
Abstract
The National Park Service (NPS) has domestic responsibility for emergency medical services (EMS) in remote and sometimes tactical situations in 417 units covering over 34 million hectares (84 million acres). The crossover between conflicting patient care priorities and complex medical decision making in the tactical, technical, and wilderness/remote environments often has many similarities. Patient care in these diverse locations, when compared with military settings, has slightly different variables but often similar corresponding risks to the patients and providers. The NPS developed a Tactical EMS (TEMS) program that closely integrated many principles from: 1) Tactical Combat Casualty Care (TCCC); 2) Tactical Emergency Casualty Care (TECC); 3) and other established federal and civilian TEMS programs. Combining these best practices into the NPS TEMS Program allowed for standardized training and implementation across not only the NPS, but also paralleled other military/federal/civilian TEMS programs. This synchronization is critical when an injury occurs in a joint tactical operation, either planned (drug interdiction) or unplanned (active shooter response), so that patient care can be uniform and efficient. The components identified for a sustainable TEMS program began with strong medical oversight, protocol development with defined phases of care, identifying specialized equipment, and organized implementation with trained TEMS instructors. Ongoing TEMS program management is continuously improving situationally appropriate training and integrating current best practices as new research, equipment, and tactics are developed. The NPS TEMS Program continues to provide ongoing training to ensure optimal patient care in tactical and other NPS settings.
Keywords
Introduction
The National Park Service (NPS) under the Department of the Interior (DOI), has domestic responsibility for emergency medical services (EMS) in remote and sometimes tactical situations in 417 units covering over 34 million hectares (84 million acres). 1 In 2015 there were 307,247,252 visitors to these NPS units that range from the iconic National Parks (Yellowstone, Yosemite, Grand Canyon) to other NPS units such as the National Mall in Washington DC, as well as national preserves, seashores, and other areas. 1 The park service had its 100-year anniversary in 2016 with record visitation. The NPS Visitor and Resource Protection Division is responsible for: 1) protecting parks from people; 2) protecting people from the parks; and 3) protecting people from people. Many of these duties require NPS rangers to be cross trained across many areas from law enforcement, to EMS, to search and rescue (SAR), to wildland and structural firefighting. 2 The NPS averages 10,000–15,000 EMS calls per year and many of these have remote and prolonged care settings.3,4 Based on this combination of unique environments and sometimes tactical settings, many of the issues the warfighter has faced in Iraq and Afghanistan in the recent decades have direct relevance when applied to the NPS mission space.
The operational environment of the NPS is unique as it crosses over between tactical, technical, and wilderness/remote situations on a regular frequency. Although a tactical situation can develop anywhere, some environments in the NPS have an elevated likelihood that they could have a tactical situation occur. Examples of some conceivable tactical environments are NPS units on the United States (US) / Mexico border where the DOI (including NPS) manages 1287 km (800 miles) of border (see Figure 1) or other settings such as the National Mall in Washington, DC. More often the NPS is known for its beauty and with this sometimes comes technical rescue, such as rescuing a big wall climber off El Capitan in Yosemite (see Figure 2). Other technical environments such as caves, underwater diving, avalanches, and swiftwater settings provide unique specific challenges. Remote/Wilderness settings such as large National Parks in Alaska (see Figure 3), or even locations in the continental United States can sometimes have delayed patient access and extractions lasting hours or sometimes days before patients can reach definitive medical care. Weather and other factors such as helicopter availability and limited communication can lead to even further prolonged field care and delayed rescue.

National Park Service ranger on patrol at the US / Mexico border, a potentially tactical environment. Photograph credit: Will Smith.

Technical rescue in Yosemite National Park. Photograph credit:

A National Park Service Wilderness/Remote setting in Wrangell-St. Elias National Park and Preserve in Alaska. This park rises from the ocean to Mt. St. Elias at 5732 meters (18,808 feet) and occupies 5.3 million hectares (13.2 million acres, which is the same size as Yellowstone, Yosemite, and Switzerland combined). Photograph credit: Wrangell-St. Elias National Park and Preserve (public domain). Available at:
Providing patient care in these wide-ranging NPS venues has challenging variables that often make traditional EMS care difficult. The NPS recognized this need for specialized prehospital medical training with its Parkmedic training program in the 1970s. 5 The Parkmedic program allows for an expanded scope of practice (ie, reduction of dislocations, antibiotic use, etc.) with additional focused training for medical decision making requirements in technical and wilderness/remote settings. The first formal NPS EMS course was taught in 1972 and the first Parkmedic training was in 1978. 6 The specialized course continues to be taught every other January by the University of California San Francisco–Fresno emergency medicine faculty and residents. This program over the past nearly 40 years has been one example of the NPS adapting EMS response to the unique mission requirements in the NPS.7,8
It has been recognized that patient care priorities can vary with the risk of the environment, whether it is tactical, technical, or wilderness/remote. With this recognition, it was clear that a special TEMS program with adapted training, protocols with defined phases of care, and specialized equipment was needed. This complex setting, as with other ongoing NPS EMS programs, require continued close medical oversight with experience in these specialty areas. 9 The National Association of EMS Physicians (NAEMSP) and National Association of State EMS Officials (NASEMSO) have also made this clear recognition of the importance of strong medical oversight in their position statement. 10 This continued recognition and the growing awareness of the benefit of the military tactical combat casualty care (TCCC)11,12 and other TEMS programs with improved survival of those injured in tactical settings, led the NPS to begin developing a formal tactical EMS program.
Although there are tactical skills such as needle decompression taught in the Parkmedic course, they are generally reserved for the traditional advanced life support (ALS) providers. The Parkmedic level of certification is generally considered to be between the advanced emergency medical technician (AEMT) and paramedic level of care. 13 However, other formal EMS certifications are also recognized and commonly practiced throughout the NPS as outlined in The 2005 National EMS Scope of Practice Model. 14 NPS rangers responsible for visitor and resource protection, regardless of their EMS skill level, are at increased risk of tactical injuries by the fact that many are also federal law enforcement officers. With the knowledge that all levels of providers would benefit from this TEMS program, as recognized from the Department of Defense (DoD) conflicts in Iraq and Afghanistan, it was felt that the NPS TEMS program should be taught at all EMS levels, as well as to non-EMS law enforcement rangers in some approved settings.
The recent advances in TCCC focus on the core principles of avoiding preventable deaths and to combine good medicine with good tactics.11,15 The conflicts in Afghanistan (Operation Enduring Freedom – OEF) and Iraq (Operation Iraqi Freedom – OIF) have shown some of the lowest case fatality rates of any modern conflict. 16 This is thought to be from a multifactorial approach from improved personal protective equipment, widespread TCCC implementation, faster evacuation times, and better trained medics. 16 A focus on the potentially preventable deaths on the battlefield helped drive TCCC to provide the biggest benefit. These preventable deaths were identified early in OIF/OEF to be extremity hemorrhage, tension pneumothorax, and airway compromise. 17 Eastridge and colleagues confirmed that the same potentially preventable deaths continued to be consistent in the ongoing OIF/OEF conflict, thus confirming the correct focus of TCCC and early point of injury battlefield care. 18 Kotwal and others showed that aggressive and formalized TCCC training to service members actually saved lives. 19
TECC around 2011 began as an adaptation from TCCC in the federal/civilian sectors that applied similar TCCC concepts across multiple all risk areas (tactical, hazmat, etc.) and to a slightly expanded patient population. 20 Patients generally treated with TCCC in combat settings were young and healthy. When a federal/civilian tactical event occurs, the demographics are much more diverse. There are potentially children and elderly, patients with multiple medications that could be blood thinners, as well as other issues such as federal/civilian legal constraints. Many departments providing TECC care in the United States have now adapted this into formalized rescue task force (RTF) programs.
The RTF concept applies the TECC protocols in an integrated overall operational group during a larger event. Some of the initial forward thinkers in this area were from Arlington County, Virginia. They documented their experience in an exemplary article in the
Phases of care in TCCC and TECC have shown that timing of medical care is everything. This concept continues to reinforce that patient care priorities do transition during a tactical situation. Table 1 describes the identified phases of care established in the TCCC/TECC guidelines.20,23
The right equipment for enacting TCCC, TECC, and other TEMS programs also clearly showed a positive effect in saving lives. 24 With the identification of the reversible life threats, individual first aid kits (IFAKs) became commonplace with the equipment needed to save lives, including supplies such as tourniquets, bandages, hemostatic agents, etc. These kits became standard issue for all deploying soldiers. Civilian law enforcement agencies now also issue IFAKs in many areas of the country. Pima County, AZ credited several lives saved to TCCC training and universal deployment of IFAKs used during the Gabby Gifford shooting in 2011.25,26 As these kits have been developed and deployed, training and medical tactics have also changed. Tourniquets have become recognized as the first step to controlling severe bleeding, instead of the last. Nasal pharyngeal airways (NPA) are issued to help treat airway compromise. Medical treatments for tension pneumothorax with needle decompression and chest seals for open chest wounds also benefit patient care, and are generally standard issues in most IFAKs.
As noted, the crossover between the tactical, technical, and wilderness/remote environments have many similarities. The complex medical decision making in each of these settings can be applied to not only active shooter/mass violence events, but can also be used in hazardous materials response and other high risk situations. Protocol development with phases of care and organized implementation are key in keeping providers safe while more efficiently taking care of patients in these many diverse settings. Best practices in these areas with blending of field research and focused training to sometimes nontypical EMS providers can be lifesaving. 27 The NPS moved to develop a TEMS program that applies many of the TCCC and TECC principles in a like fashion, as well as mirroring other established federal and civilian TEMS programs. Integrating these common best practices into the NPS TEMS program allowed for standardized training and implementation across not only the NPS, but also paralleled other military/federal/civilian TEMS programs. This synchronization is critical when an injury occurs in a joint tactical operation, either planned such as a drug interdiction, or unplanned such as an active shooter event, so that patient care can be uniform and efficient. The NPS has been able to use the lessons learned and best practices by standardizing training so when joint operations are occurring between federal and DoD assets, patient care can be consistent and efficient.
Development
In 2009 it was formally recognized that the conflicts in Iraq and Afghanistan were leading to life saving TCCC guidelines and that the NPS needed to incorporate many of these lessons learned into a formal program that benefited all that encountered the NPS jurisdictions. A group of NPS subject matter experts was appointed by the NPS EMS Advisory Committee to develop a NPS TEMS Program. This group consisted of current and former military members, current NPS park rangers, EMS professionals, and faculty from academic institutions. The components identified for a sustainable TEMS program began with strong medical oversight, protocol development with defined phase of care, specialized equipment, and organized implementation with trained TEMS instructors. The best practices of TCCC and TECC, as well as other established TEMS programs, were reviewed and adapted to create the NPS TEMS Protocols and Procedures Manual, Field Manual (FM)-51 Tactical (T). This document serves as a special addendum to the already well established Field Manual 51 (FM 51), which provides the standard NPS EMS protocols and procedures.
Care guidelines were adapted from the standard NPS protocols and procedures to emphasize bleeding control with the acronym XABC (eXsanguination, Airway, Breathing, and Circulation), focusing on the important principles of TCCC/TECC. Other components of the RTF and escorted warm zone care are also introduced. Casualty collection points (CCPs) are discussed as a concept to help optimize care at focused locations by TEMS providers.
FM-51T also clearly recognizes the stages of care and treatment priorities. The precedence is to perform the
IFAKs are issued to each law enforcement officer and other additional EMS response units. Some IFAKs were purchased prepackaged commercial off the shelf (COTS) from various commercial vendors, while some NPS units chose to individually procure the items for a cheaper cost, but with equivalent equipment. Figure 4 shows an example of a NPS TEMS kit packing list, with associated costs from 2011. Early on, training and education ensured that teams were removing granular clay agents from kits based on the Army Institute of Surgical Research findings of the harm caused. 28 This paralleled the TCCC recommendations to remove the same agents from the military IFAKs.
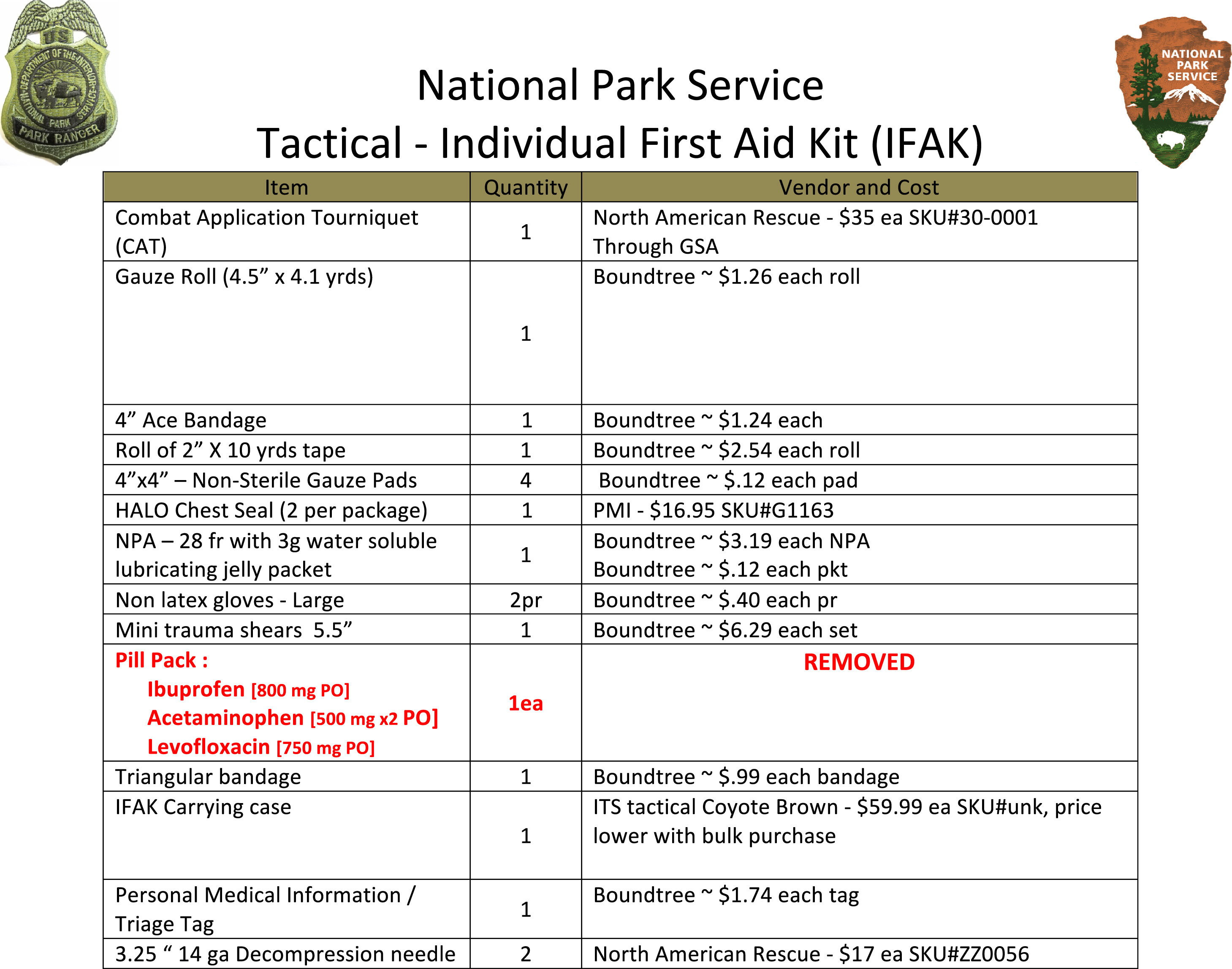
Example of a National Park Service individual first aid kit (IFAK) packing list. Total cost per IFAK is approximately $130.
Pill packs (now called combat wound medication packs [CWMP] by TCCC) were initially included in the program with acetaminophen (Tylenol) 1 g, ibuprofen (Advil, Motrin) 800 mg, and levofloxacin (Levaquin) 750 mg. Alternative antibiotics of azithromycin (Zithromax) 500 mg plus metronidazole (Flagyl) 1 g were selected for substitution for individuals with fluoroquinolone allergy or intolerance. The pill pack was to be taken orally for pain and/or penetrating injury or other open wound.
The entire NPS TEMS training module was designed to be completed every 2 years, and take approximately 4 hours. This includes a 1 hour standardized presentation and 3 skills sessions, taking 1 hour each. To maintain skills retention, skills reviews are incorporated every 6 months with other EMS or law enforcement training. The 3 skills stations were: 1) bleeding control (tourniquet use, wound packing, pressure dressings); 2) penetrating chest trauma, (needle decompression [NDC], chest seals); 3) IFAK check and protocol review. See Table 2 for a further description of each skill station. A standardized evaluation sheet for each skill station identifies the critical learning objectives that need to be mastered. A brief written test is administered initially and then at the end of each 2-year training module to also verify comprehension of the training.
NPS TEMS skills stations
NPS, National Park Service; TEMS, tactical emergency medical services; CAT, combat application tourniquet; EMS, emergency medical services, IFAK individual first aid kit; EMR, emergency medical responder; EMT, emergency medical technician; ALS, advanced life support.
Each participant will demonstrate understanding and skill performance based on Station Evaluation Sheet, included with this NPS TEMS Module.
There are identified BLS and ALS levels of NPS TEMS responders. All TEMS programs require local EMS medical advisor (LEMA) approval and have a local TEMS coordinator.
Basic Life Support (BLS) LE Ranger (no formal EMS Certification) EMR (Emergency Medical Responder) EMT (Emergency Medical Technician)
Advanced Life Support (ALS) AEMT Parkmedic Paramedic Advanced Provider (nurse, nurse practitioner, physician assistant, physician)
Implementation
Once the NPS TEMS program was developed and approved by the NPS EMS Advisory Committee, it was implemented across the NPS. A core group of instructors were trained at a meeting in Tulsa, OK in March 2011. Since this event, the training has continued throughout the NPS with over 30 NPS TEMS instructors. Ongoing updates to the program have kept pace with the Committee on TCCC and Co-TECC recommendations. The TEMS instructors are also encouraged to integrate more complex scenarios after the initial training to better approximate real world situations. These have included simunition as well as moulage. There have been integrated interagency trainings with partner units to unify treatment and response for actual future TEMS situations.
During continued evaluation of the NPS TEMS program, the pill pack was removed after nonuse and logistical challenges. There were also discussions regarding the concerns with contents of the pill pack, specifically with ibuprofen causing platelet inhibition as well as fluoroquinolones with tendon and other soft tissue issues.
It was recognized that some small but relevant deviations were made from the TCCC guidelines, but these were felt to be justified in the NPS operational environment. However, to the greatest extent possible, the core tenants of TCCC, TECC, and other federal/civilian TEMS programs were maintained to allow deployed interoperability for uniform and efficient patient care. Schwartz et al have also looked at competency based TEMS guidelines for uniformity in the TEMS community. 29
Additional expansions in the NPS TEMS program, as well as to the general NPS protocols, have mirrored many of the TCCC evolving recommendations. These have included ketamine for both subdissociative pain dosing as well as sedation dosing for procedures such as cardioversion and also chemical restraint for excited delirium/behavioral emergencies. The NPS has also added prehospital administration of tranexamic acid for serious hemorrhage. Conversion guidelines for extended tourniquet use have also been developed for prolonged field care situations.
Conclusion
The National Park Service’s diversity in land and sea creates similar tactical, technical, and wilderness/remote missions similar to those encountered by the warfighter. With these similarities, it is paramount that a Tactical EMS program would closely mirror the TCCC lessons learned from the military and adapt them to a slightly different environment while still maintaining the best practices. The NPS TEMS program continues to provide ongoing training to ensure optimal patient care in tactical and other NPS settings.
Acknowledgments: NPS Tactical EMS Sub-Committee members (Dean Ross, Jay Shields, Clay Anderson, Geoff Stroh, Mark Jacoby, and Will Smith), NPS EMS Advisory Committee, and all the NPS employees that keep our National Parks and other units safe for all to enjoy.
Financial/Material Support: None
Disclosures: None
Footnotes
☆
Presented at the Tactical Combat Casualty Care: Transitioning Battlefield Lessons Learned to Other Austere Environments Preconference to the Seventh World Congress of Mountain & Wilderness Medicine, Telluride, CO, July 30–31, 2016.