
Abstract
Introduction
SARS-CoV-2 poses challenges for the safe delivery of a camp experience with a medically complex camper population. Multiple studies have investigated the effect of nonpharmaceutical interventions for preventing SARS-CoV-2 transmission in traditional summer camp settings, but none in the medical summer camp settings. Our objective was to describe and evaluate the nonpharmaceutical interventions on SARS-CoV-2 transmission rate in a medical summer camp setting.
Methods
This was a single-institution cross-sectional study conducted between June 2021 and August 2021 in a rural summer camp setting in upstate New York. Nonpharmaceutical interventions consisted of prearrival guidance on low-risk activities, obtaining negative SARS-CoV-2 polymerase chain reaction results within 72 h prior to arrival, adult SARS-CoV-2 vaccine mandate, universal masking mandate, small cohorts, daily symptom screening, and rapid testing on site. Primary cases were defined as an individual with a positive SARS-CoV-2 test result of any type while at camp or 2 wk after departure from camp without any known exposure at camp; secondary cases were defined as cases from potential exposures within camp.
Results
Two hundred and ninety-three campers were included. Nine individuals were tested owing to potentially infectious symptoms while at camp. Thirty-four campers were tested because they arrived from a county with an a priori intermediate level of SARS-CoV-2 community spread. Zero on-site rapid tests were positive for SARS-CoV-2.
Conclusions
We describe the implementation of multilayered nonpharmaceutical interventions at a medical summer camp during the SARS-CoV-2 pandemic.
Introduction
Advances in medical diagnostics and therapeutics have resulted in more children living with chronic medical conditions. 1 While mortality for these individuals has decreased, psychosocial morbidity, such as anxiety, depression, and self-esteem disturbances, has increased. 2 SARS-CoV-2, the microbe responsible for COVID-19, has had significant ramifications for the lives of children since 2019. 3 Children have been exposed to loss of loved ones, household financial hardship, food insecurity, asynchronous education, restrictions of in-person interactions, and gaps in typical psychosocial outlets, resulting in negative health outcomes. 4 -7 Summer camps foster the development of social skills, team work, problem solving, and self-identity.8,9 Medically complex children often cannot participate in traditional summer camps and therefore are not provided the opportunity to develop such skills. Medically complex children do, however, have the opportunity to attend medical summer camps, where they learn the same life-long skills as in a traditional summer camp, in addition to learning different coping mechanisms, management of their own illness, and altruism. 10 -14 Therefore, the pandemic has the potential for greater negative biopsychosocial ramifications in the medically complex child.11,15,16
Multiple studies have described the range of nonpharmaceutical interventions (NPIs) implemented in traditional summer camp settings. These NPIs have been used to mitigate the transmission of SARS-CoV-2 with varying degrees of success. 17 -22 To our knowledge, none of these studies has evaluated the role of NPIs in a medical summer camp setting. The objective of this study was to describe the demographics, NPIs, and transmission patterns of SARS-CoV-2 among medically complex children while attending a medical summer camp.
Methods
Study Design
This was a single-institution cross-sectional study conducted between June 2021 and August 2021 in a rural summer camp setting in upstate New York. The study was conducted at a residential medical summer camp with approximately 50 to 60 campers per session with 6 sessions of 5 d duration. The study was determined to be exempt from review by the Albany Medical Center institutional review board, and therefore consent was not required. All enrolled campers were included. No one was excluded from the study. Data were entered directly into a Research Electronic Data Capture (REDCap) tool hosted at Albany Medical Center. Individual-level demographic data (ie, age, gender, and county of residence) and medical data (ie, medical history, SARS-CoV-2 vaccination status, and SARS-CoV-2 infection history) were gathered from the self-reported application. All “prearrival” SARS-CoV-2 polymerase chain reaction (PCR) tests and “during session” SARS-CoV-2 nucleic acid amplification tests (NAATs) and their results were gathered on an encrypted central camp database.
NPIs
Prearrival Screening
Seventy-two hours prior to the first day of a camp session, the medical team assessed the level of SARS-CoV-2 transmission within the 11 counties surrounding the camp. An a priori definition of risk included low risk, intermediate risk, and high risk (Figure 1).
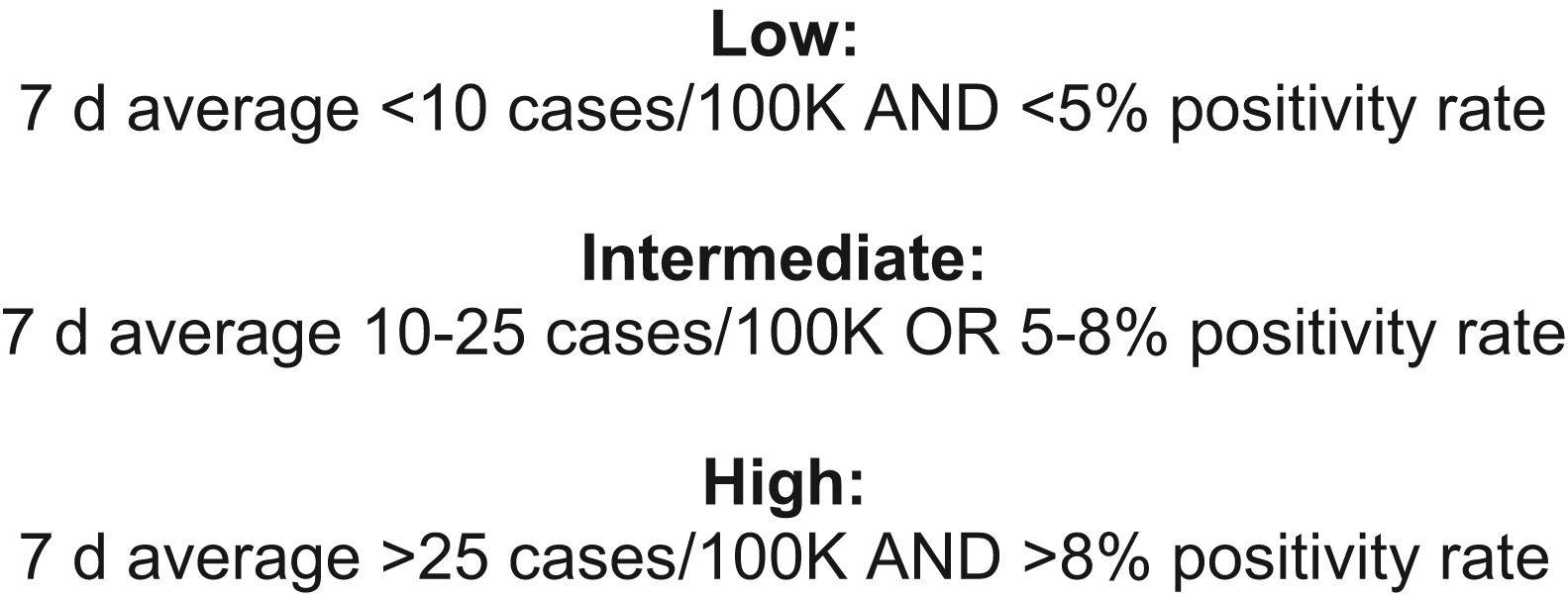
Prearrival risk stratification of SARS-CoV-2 infection community spread.
If community risk was low, prearrival and in-session mitigation strategies were implemented as described later. If community risk was intermediate, the same mitigation steps as for low risk were implemented in addition to performing rapid SARS-CoV-2 NAATs upon arrival to the camp for all individuals coming from counties with non–low-risk community infectivity. If community risk was high, the camp did not open for that session.
Mitigation Steps
Prearrival mitigation steps included a prearrival screening telephone call and prearrival SARS-CoV-2 testing. Screening telephone calls were performed by the medical staff calling the camper’s family 2 wk prior to arrival to evaluate travel/exposure history. The medical staff also informed the family that the household should quarantine until arrival at the camp. Prearrival testing involved all campers providing documentation of a negative SARS-CoV-2 PCR result within 72 h prior to arrival on site.
In-Session Mitigation Steps
Staff vaccination mandate: All staff and volunteers were required to be fully vaccinated against SARS-CoV-2 2 wk prior to arrival on site.
Daily symptom screening: Every morning prior to leaving their cabin, all staff members and campers underwent a standardized symptoms screen by medical staff (pinpoint SARS-CoV-2 screening, Wellcheck. Monkton, MD). If an individual reported any symptoms, they were evaluated by the camp physician.
Cohorting: On site, cohorts were made up of 10 campers and 5 to 7 staff members.
Universal masking: Masks were worn by all campers/staff unless the only people present were within the on-site cohort or they were eating/drinking, participating in an aquatic activity, or sleeping.
Intentional staffing pattern: Activity areas that required specific training/certifications had dedicated staff assigned to that area and were counted within an on-site cohort. This allowed for small cohorts without a lot of “cross-contamination” within a program area by the program staff.
Intentional common space utilization to allow for social distancing: Each on-site cohort had a designated indoor and outdoor dining area to physically distance every cabin from one another, while all masks were down during mealtime.
Specific-person under investigation protocols: Any potentially infectious complaint was evaluated in an infirmary physically separate from the noninfectious infirmary. Any infectious complaint had a rapid SARS-CoV-2 NAAT performed on site. If negative, they could return to camp activities per standard medical policies. If positive, the whole cabin cohort was sent home.
Statistical Analysis
Descriptive analysis was used to describe camper demographics, index cases, primary cases, secondary cases, primary attack rate, and secondary attack rate. Index cases were defined as an individual with a positive SARS-CoV-2 test result of any type while at camp or 2 wk after departure from camp without any known exposure at camp; primary cases were defined as cases from potential exposures while at camp. Secondary cases were defined as cases from potential exposures to primary cases. A contact was defined as any individual who had close contact (<2 m [6 ft] for ≥15 min within a 24 h period) with a primary case with or without masks while at camp. The primary attack rate and secondary transmission rate were calculated according to previous studies. 18 The primary attack rate was calculated as the number of new primary cases during the camp session of infection divided by the number of campers on-site during the session of infection. The secondary transmission rate was calculated as the number of secondary cases among contacts of index cases. Chronic medical conditions were defined as any medical condition expected to last >12 mo and require the care of a specialist provider.
Results
The study cohort consisted of 499 total individuals, with 242 of those being campers. The mean age of the campers was 12 y. As seen in Table 1, 168 (69%) were from the state of New York, with 27% of those campers being from the Capital District region of New York (composed of Albany, Columbia, Fulton, Greene, Montgomery, Rensselaer, Saratoga, Schenectady, Schoharie, Warren, and Washington counties). Of the 242 campers, 192 (79%) had a chronic medical condition; the most common were sickle cell disease (22%), bleeding/clotting disorders (13%), cerebral palsy (10%), and epilepsy (6%). Of the 242 campers, 87 (36%) were vaccinated. All eligible campers were vaccinated with the Pfizer Biontec messenger RNA vaccine because this was the only SARS-CoV-2 vaccine that had US Food and Drug Administration emergency use approval in patients aged <18 y old at the time of the study. Two hundred thirty-nine campers (99%) had a negative SARS-CoV-2 PCR test result prior to arrival at camp.
Camper demographics
SLE, systemic lupus erythematosus.
Of those who were vaccinated.
Percentage of those with chronic medical conditions. Chronic medical conditions are not mutually exclusive.
A total of 232 infirmary visits were logged, a combination of staff, volunteers, and campers. As seen in Table 2, 38 total SARS-CoV-2 tests were performed during the study period, with 4 resulting from symptomatic testing and 34 resulting from asymptomatic screening in persons coming from counties with intermediate risk of SARS-CoV-2 transmission. Overall, there were no positive SARS-CoV-2 test results while persons were on site or for 2 wk after their departure from camp. There were no index, primary, or secondary cases of SARS-CoV-2 infection. No sessions were canceled because of high-community spread or SARS-CoV-2 outbreak within camp.
SARS-CoV-2 transmission patterns.
Discussion
No transmission of SARS-CoV-2 was observed within this residential summer camp for >60 d. This is the first study to our knowledge that evaluates the transmission of SARS-CoV-2 within a residential summer camp for medically complex children. Our findings correspond with those from previous studies that show low-transmission rates when a multilayered mitigation approach to infection control is implemented. 17 -22 Similarly, our findings are consistent with findings of studies showing low-transmission rates within schools that have a multilayered mitigation approach to infection control. 23 -26 Our findings are contrasted by findings of studies that show high-transmission rates within residential summer camp communities without a multilayered mitigation approach to infection control. 27
The limitations of our study include a small sample size of 242 campers. This study was limited to only one medical summer camp in one isolated geographic region of the United States. Each camper was only on site for 5 d. This study was conducted during a period when Alpha and Delta variants of SARS-CoV-2 were the most prevalent variants. The lower transmissibility of these variants than those of other variants, such as Omicron, poses a potential limitation to the generalizability of this study. Lastly, this study took place during a period with low community SARS-CoV-2 transmission rates (28 cases/100,000 7 d average in New York State over the 60 d study period).
Conclusions
In this study, we described the implementation of a multilayered mitigation approach to infection control in a medically complex summer camp population. Future research should focus on evaluating the effectiveness of such measures in broader geographic locations, times of higher community SARS-CoV-2 transmission rates, times of differing variants of concern, and populations with varying chronic medical conditions.
Footnotes
Acknowledgements
Acknowledgments: The authors thank Erik Reidel, MD for assisting in the development of study design.
Author Contributions: study concept and design (KW, SN, AA, CW); data acquisition (KW, SN, AA, CW); data analysis (KW, SN, AA, CW); drafting and critical revision of the manuscript (KW, SN, AA, CW); approval of final manuscript (KW, SN, AA, CW).
Financial/Material Support: None.
Disclosures: CW is the Medical Director of Double H Hole-in-the-Woods Ranch. SN is the Nursing Director of Double H Hole-in-the Woods Ranch. None of the other authors have disclosures.