
Abstract
Introduction
Most of the literature on sailing injuries is centered on competitive sailing, often involving a single regatta. The aims of this study were to provide a description of the types of injuries and illnesses sustained during amateur offshore cruising events, estimate their incidence, and investigate potential risk factors for injuries.
Methods
We conducted a cross-sectional survey of self-reported sailing-related injuries and health issues during 4 different events organized by the World Cruising Club between 2014 and 2015. Prior to departure, sailors received an injury or health issue report form to complete during their sailing event. Questionnaires were then collected at the end of each event. Bivariable (Student’s t tests and χ2 tests) and mutilvariable logistic regression were used to study the associations among injuries, health issues, and the characteristics of sailors or sailboats.
Results
The incidence of injuries and health issues among the respondents was 1.08 and 1.01 per 10,000 nautical miles, respectively. Smaller boats (
Conclusions
Injuries and health issues are relatively common among amateur offshore recreational sailors, but severe injuries are rare. Smaller boats and having less experience in sailing with the current boat were associated with more injuries. Preventive strategies should include a sailing experience requirement on the boat being sailed for all crew members, increasing the minimum boat size requirement for sailing events, and mandatory first-aid training prior to a cruising event for all crew members.
Introduction
It has been documented that sailing as a recreational activity began gaining popularity in Holland ∼400 y ago, and sailboat racing was first formalized in England in 1851.1,2 Modern sailing encompasses a wide variety of water crafts and involves many different activities. At one end of the spectrum are small dinghies, suited for one person, which rely on crew weight for stability and are sailed recreationally for just a few hours on protected waters. At the other end are much larger sailboats, which rely on a ballasted keel for stability and are raced around the world 24 h/d for weeks by professional crews, with the goal of maximizing boat speed and winning. Recreational sailing or “cruising” on sleep-aboard keel boats differs from the latter because it is not a matter of winning but rather a matter of enjoyment. Recreational sailing on sleep-aboard keel boats from harbor to harbor in sight of land is commonly referred to as “coastal” cruising, whereas cruising across oceans is referred to as “offshore” cruising. Cruising differs significantly from competitive sailing because both involve different objectives. Competitive sailers, often backed by sponsors, sail very-high-performance boats while pushing almost all limits to try to be as fast as possible in order to win. These limits include human physical limits, technological limits, and sailing their boats in dangerous weather patterns seeking higher winds. Cruisers usually attempt to sail around storms in order to minimize risks to both the boat and crew. To our knowledge, the incidence of and risk factors for injuries and illnesses have not yet been reported in the context of recreational offshore cruising.
Participation in offshore cruising has increased significantly in recent years,3,4 especially since the creation of the first transatlantic sailing Atlantic Rally for Cruisers (ARC) in 1986. The World Cruising Club (WCC) has defined a sailing rally “as safe and social cruising while offering an element of fun competition, but not a race. Rallies are about crossing oceans with friends; feeling confident and prepared on departure day; having support and friendship at sea; and providing a welcome to salute your achievement on arrival.” 5 In the ARC event alone, >200 boats and 1200 people are estimated to sail an average of 2700 nautical miles (NMs) each year.4,6 The ocean passages (or legs) in ARC rallies vary in length from 800 to 2700 NMs. Sailing rallies are planned in such a way as to avoid the hurricane and winter-storm seasons in the North Atlantic and regions of piracy in order to minimize risks to participants. They attract a wide range of participants, 7 including professional and recreational sailors, retirees, and even families with small children. 8 It is also of interest to note that a recent study, using cost-benefit analysis and net present value indicators, identified sailing and cruising as being potentially one of the fastest growing and most profitable sectors of activity in the tourism industry. 9
Medical care for injury or illness aboard a sailboat presents some unique challenges, particularly when offshore. Definitive medical attention is often many days away, supplies are limited, space below deck is cramped, and the motion of the vessel can be jarring and unpredictable. Evacuation at sea is often dangerous and may not always be possible. Compounding these challenges is the possibility that injuries may occur at night and during stormy weather when crew members are fully engaged in sailing the boat and may also be fatigued or seasick. Numerous studies have found that high wind speeds increase the risk of injury among sailors.8,10-13
Only 1 published study, by Rouvillain et al, 14 attempted to describe the injuries associated with sailing in the cruising population. Their results suggest that most of the injuries reported could have been prevented if a few simple recommendations had been implemented (wearing shoes, using a hatch cover, a bimini top, a windlass, and adequate wound care). Most of the literature available on sailing injuries comes from professional or competitive sailing.10,13,15-18 In a prospective study conducted during the 2003 America’s Cup race, the incidence of injuries was estimated to be 2.2 per 1000 sailing hours. 16 Fewer serious injuries but a higher proportion of minor injuries (eg, abrasions and contusions) were reported during an amateur around-the-world yacht race (BT Global Challenge). 17 Comparable studies involving large sailboats have shown that the most frequent areas affected by injuries are the upper limbs (22%–40%), lower limbs (17%–38%), and back and trunk (11%–21%).12,16,17 Dermatologic conditions, such as cracked skin, skin sores, and fungal rashes, were the most common illnesses reported during the Whitbread Round the World Yacht Race from 1997 to 1998. 18 In a 2016 analysis of US Coast Guard data, a fatality rate of 1.19 deaths per million sailing person days was estimated on sailboats in US waters. 19
To our knowledge, the incidence of and risk factors for injuries and illness have not yet been reported in the context of recreational offshore cruising. A detailed understanding of the types of injuries or illnesses, their frequency, and their associated risk factors would be of great value to the cruising community. This knowledge would help optimize preparation, potentially reducing the likelihood of injuries or health issues. In order to improve risk assessments and help educate the sailing community, we pursued 3 specific objectives for this study. The aims of this study were as follows: 1) to provide a description of the types of injuries and illnesses sustained during amateur offshore sailing events for cruisers, 2) to estimate their incidence, and 3) to investigate potential risk factors for injuries.
Methods
Research Design
We used a cross-sectional survey design of self-reported sailing-specific injuries and health issues. The survey questionnaire was adapted from a previously published sailing injury report form. 20 The revised questionnaire (see online Supplemental Material S1) included questions such as the sailor’s sex, age, sailing experience, sailing credentials, and first-aid training. It also included questions about the sailboat, such as the type of boat and number of crew members onboard. Sailors who sustained an injury were asked additional questions, such as the nature of the injury, part of body, severity, and context or cause of the injury. All participants were also asked if they had suffered other health issues while sailing such as motion sickness, sunburn, anxiety, insomnia, earache, skin rash or infection, conjunctivitis, headaches, toothache, diarrhea, food or water poisoning, or other.
We recruited recreational sailors during 4 different sailing rallies organized by the WCC during the years 2014 to 2015 (Figure 1). The sailing rallies were composed of 1 to 3 separate sailing passages of various lengths ranging from 800 to 2700 NMs. Each passage was expected to take an average of 6 to 21 d to complete. Because this study specifically targeted recreational sailors, crews from boats registered in a competitive race class were excluded. Boats that did not start (DNS; n=7), had retired (RTD; n=9), or did not finish (DNF; n=6) were also excluded.
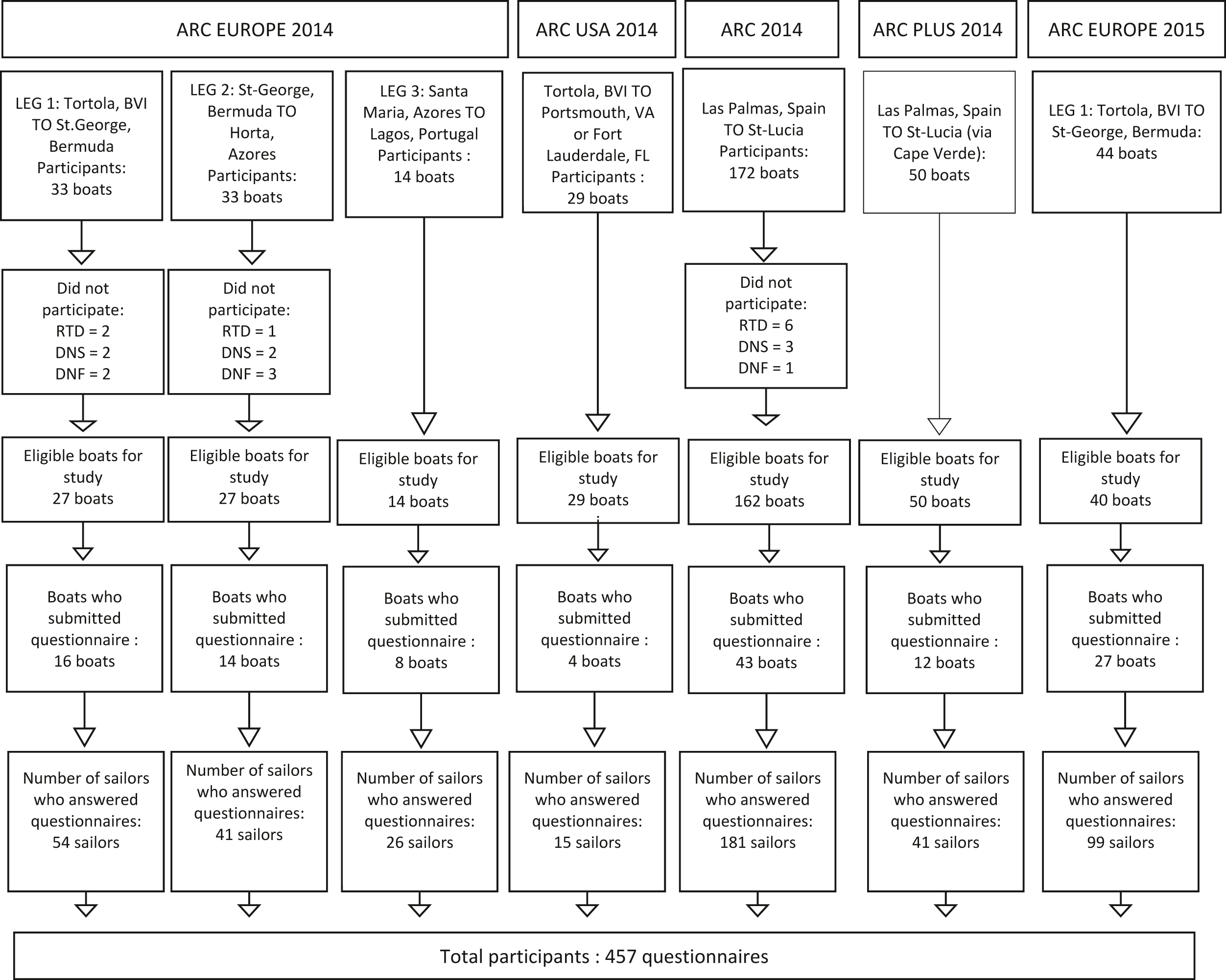
Flowchart of the study participants. ARC, Atlantic Rally for Cruisers; BVI, British Virgin Islands; DNF, did not finish; DNS, did not start; FL, Florida; RTD, retired; VA, Virginia.
Data Collection
The distribution of the paper questionnaire was done by the principal investigator (DOH) during the skippers’ predeparture briefings held before each sailing passage. Each crew member from eligible boats received a paper copy of the questionnaire with a consent form and was instructed to record each injury or illness on the form promptly in order to minimize recall bias. Sailors who participated in multiple events had the opportunity to complete >1 form. In the absence of injury or illness during a passage, only sections A (sailor or sailboat general information) and G (consent) required completion. Sailors were reminded to return their completed questionnaires at the end of each passage. The forms were then collected by the principal investigator or WCC staff for future data analysis.
Description of the Study Variables
The main dependent variables were as follows: 1) the report of an injury and 2) the report of another health issue. The type of training or accreditation reported for sailing and first-aid credentials was converted into categorical variables using a matrix based on the duration of training (see online Supplemental Materials S2 and S3). The characteristics of sailors and sailboats were the independent variables. Because the characteristics of injuries and/or health issues were reported only in their presence, they were treated as descriptive variables.
Data Analysis
Descriptive statistics were produced for all variables (frequencies and proportions). Continuous variables were divided into meaningful categories for descriptive purposes. Bivariable analyses, such as the Student’s t test and χ2 test, were conducted between the independent and dependent variables. Student’s t tests and χ2 tests were also used to describe the associations among sex, health issues, and characteristics of sailors or sailboats. Multiple logistic regression models were developed to identify the most significant predictors of injury and health issues among the characteristics of sailors or sailboats. All characteristic variables with
Ethical Considerations
This research project received ethical approval from the Ethics Review Board of Université du Québec à Trois-Rivières (CER-14-201-10.01). Participation was voluntary, and each respondent provided written consent.
Results
Three hundred seventy-five boats departed for 7 different offshore passages. Excluded from the study were boats in racing categories, leaving a total of 349 eligible boats, of which 9 RTD, 7 DNS, and 6 DNF. Four hundred fifty-seven questionnaires were collected from sailors from 124 different eligible boats, representing 35.5% of all eligible boats that participated in the different passages (Figure 1). Two participants completed 4 different questionnaires, 20 completed 3 questionnaires, 24 completed 2 questionnaires, and 341 completed 1 questionnaire. The incidence of injuries among the respondents was 1.08 per 10,000 NMs, and the incidence of health issues was 1.01 per 10,000 NMs.
Table 1 presents the descriptive statistics of the participants by sex. Women were significantly younger than men (
Sailboats’ characteristics and sailors’ characteristics by sex
aSome sailors might have completed >1 questionnaire.
Table 2 presents the bivariable association between the characteristics of sailors, boats, and crew and the occurrence of injuries or health issues. Ninety sailors reported an injury (cumulative incidence of 0.20 per person per passage), and 65 sailors reported 84 health issues (cumulative incidence of 0.18 per person per passage). Twenty sailors reported both a health issue and an injury. Sailors who had sailed fewer miles on a particular boat and those on smaller boats were at a higher risk of injury (
Associations between the sailboats’ or sailors’ characteristics and the occurrence of injuries or health issues
P value <0.05
Table 3 presents the results of the bivariable and multivariable logistic regression for the association between the characteristics of sailors, boats, and crew and the occurrence of injuries or health issues. Among these characteristics, boat length was the most significant predictor of injuries (odds ratio [OR], 0.87 [0.82–0.93]) in the multivariable model. Boat length (OR, 0.91 [0.86–0.96]) and sex (OR for women, 2.53 [1.42–4.51]) were the most significant predictors of health issues.
Bivariable and multivariable logistic regression between the sailboats’ or sailors’ characteristics and the occurrence of injuries or health issues
OR, odds ratio.
Table 4 presents further description of the injuries reported related to weather conditions/sea state, position of the crew on the boat, and points of sail. It also describes injury-specific details such as type of injury, anatomic location, mechanism, and severity of injury. Contusions (27%), lacerations (19%), and burns (sunburn, rope burn, and scalding injuries) (14%) were most common, and the upper extremities (22%), head/face (19%), and hand (19%) were most commonly injured. The majority of injuries occurred below decks (38%) or on decks (excluding the cockpit) (30%) and were caused by slipping/falling (24%) or impact of the boom or with hardware (20%). Very few of the injuries were severe (1%), and only 8% of those injured planned on seeking medical care ashore.
Description of the injury
Table 5 represents health issues reported by sex. Female sailors reported twice as many health issues as their male counterparts (
Health issue by sex
Statistically significant.
Discussion
Again, to our knowledge, this is the first study to examine injuries and illnesses in amateur sailors participating in recreational offshore sailing events. Data regarding the mechanisms of injuries, types of injuries, and incidence of injuries should prove valuable for cruising sailors preparing for offshore passages and sailing organizations hosting offshore sailing events.
Significant Findings
The incidence of injuries among the respondents was 1.08 per 10,000 NMs. Otherwise stated, a crew of 6 was likely to experience ∼1.75 injuries per transatlantic passage (∼2700 NMs). The majority of reported injuries were classified as slight or minor (79%), with <8% seeking medical care on arrival at the port. Only 1% of injuries were classified as severe, and there were no medical evacuations during the 7 ocean passages included in the study.
We found that contusions and hematoma were the most prevalent types of injury, with the incidence at 27%. Lacerations, burns (photo-induced or thermal), and abrasions accounted for 19%, 13%, and 11% of all injuries, respectively. The upper extremities (22%), hand/fingers (19%), and head/face (19%) accounted for the majority of injuries. These findings are similar to sailing injuries reported in previous studies.8,16,17,20 Most injuries occurred during the day (59%) in dry weather (74%) and with seas of <10 ft (75%) and at wind speeds of <20 knots (66%). Although other studies have shown that high wind speeds and rough seas are risk factors for sailing injuries and fatalities,8,11,15,19 it is likely that most injuries in our study occurred in fair weather because the vast majority of the sailing in our study was done in favorable weather. The routes selected by the WCC are expressly chosen to favor good weather. Cruising sailors, unlike racing sailors, steer around storm systems when possible.
An important finding was that boat length had a negative association with the incidence of both injuries and health issues. To our knowledge, this finding has not been reported in the medical literature. The presence of fewer crew members also had a negative association with the occurrence of injuries in the bivariable analysis. However, smaller boats are usually sailed by fewer crew members, and when both factors were considered simultaneously, only shorter boat length was significantly associated with fewer reported injuries.
Fewer total number of miles sailed on a particular vessel was also significantly associated with a higher risk of injury, whereas offshore sailing experience and level of sailing credentials were not. Different sailboats have different configurations of lines, winches, sails, hatches, and deck layouts. They may also have different systems for steering, reefing (reducing sail size), and navigation. As such, lack of familiarity with the operation of a specific sailboat is likely to lead to more errors and resultant injuries, particularly while performing complex maneuvers such as sail changes, reefing, or tacking.
Somewhat surprising was that more than half of injuries were reported while the sailors were either below decks (37.8%) or off watch (20%). Spalding et al 18 also found that one third of injuries in the Volvo Ocean Race occurred below decks. This is likely because without the visual cues of oncoming waves or sudden maneuvers on the deck, the movement of the boat is less predictable, potentially leading to falls and injuries below deck.
The most common nontraumatic medical issues reported were sea sickness, sunburn, rashes, and insomnia. Women were equally likely to be injured but twice as likely to report illnesses than men, primarily because of a higher incidence of sea sickness, anxiety, and skin rash/fungal infection. Less experience at sea and female sex have been widely reported to be risk factors for sea sickness,21,22 and women in this study reported less sailing experience than men. Although the gender difference in the report of skin rash/fungal infection was statistically significant, the absolute difference appears to be minimal (0.6% for men vs 3.6% for women). Readers should keep in mind that there is a possibility that the gender differences observed for the incidence of health issues might have been related to differential reporting. 23
Finally, ∼40% of the respondents had no first-aid training prior to departure. This is a source of concern given the nature of offshore sailing but could be easily corrected if the cruising organization required this type of training prior to departure. Although it is currently unknown whether first-aid training influences the perception of risk and, therefore, the incidence of injuries, this training would help provide knowledge for the management of frequent and diverse injuries and lead to proper interventions that would most likely contribute to the mitigation of risks of a relatively simple injury or health issue evolving into a more serious one.
Implications
Sailors should be aware that larger boats appear to be safer while making offshore passages and are associated with fewer injuries and health issues. In general, larger boats are more stable and experience less pounding (boat slamming up and down while passing waves) in heavy seas. They also have more freeboard (distance from deck to waterline), higher boom clearance to prevent head collision with the boom or hardware, and more interpersonal space below decks. These factors make falls and the impact of the boom less likely. The risks of sea sickness and infectious diseases are likely mitigated by more stable vessels and more distance among crew members, respectively.
Among all experience-related variables that we studied, our results suggest that gaining experience with the boat that will be used for an offshore ocean passage is the most important in reducing the risk of injury. One quarter of our respondents had minimal experience (<500 NMs) with their boat. Although some rally organizers require that every captain should have sailed their boat on a previous offshore passage of a minimum of 500 NMs, extending that requirement to the rest of the crew could be considered to prevent injuries.
Albeit the vast majority of injuries were not threats to life or limb, they were very diverse, varying from lacerations and contusions to seasickness and anxiety. Sailors should have adequate training and medical kits to face those eventualities. Of concern to the authors is that 40% of the respondents did not have proper first-aid training. Sailing organizations might contribute to the prevention of injuries through training opportunities and require formal first-aid training for all sailors. Sailing rally organizations should consider increasing their minimal boat size requirement and promote the use of larger boats.
Future research efforts in this field should attempt to assess the validity and reliability of the questionnaire proposed by Neville and Folland. 20 Although we were able to recruit many participants, future studies should dedicate more resources to survey distribution and data collection to increase the response rate. Great attention should also be given to identification of the population at risk.
Limitations
We estimated the response rate by calculating the percentage of boats for which we received at least 1 questionnaire. After receiving questionnaires from 35.5% of boats, we cannot rule out the possibility of selection bias because it is possible that nonrespondents might have presented different profiles of injury and illness compared with those of the respondents. Our data collection used an adapted version of the questionnaire developed by Neville and Folland 20 on the epidemiology and etiology of sailing injuries. However, this questionnaire has not been validated, and its psychometric proprieties are unknown. Consequently, there is a possibility of information bias. Hence, based on a previous similar study design, it is conceivable that the reported injuries and/or health issues in this study were either underreported or overreported. Additionally, because the RTD, DNS, and DNF boats were excluded as a result of of the impossibility of collection of data and that some might have retired because of illness or injury, it is possible that we might have underestimated the rates of injuries and health issues. Finally, the method we used to categorize first-aid training by duration has not been validated. Therefore, it is unknown if it is an appropriate measurement of medical preparedness, particularly in a wilderness setting.
Conclusion
Injuries and health issues are relatively common among amateur offshore recreational sailors, but severe injuries are rare. Smaller boats and less experience with the current boat were associated with more injuries. Preventive strategies should include an experience requirement and mandatory first-aid training as a prerequisite for participation in cruising rallies.
Footnotes
Acknowledgments
The authors wish to thank the World Cruising Club for its help and support in data collection while conducting this research.
Author Contributions: study concept and design (DOH); acquisition of the data (DOH); analysis of the data (DOH, ED, M-AB, ATN); drafting of the manuscript (DOH, ED, M-AB, ATN); critical revision of the manuscript (DOH, ED, M-AB, ATN); approval of the final manuscript (DOH, ED, M-AB, ATN).
Financial/Material Support: DOH received an in-kind contribution from Université du Québec à Trois-Rivières to participate in the research project. Otherwise, the authors DOH, ATN, ED, M-AB received no specific funding for this work. M-AB reports research grants unrelated to this work from the University of Quebec-Trois-Rivieres and fees from medical-legal expertise from the Canadian Chiropractic Protective Association and Intact Assurance. ED reports research grants unrelated to this work from Fondation chiropratique du Québec. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosures: None.
Supplemental Material(s)
Supplementary material associated with this article can be found in the online version at
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.