourniquets are considered primarily for tourniquet replacement, conversion, or prolonged application.
Different from bleedings at the extremities, those that are located at junctional regions where the extremities join the torso, such as the groin or the axilla, may be too proximal for limb tourniquet application. 21 Several junctional tourniquets have been developed, and TCCC guidelines suggest the use of such devices if the bleeding site is amenable. 11 However, there is still limited evidence available on their effectiveness and safety,19,77,78 and none is specifically recommended by the CoTCCC. 76 Moreover, they add bulk and weight that limit their use in space.
Hemostatic Agents
When external hemorrhage occurs at sites that are not amenable to tourniquet use, hemostatic dressings are currently recommended in combination with direct pressure.11,19 The current TCCC hemostatic dressing of choice is Combat Gauze (QuickClot). Celox Gauze, ChitoGauze, or XStat can be used as alternatives (Figure 3). 76 Apart from the preference for gauze-type dressings because these are more easily packed into the depths of narrow-tract wounds and do not present ocular hazards in windy environments, 23 powders or granular agents cannot be poured into the wound in microgravity.

Hemostatic agents recommended by the Committee on Tactical Combat Casualty Care. 76 Xstat is best suited for deep, narrow-tract junctional wounds. iTClamp may be used alone or in conjunction with hemostatic dressing or XStat.
While many gaps still remain in high-level evidence on the effectiveness of hemostatic gauzes,19,79 a retrospective review of 3792 military cases showed that the use of Combat Gauze, Celox, or ChitoGauze (n=317) improved survival by an average of 7%. 80 Combat Gauze—which was recently added to the medical pack on the ISS—has been shown to achieve hemostasis in 79 to 89% of penetrating injuries in military studies 81 -83 and 73 to 95% in civilian trauma.59,84,85 However, the function of Combat Gauze depends primarily on blood-clotting activity. 86 Even though successful hemostasis has been reported in coagulopathic models of hypothermia and hemodilution,87,88 this dressing may be less effective in space.54,55 Celox and ChitoGauze are chitosan-based hemostatic dressings that form a mucoadhesive barrier and work independently of the coagulation system. 86 Both have been found to be safe and more effective than Combat Gauze in preclinical studies, with a 10% failure rate to stop or minimize bleeding using ChitoGauze in a civilian setting.22,89 To determine the effectiveness of different hemostatic dressings in space, comparative studies in microgravity conditions are required. If results are similar, the lightest, safest, and most compact choice would be favored. 90
For deep limb or junctional wounds, XStat is preferred. It involves a syringe-like applicator that injects rapidly expanding cellulose-based sponges coated with chitosan, and the first clinical evidence from a civilian setting has shown that in 9 out of 10 penetrating trauma injuries, bleeding completely stopped on initial deployment. 91 Finally, for external hemorrhage of the head and neck, the iTClamp has been recommended as an additive or alternative. This self-locking mechanical clip applies pressure and promotes the generation of a hematoma that can tamponade bleeding and may be useful if wound edges are easily reapproximated. 11 Both XStat and iTClamp may be particularly useful in space as they are small and require minimal training to us, but for both devices, efficacy and safety in prehospital and austere environments—including space—remain to be determined. 64
Tranexamic Acid
Another advancement that has led to increased survival rates on the battlefield is the early administration of tranexamic acid (TXA) for casualties in or at high risk of hemorrhagic shock.11,92 TXA is a lysine derivative that slows down the conversion of plasminogen to plasmin, thereby preventing clot breakdown without inducing clot formation. The US military has included TXA in TCCC and clinical practical guidelines since publication of the CRASH-2 and MATTERs studies about a decade ago, which demonstrated reduced mortality in more than 20,000 civilian and 896 patients with military trauma when TXA was given within 3 h of injury.93,94 In the latter study, TXA was also associated with less coagulopathy. 94 For the greatest survival benefit, TXA should be given as soon as possible after injury 95 but not later than 3 h, as this has actually shown to increase mortality.11,93
So far, no data exist on the use of TXA in space, and despite promising initial results recent evidence suggests that TXA may increase the risk of venous thromboembolism by approximately 3-fold.96,97 As a result, potential overuse in lower-risk trauma patients remains a concern. These observations are particularly relevant for spaceflight, when altered coagulability, higher levels of fibrinogen, endothelial dysfunction, and stagnant blood flow in the upper body already seem to increase the risk of thrombosis in otherwise healthy astronauts. 55 Further investigation into the safety and mechanisms of action of TXA will be necessary to better understand its usability for future space missions, including its application when resuscitation fluids are not available. Storage requirements, the potential impact of radiation on shelf-life stability, and a lack of resources for resupply will also have to be considered.92,98
Advanced Techniques and Future Perspectives
Besides the current TCCC and PCC concepts for extremity and junctional hemorrhage control, more advanced techniques may provide additional solutions for the major resuscitation challenges in space exploration, in particular for injuries of the chest and abdomen that are not amenable to compression. Examples of recent developments include the Abdominal Aortic Junctional Tourniquet (AAJT) for external pressure to the abdomen, injection of self-expanding foam (ResQFoam) or hemostatic hydrogel, resuscitative endovascular balloon occlusion of the aorta (REBOA), wound-closure through nanobridging, and portable blood salvage and autotransfusion technology to recycle spilled blood. 99 -101 Although these techniques require further improvement, their life-saving potential and relative ease of administration in austere environments deserve careful consideration.
With regard to fluid resuscitation, early administration of whole blood has recently been recommended for implementation in TCCC guidelines, and the use of freeze-dried plasma is currently under investigation in special operations forces as well.101,102 These products are particularly suited for use in austere environments, and their role in space exploration has recently been discussed in detail by Nowak and colleagues. 25
Finally, Moon and Mars missions may require even more specialized care and definitive surgical repair when medical evacuation is not possible. 90 To this end, battlefield trauma care in the US military and other North Atlantic Treaty Organization countries has involved forward positioned (Role 2) surgical teams that can provide early damage control resuscitation and surgery as close as possible to the point of injury and without the need for transportation to a more advanced care facility.103,104 In space, such a staged or minimalist surgical approach may allow for temporizing measures if more advanced procedures are beyond the capabilities of the crew medical officer, so that definitive surgical reconstruction can be undertaken with better logistic planning, minimal time pressure, and additional specialty training and consultation from Earth. 90 Although a detailed discussion of advanced resuscitation and surgery procedures is beyond the scope of this review, it is worth mentioning that renewed attention to the optimal utilization and composition of such forward teams by the Committee on Surgical Combat Casualty Care (CoSCCC) could provide valuable lessons for future space missions as well. 105
Training And Medical Support
The capability of any spaceflight medical care system to handle trauma scenarios will ultimately be limited by the capability and training of the crew. Correct tourniquet application, the use of hemostatic agents, pressure dressings, and other basic hemorrhage control techniques—including practice under simulated emergency stress—are essential medical training components for maximizing trauma resuscitation outcomes.73,74 The current training curriculum for providing emergency care in LEO, however, does not cover training in hemorrhage control techniques other than preflight tourniquet familiarization and is designed primarily to prepare a crew medical officer to interact with ground support in a meaningful fashion. 6 On a Mars mission, loss of real-time support means that this training paradigm will be inadequate. 4
Guided by exploration-class mission parameters, additional hands-on training in trauma resuscitation—including early hemorrhage control—will be needed. Similar to TCCC training principles in the military,10,102 this would likely also require all crew members to be involved so that each is independently capable of providing life-saving emergency care. 6 More complex procedures, however, will require more specialized training, and having a broadly trained paramedic or physician on board may greatly enhance mission safety. 106 In a study comparing air medical evacuation outcomes in 671 combat casualties, a higher level of flight medic training was shown to be associated with better survivability and physiological outcomes. 107
Current operations in LEO require all training to be conducted during a 2-y preflight period, 6 and time and opportunities for medical training are usually limited. In combination with prolonged mission durations and constantly evolving scenarios, this means that exploration crews may have to rely on onboard refresher and just-in-time training programs to maintain and expand their skillset. 108 To this end, trauma and surgical manikins have previously been studied in microgravity conditions,38,106 and the European Space Agency (ESA) and National Aeronautics and Space Administration (NASA) are currently investigating onboard training systems based on virtual reality. Such platforms may soon allow for virtual trauma simulations to practice resuscitation principles 109 and could potentially also be used for just-in-time rehearsals of more complex, staged procedures.
Still, it will be unlikely that a crew medical officer will possess the skills to cover all medical conditions and emergency scenarios that may occur. The Autonomous Medical Operations group at NASA and the Space Medicine Team at ESA are putting significant work into the development of an onboard support system, including software and hardware that can assist in medical operations when greater independence from Earth is required. 110 By using systems engineering practices, such a system can integrate complex data and functions from various spacecraft systems into autonomous operations to support crew health and performance. 111 For trauma care, this could include diagnostics and monitoring using machine learning models based on physiological data from advanced monitoring technology. For instance, continuous arterial waveform analysis has shown promising results for early hemorrhage detection. 112 Other examples include medical database management to support clinical decision making and the incorporation of augmented reality for step-by-step procedural guidance. 110
Conclusion
The spaceflight environment poses unique challenges to prehospital trauma care. The limited resources and training, physiological changes due to microgravity exposure, and complicated nature of an emergency evacuation are all changing parameters as missions move farther from Earth. The potential benefits of medical care capabilities focused on the point of injury—versus a return to definitive care—should be carefully weighed for different mission types. Effective early hemorrhage control will be a crucial component of such an approach to preserve cardiovascular reserve, even more so in upcoming exploration-class missions during which an emergency return to Earth is simply not possible. The implementation of basic techniques such as hemostatic dressings and tourniquets will require additional training but could play an important role in delaying the onset of hypovolemic shock. Future research focusing on their efficacy in space is desired. Other techniques—including early TXA administration and devices for junctional or noncompressible wounds—show promise too but will need further characterization first. Looking forward, the ongoing advancement and approaches emerging from the battlefield suggest that tactical and surgical combat casualty care will continue to provide valuable lessons in the years to come and can help to further improve hemorrhage control and trauma care for future space exploration.
Footnotes
Acknowledgments
This work is the result of a library project by ST as part of the Space Physiology and Health MSc at King’s College, London, UK. We would further like to acknowledge Christopher Schubert, medical training lead at the NASA Johnson Space Center, for his insightful comments and input on the manuscript.
Author Contributions: study concept and design (ST, MK); acquisition of data (ST); drafting of manuscript (ST); critical revision of the manuscript (MK); approval of final manuscript (ST, MK).
Financial/Material Support: None.
Disclosures: None.