
Abstract
Introduction
Point-of-care ultrasound (POCUS) is utilized in austere environments because it is lightweight, durable, battery powered, and portable. In austere settings, weight and space constraints are limitations to carrying dedicated ultrasound gel. Few studies have assessed commonly carried liquids as gel alternatives. The study objective was to assess the suitability of common food and personal care products as ultrasound coupling agents compared with that of commercial gel.
Methods
A noninferiority study compared 9 products to commercial gel. Each substance was independently tested on 2 subjects by 2 sonographers covering 8 standardized ultrasound windows. Clips were recorded, blinded, and independently graded by 2 ultrasound fellowship-trained physicians on the ability to make clinical decisions and technical details, including contrast, resolution, and artifact. A 20% noninferiority margin was set, which correlates to levels considered to be of reliably sufficient quality by American College of Emergency Physicians’ guidelines. The substances included water, soap, shampoo, olive oil, energy gel, maple syrup, hand sanitizer, sunscreen, and lotion.
Results
A total of 300 of 318 (94%) clips met the primary endpoint of adequacy to make a clinical decision. All media, except sunscreen, were noninferior to commercial gel in the ability to make a clinical decision (α=0.05). In terms of secondary outcomes, resolution, artifact, and contrast, all substances were noninferior to commercial gel (α=0.05). The sonographers concluded that all gel alternatives’ usability performed similarly to commercial gel, with the exception of energy gel.
Conclusions
Of the 9 substances tested, 8 were noninferior to commercial gels for clinical decisions. Our study indicates that several POCUS gel substitutes are serviceable to produce clinically adequate images.
Keywords
Introduction
Point-of-care ultrasound (POCUS) has emerged as an imaging modality of choice in austere and low-resource environments because it is lightweight, durable, battery powered, and portable. 1 Handheld ultrasound units are particularly useful for remote clinics or backcountry settings, where specialty resources and advanced imaging are not available. 2 In recent years, several handheld ultrasound models have been introduced to the market that connect directly or wirelessly to users’ phones or tablets. These devices are more portable than laptops or cart-based units currently in widespread use. Their existence has led to increased availability of ultrasound in austere and wilderness settings, in which all equipment is carried by participants. Out-of-hospital, portable ultrasound has been used in rural or high-altitude clinics, tactical environments, and natural disasters. 1 The use of portable ultrasound is quickly expanding to wilderness settings, including smaller expeditions, wilderness rescue, and even personal recreational activities.
Ultrasound requires a gel or liquid medium to act as a coupling agent, which helps transmit waves from the transducer into the patient’s body to produce adequate imaging.2,3 Commercial ultrasound gel is the gold standard because it consistently produces excellent coupling, is easy to apply and clean up, allows for easy sliding of the probe, and is generally safe for patients and ultrasound equipment. 2 However, commercial gel can be poorly suited for austere use because it is relatively expensive and is a heavy, single-purpose product that can be cumbersome to carry.2,3 Cheaper alternatives, such as constituted glucomannan powder, cassava flour, bulla, and cornstarch, have been shown to perform as well as commercial gel in terms of image quality. 2 -8 These alternatives must be prepared prior to use, and thus, their use may be limited in emergent austere situations. A water bath approach has also been shown to perform similarly to commercial gel, although the practicality of this technique is largely limited to extremities. 9 -11
There is a paucity of information on alternatives to commercial gel in a wilderness or backcountry setting, where the only available resources are those that are carried in backpacks. The primary outcome of this study was the ability to make a clinical decision using alternative media in POCUS. The secondary outcomes were to explore the technical components of images to assess for agreement with the primary outcome and assess the products for usability.
Methods
This was a randomized, interventional, prospective study utilizing a noninferiority analysis, which evaluated 9 commonly carried toiletry and food products as gel alternatives compared with the Aquasonic 100 (Parker Laboratories, Inc, Fairfield, NJ) commercial ultrasound gel. Gel alternatives included the following: (1) Dr. Bronner’s clear liquid body soap; (2) tap water; (3) Purell hand sanitizer; (4) Pert shampoo; (5) Lubriderm body lotion; (6) NO-AD SPF 45 sunscreen; (7) McLure’s Grade A Pure Vermont maple syrup; (8) Pics olive oil; and (9) Clif energy gel shot in Double Espresso. The gel alternatives were chosen based on the authors’ perception of the likelihood of being carried into the backcountry or on an expedition; the lack of known ability to cause corrosive damage to the skin or transducers; and in the case of maple syrup, a regional novelty. All gel alternatives were stored and used in a room at a temperature of approximately 21°C (70°F). The institutional review board (IRB) at Dartmouth-Hitchcock Medical Center determined that the investigation did not qualify as human subjects research and was exempt from IRB review and approval.
Two emergency medicine physicians credentialed in ultrasound with wilderness medicine fellowship training used Phillips Lumify (Koninklijke Philips N.V.,) fitted with a broadband phased array transducer (4-1 MHz) with a mechanical index of 0.5 and frame rate of 29 Hz, attached to a Samsung S-6 (Ridgefield Park, NJ) tablet in the extended focused assessment with sonography in trauma (e-FAST) factory setting. Ultrasound clips were obtained from 2 models for analysis. Both models were men with a healthy-range body mass index (BMI) and no known anatomic abnormalities or known pathologies. The models properly consented to and were informed of the voluntary nature of the research, procedures, and potential risks. The sonographers each imaged 1 model, from whom they obtained and recorded 4-s clips from 8 windows: right upper quadrant, left upper quadrant, pelvic, lung apex, cardiac parasternal long axis, cardiac parasternal short axis, antecubital fossa, and popliteal fossa (Figure 1). Imaging windows, which included those performed in the e-FAST examination, and musculoskeletal ultrasound examinations were chosen because they are commonly used in emergency and trauma situations and allow for assessment of gel alternatives at a wide array of tissue types and depths.
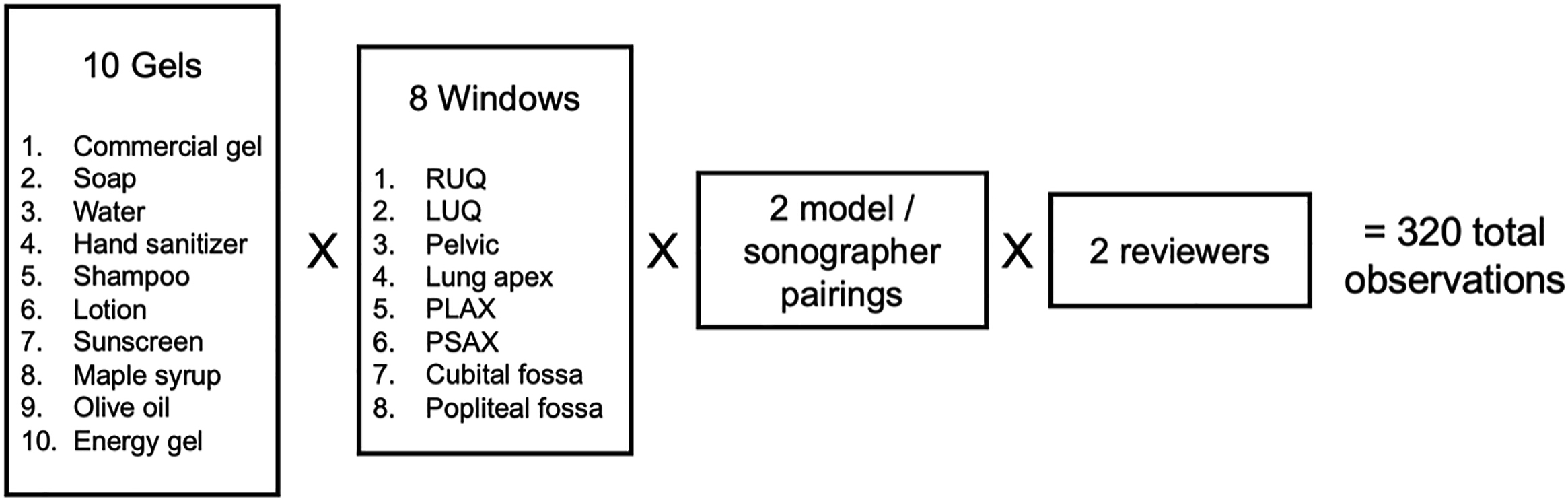
Experimental design. LUQ, left upper quadrant; PLAX, parasternal long axis; PSAX, parasternal short axis; RUQ, right upper quadrant.
Sonographers began by obtaining clips in each window using the commercial gel (Figure 2). They were instructed to obtain the appropriate view for each window, with a marking on the models serving as a precise and reproducible guide for scan location. From this consistent marked location, sonographers were allowed to optimize image acquisition based on their experience and expertise. The probe and model were cleaned between attempts, and the procedure was repeated for each of the remaining gel alternatives. All gel alternatives and commercial gel were applied directly to the models’ skin (ie, no water baths). Sonographers were unblinded to the gel alternative with which they were working and were not restricted in the volume of media used to obtain the clips. They were asked to record their impression of each gel alternative by rating each on the Likert scale (1–5) based on the metrics of ease of application, adherence, ease of sliding, and ease of cleanup. These observations were entered into Microsoft Excel (version 16.61) for descriptive analysis. All scans were obtained in a single 3-h time period.
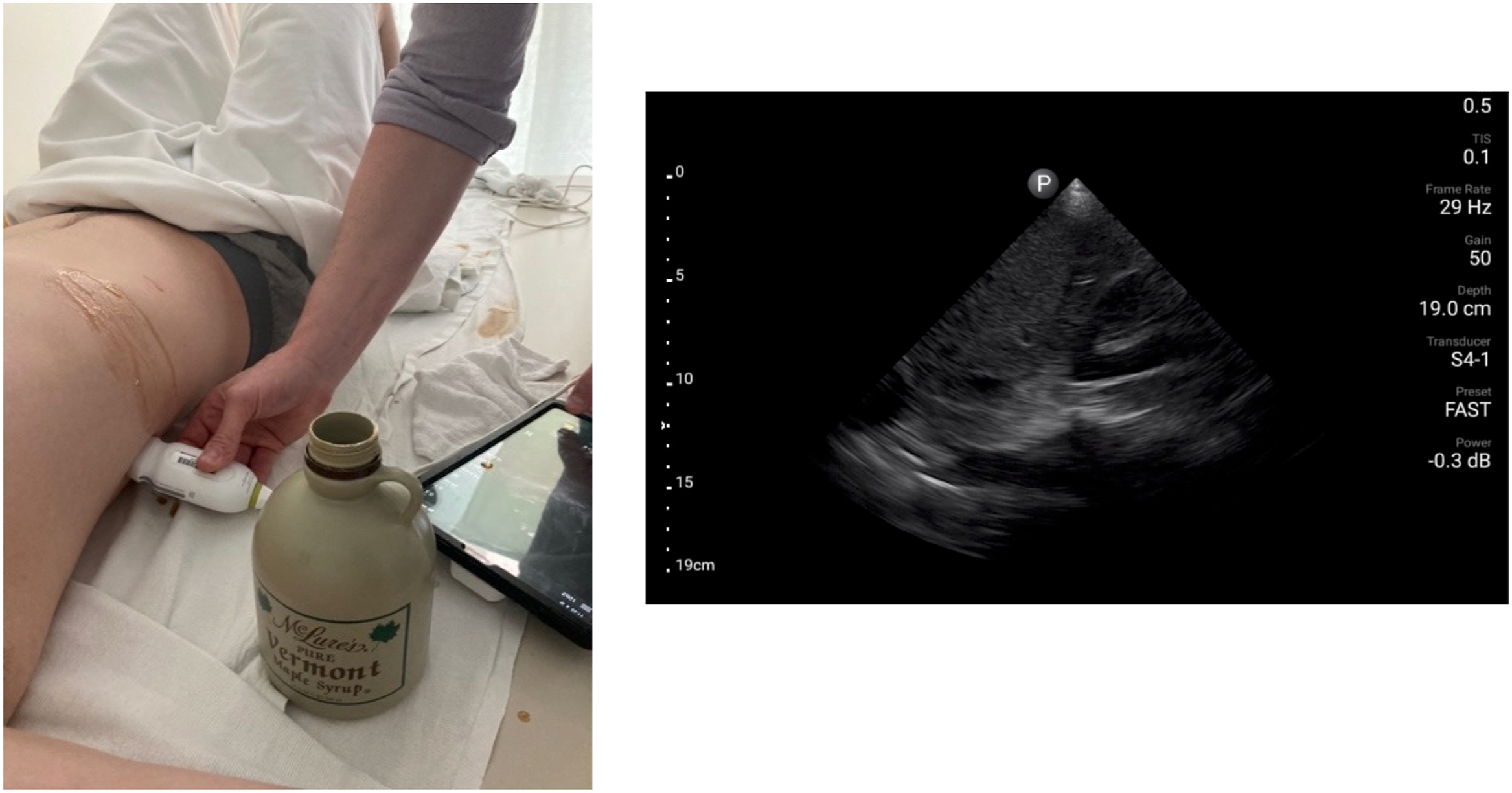
Sonographers obtained windows from models using gel alternatives and Lumify. Shown here is maple syrup, assessed in the right upper quadrant.
The clips were loaded into Synchronicity image archival and documentation software (FUJIFILM SonoSite Inc., Bothell, WA), and each clip was randomized to a number between 1 and 160 using a random number generator linked to a key. This allowed for complete blinding of reviewers. Reviewers were instructed to review clips in Synchronicity in order. The clips were sorted into blocks by window such that all clips of a certain window were viewed together by the reviewer (ie, parasternal short-axis images were assigned to identification numbers 1–20). The gel alternative and model were then randomized within each block so that the reviewers did not know which media or model they were reviewing within that block.
Two emergency medicine faculty members who had completed an advanced emergency ultrasound fellowship each reviewed 160 deidentified video clips, generating a total of 320 observations. With regard to the primary outcome, the reviewers determined whether the quality of each clip was adequate to make a clinical decision with a dichotomous yes or no response. This standard was based on established American College of Emergency Physicians (ACEP) emergency ultrasound standard reporting guidelines and consistent with our institutional ultrasound quality assurance (QA) criteria. 12 With regard to the secondary outcome, the reviewers were then asked to rate each clip on the Likert scale (1–5) on 3 aspects of clip quality, including resolution, artifact, and tissue contrast. Definitions regarding interpretations of images on this scale were clearly defined for each metric (Figure 3). Study data were collected and managed using the secure Research Electronic Data Capture platform (version 11.3.4; Vanderbilt University, Nashville, TN) hosted at Dartmouth Health.
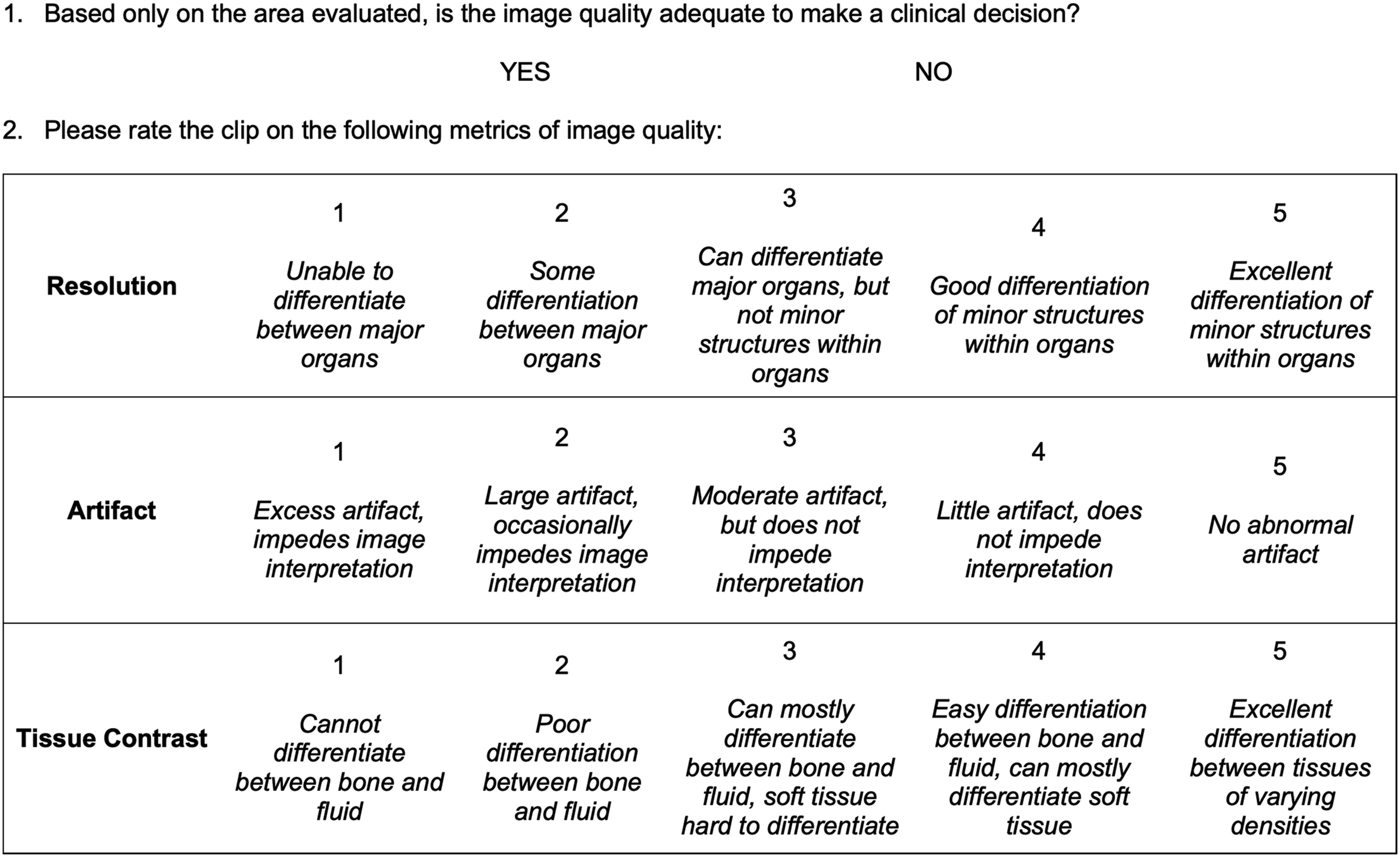
Response rubric for image review.
Statistics
Results were evaluated using a noninferiority approach compared with that for the Aquasonic gel control. Because this study was based on the ability to make clinical decisions in an austere setting, the ability of a gel to produce serviceable images is more important than technical perfection. A noninferiority margin of 20% was, therefore, selected based on ACEP and internal QA guidelines, which denote that a Likert scale rating of 4 or 5 represents a study that can reliably produce a clinical interpretation, correlating to a 20% difference on the 5-point Likert scale. 13 The 20% noninferiority margin was applied to our study as follows: for the dichotomous primary outcome of image adequacy to make a clinical decision, noninferiority was demonstrated when the upper bound of a 1-sided 97.5% CI (α=0.05) of the difference between the Aquasonic gel control and gel alternative did not exceed 20%. For the secondary outcomes (ie, resolution, artifact, and contrast), the noninferiority margin was chosen as 20% of the mean of the Aquasonic gel control data (Δresolution=0.81, Δartifact=0.71, Δcontrast=0.87). For these outcomes, noninferiority was demonstrated for the experimental media if the upper bound of a 1-sided 97.5% CI (α=0.05) did not exceed the corresponding threshold for each secondary outcome. Continuous and ordinal results are summarized as means with SDs. To ensure that no significant differences could be observed between the responses of the 2 reviewers, interrater reliability was assessed for all responses using Krippendorf Alpha and percent majority agreement. Data were analyzed using R statistical software (version 4.1.2) with the RStudio graphical user interface (version 2021.09.0+351).
Results
A total of 318 of 320 (99%) expected observations were obtained. During data attainment, a parasternal short-axis window using soap was unintentionally not gathered. The reviewers deemed a total of 300 images (94% of observations) as adequate to make a clinical decision. Eighteen of these 318 (6%) observations were rated as inadequate to make a clinical decision. Thirteen of these 18 (72%) observations were in the parasternal short-axis window. Interrater reliability for image accuracy, calculated using Krippendorf Alpha, was 0.06 (percent majority agreement: 90%), 0.46 for resolution (percent majority agreement: 52%), 0.52 for contrast (percent majority agreement: 43%), and 0.52 for artifact (percent majority agreement: 54%). With regard to our secondary outcomes, the reviewers were consistently within ≤1 unit disagreement on the Likert scale 96% of the time (153/159 observations).
The faculty reviewers rated clips that were captured using standard commercial gel for adequacy in making a clinical decision 94% of the time (Table 1). At the designated noninferiority margin of 20%, all media, with the exception of sunscreen, were noninferior to commercial gel in terms of adequacy in making a clinical decision (Figure 4).
Image adequacy of gel alternatives compared with that of commercial gel a
Note that 97.5% CIs are used for the difference to account for the 1-sided nature of the comparison (α=0.05).
Differences are commercial gel − gel alternative. Values >0 indicate that the commercial gel was more favorable than the gel alternative, whereas values <0 indicate that the commercial gel was less favorable than the gel alternative.
Denotes noninferiority at a 20% margin.
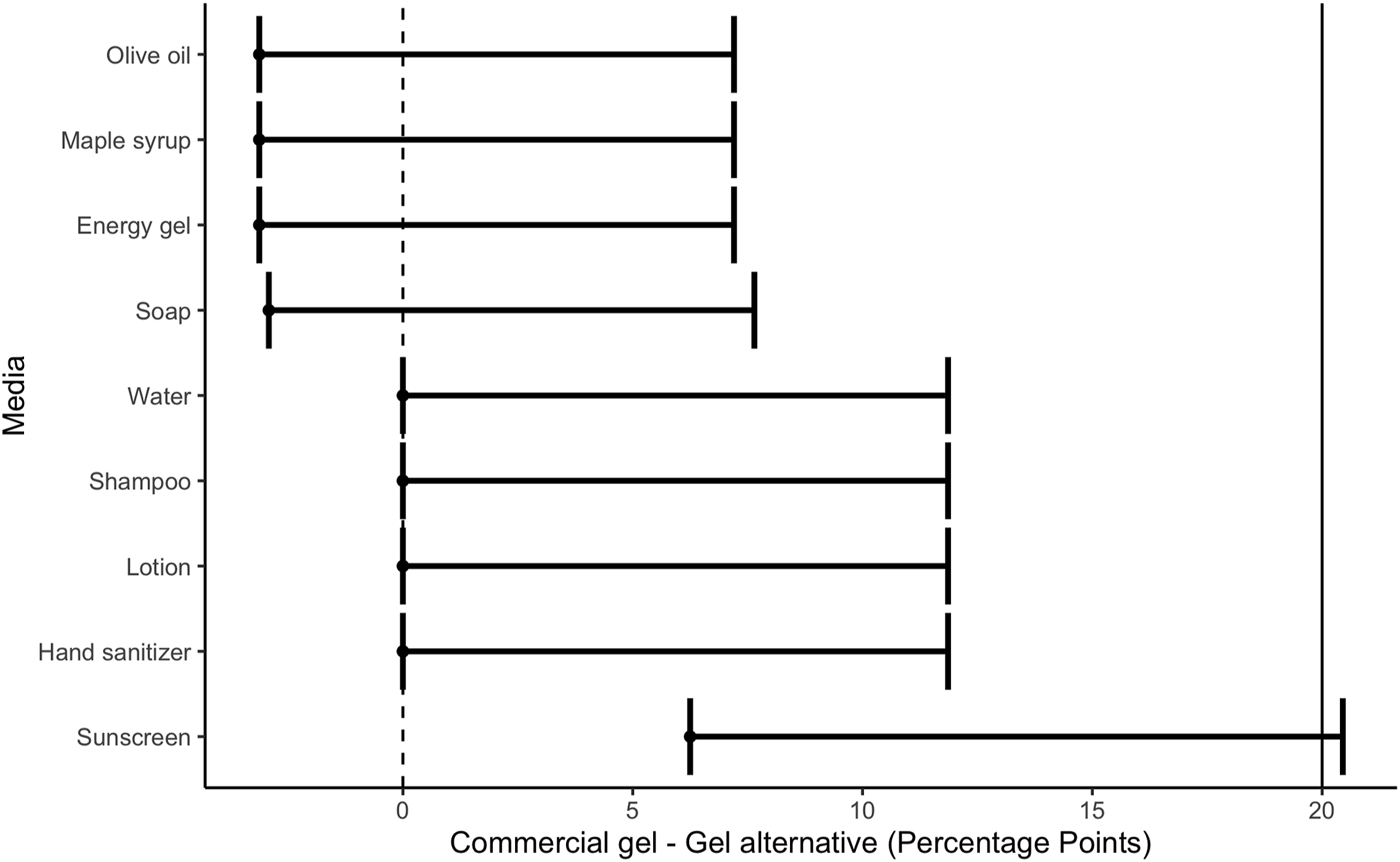
Image adequacy of gel alternatives compared with that of commercial gel. The mean and 1-sided CIs of the difference between commercial gel and gel alternatives are displayed. Gel alternatives, with the exception of sunscreen, fall within the 20% noninferiority (NI) margin (solid vertical line) as the upper boundary of the CI does not exceed the NI margin.
Second, the faculty reviewers assessed the technical aspects of clips for resolution, artifact, and contrast (Table 2). All gel media scored highest for resolution and contrast while scoring uniformly lower for artifact (commercial gel mean of 4.06, 4.19, and 3.50, respectively). The resolution of clips captured with any gel alternative was noninferior to that of the commercial gel (Figure 5). For every outcome, gel alternatives were noninferior to the commercial gel.
Image resolution, artifact, and contrast of gel alternatives compared with those of commercial gel a
NI, noninferiority; UB, upper bound.
Note that 97.5% CIs are used for the difference to account for the 1-sided nature of the comparison (α=0.05).
All differences are commercial gel − gel alternative. Values >0 indicate that commercial gel was more favorable than the gel alternative, whereas values <0 indicate that commercial gel was less favorable than the gel alternative.
Denotes noninferiority at a 20% margin.
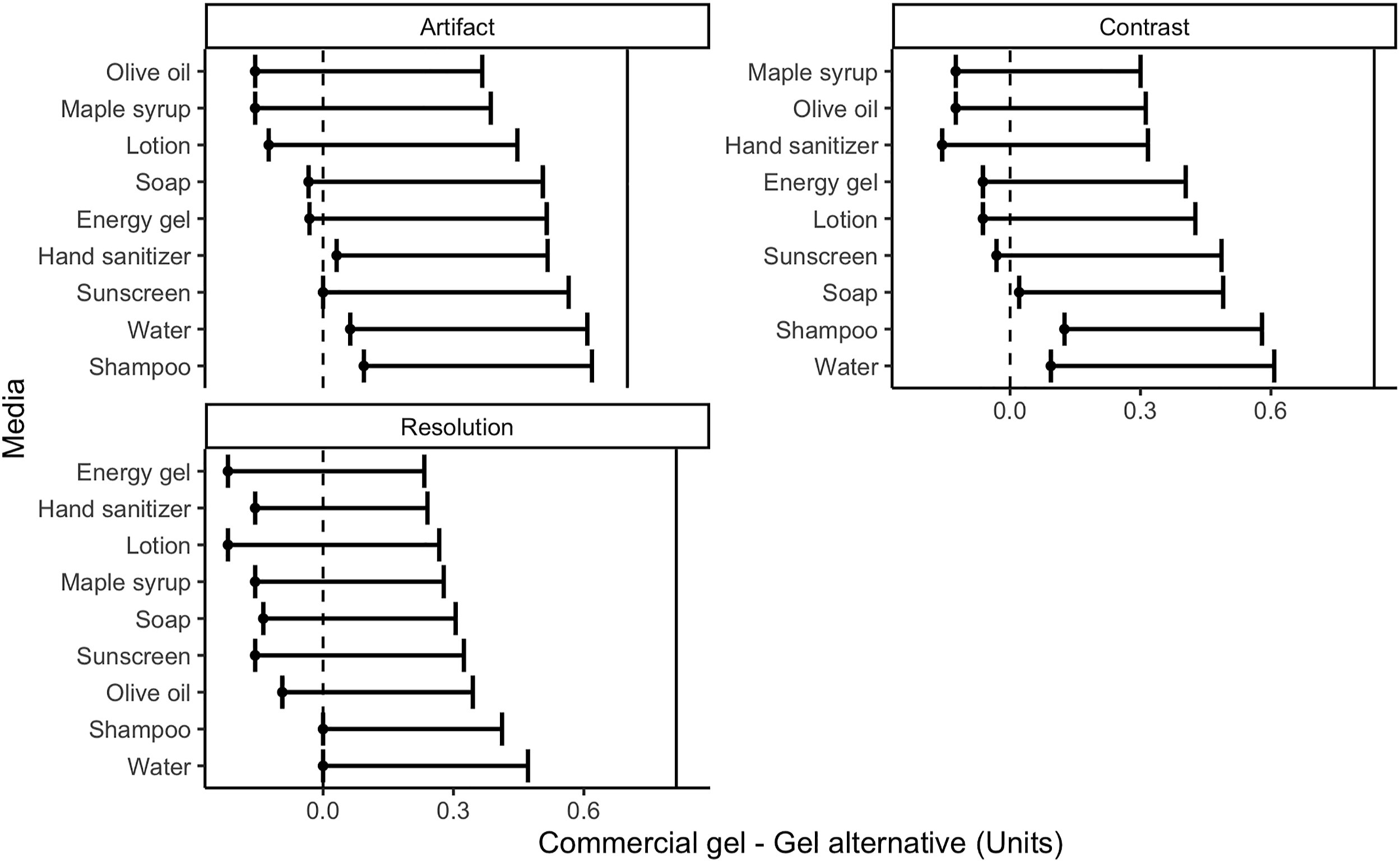
The resolution, artifact, and contrast of gel alternatives are compared with those of commercial gel at a 20% noninferiority (NI) margin. The mean and 1-sided CIs of the difference between commercial gel and gel alternatives are displayed. Gel alternatives fall within the calculated 20% NI margin (solid vertical line) as the upper boundary of the CI does not exceed the NI margin.
Using the Likert scale, sonographers also provided their ease-of-use impressions of gel alternatives in comparison with those of the commercial gel (Table 3). They were often in agreement, rating the gel alternatives no more than 1-point different in all but 1 instance. They agreed that water was equal to commercial gel in terms of ease of application; all other gel alternatives were rated as worse than commercial gel by at least 1 sonographer. They also rated water as much better than standard gel for ease of cleanup. They rated the gel alternatives as comparable for ease of sliding. Energy gel was rated strongly by both sonographers as having adherence much better than standard gel and having ease of sliding and cleanup much worse than standard gel.
Sonographer impressions of gel alternatives a
Key: 1, much worse than standard gel; 2, a little worse than standard gel; 3, equal to standard gel; 4, a little easier than standard gel; 5, much better than standard gel.
Discussion
This study investigated whether common liquid substances can be substituted for commercial ultrasound gel to make clinical decisions. Regarding the primary outcome, assessing the clinical applicability of gel alternatives as substitutes for commercial gel, we found that all gel alternatives, with the exception of sunscreen, are noninferior to commercial gel in their ability to capture images that are adequate to make a clinical decision. Although the sunscreen utilized in this study did not contain zinc, it is possible the chemical makeup of sunscreen may hinder its acoustic features and limit the coupling ability of this media. 14 Interestingly, in the secondary assessment of the technical adequacy of the clips on resolution, artifact, and contrast, all substances, including sunscreen, were noninferior to commercial gel. These results may suggest an unmeasured dimension influencing image quality above and beyond these 3 technical elements that ultimately hinder image interpretation.
The general acceptability of these substances as ultrasound coupling agents removes 1 additional burden to the use of ultrasound in wilderness and austere settings, where carrying commercial gel can add nonessential weight. Prior studies have shown that reconstituted powders can substitute for commercial gel. Our results are additive to these studies by examining gel alternatives that do not require additional time or resources. 2 -6 User preferences for certain gel attributes or availability of liquids in their pack could play a role in guiding the choice of a gel alternative in a low-resource environment. For example, adherence and difficulty in the cleanup of energy gel may limit its use as a coupling agent in a backcountry setting. In addition, although this study tested a wide range of substances, including food products, such as maple syrup and olive oil, wilderness experts may find that small toiletries, such as multipurpose shampoo, are most commonly on hand. Thus, substance availability may guide the choice of gel alternatives in low-resource environments. Our results confirm literature findings that water works as well as commercial gel as a coupling agent, although its best use may be limited to the described water bath technique because of its poor adherence.10,11 In addition, it should be noted that temperatures <0°C may freeze water-based coupling agents while increasing the viscosity of those that do not freeze at 0°C. Coupling agents with less water content may perform better in extreme cold environments and should be considered when deciding on the preferred coupling agent.
Although none of these substances was found to be corrosive to the transducer in this study, limited data exist on the effects of prolonged use of these substances on the equipment. Commercial gel and water are the only substances that have been demonstrated to be safe for both transducers and skin.10,11 Although damage is unlikely to be significant with incidental usage, we are unable to recommend any other substances than commercial gel or water for long-term repetitive use on ultrasound equipment.
Limitations
We noted the following study limitations. As described above, the parasternal short axis generated the fewest clinically adequate images. Image reviewers remarked that structures were harder to identify in this view. Sonographers were instructed to mark the patient before obtaining clips to create uniformity in the acquired window. An off-centered mark, or the capture of clips at different phases of the respiratory cycle in this window, could have limited the interpretation of the parasternal short-axis view.
In addition, the generalizability of our results may be limited by the nature of the experimental design. All clips were captured from 2 male models with a normal-range BMI and no known pathologic conditions. Images were acquired indoors in a controlled environment. Future investigation with a larger trial that recruits a more diverse subject pool would establish the validity of our results. Because of the inherent need to apply the probe and gel substitute to the volunteer, sonographers were not able to be blinded to the gel alternative. Although sonographers may have optimized image acquisition differently based on their familiarity with each gel’s consistency, they remarked that they did not notice a difference in their image acquisition time, amount of gel alternative applied, or probe manipulation based on the gel alternative that was used.
Environmental differences between our indoor study design and true wilderness settings may also have affected the ability to extrapolate our results to varying backcountry conditions. In addition, our sonographers (emergency medicine-trained physicians) and reviewers (ultrasound fellowship-trained physicians) may not reflect the true ability of backcountry users with varied experience levels to obtain and interpret images for clinical use. Reviewers with many years of experience may feel more comfortable making a clinical decision on technically limited images. A study incorporating a wider array of experience levels of medical providers in ultrasound acquisition and interpretation may confirm more generalizable results.
With regard to interrater reliability statistics, our values that are consistently <0.7 may not suggest reliable interrater reliability. 15 However, as mentioned above, only 6% of images were deemed clinically inadequate to make a decision. The limited variability in the outcome of interest limits the interpretation of the interrater reliability statistic. The percent majority agreement for the primary outcome of almost 90% suggests excellent interrater reliability and provides reassurance that interrater reliability was strong in this study. In addition, 96% agreement in secondary metrics of ≤1-point difference on the Likert scale further strengthens our conclusion of strong interrater reliability.
Conclusions
Point-of-care ultrasound has emerged as the imaging modality of choice in austere environments. However, commercial gel may be unavailable in wilderness or austere settings when the use of ultrasound is indicated. Our study suggests that many commonly carried toiletries and food products can be used as ultrasound media to produce images adequate to make a clinical decision. Wilderness practitioners may consider carrying these common liquids as dual-purpose items for intermittent use in lieu of commercial ultrasound gel.
Footnotes
Acknowledgments
The authors thank our 2 ultrasound models for their time and assistance and the Dartmouth-Hitchcock emergency department for allowing us the use of their ultrasound units.
Author Contributions: study concept and design (JNW, ZPS, SCC, JMS); data acquisition (NJD, NEW, GMK, JMS); data analysis (JNW, CCP); drafting and critical revision of the manuscript (JNW, ZPS, NJD, JMS); all authors approved the final manuscript.
Financial/Material Support: None.
Disclosures: None.
Presented as “Common liquids as ultrasound media” at the Wilderness Medical Society summer conference and, August 3, 2022, Snowmass, CO.