
Abstract
The COVID-19 pandemic has imposed significant mental health burdens upon the general population worldwide, either directly owing to the disease or indirectly through aggressive public health measures to control spread of the virus that causes COVID-19. In this narrative review, we used a systematic approach to summarize the impact of restrictive lockdown measures on the general mental health of people living in Victoria, Australia during 2020 and to identify the groups with an increased risk of adverse mental health outcomes. A systematic database search (Ovid Medline, PsycINFO, Embase) for articles examining the mental health of Victorians in the context of the COVID-19 pandemic during 2020 yielded 88 articles, of which 15 articles were finally included in this review. We found that the general mental health of Victorians was negatively affected by COVID-19 restrictions during 2020. Although studies reported heterogeneous mental health outcomes, we found that the general population consistently used coping strategies and demonstrated mental health help-seeking behaviors in response to the restrictions. Women, children, young people, carers, people who became unemployed owing to the pandemic, and those with pre-existing psychiatric conditions had a higher risk of adverse mental health consequences during the COVID-19 pandemic in 2020.
Introduction
The novel coronavirus SARS-CoV-2, initially detected in Wuhan, China in December 2019, has spread to nearly 200 countries worldwide. 1 By the end of 2020, the COVID-19 pandemic had led to more than 79 million reported cases and caused over 1.7 million deaths. 2 In an effort to limit the spread of the virus and support health services at risk of being overwhelmed, governments around the world implemented restrictions to limit people’s movements, such as physical distancing, restrictions on social gatherings, industry and education closures, stay-at-home orders, and lockdowns. These COVID-19 pandemic suppression strategies were effective at slowing the spread of the virus 3 but were not without profound social, economic, and psychological consequences. 4
In March 2020, the World Health Organization recognized the global increase in fear, stress, and anxiety in response to the pandemic. 4 An early study in Italy, the first European country to be seriously affected by SARS-CoV-2, showed high rates of post-traumatic stress disorder, depression, anxiety, insomnia, perceived stress, and adjustment disorder symptoms. 5 These mental health presentations were either directly associated with SARS-CoV-2, such as by infection with the virus or death of a loved one, or indirectly related to lockdown measures owing to the pandemic, such as having a lack of certainty about the future, reduced income or unemployment, and social isolation. 5 In Switzerland, higher levels of stress, anxiety, loneliness, and depression were reported owing to COVID-19 pandemic restrictions, tightened physical and social isolation, and decreased emotional support. 6 Worldwide, the mental health impacts have been profound. However, further research is required to distinguish between direct and indirect consequences of the COVID-19 pandemic.
In the state of Victoria, Australia, the prevalence and transmission of SARS-CoV-2 remained relatively low throughout 2020. Proportional to the number of SARS-CoV-2 cases, the Victorian government imposed some of the strictest restrictions in the world.7,8 As of 30 November 2020, Victoria had recorded 20,345 confirmed cases of SARS-CoV-2 since the beginning of the pandemic and 820 deaths. 9 The first epidemic wave in Australia began in March 2020, with nationwide implementation of COVID-19 pandemic suppression strategies, including national border closures, 1.5-meter social distancing, stay-at-home orders, work-from-home directives, industry and school closures, and bans on public and household gatherings. 10 After a brief period of staggered lifting of restrictions in late May 2020, a second wave of SARS-CoV-2 emerged in Victoria, prompting the state government to instate the most stringent measures in Australia. New stricter rules were introduced in August 2020, including a maximum 1 hour of outdoor exercise daily, travel restrictions to within 5 km of one’s home, and an 8 pm to 5 am curfew, in addition to the restrictions implemented during the first lockdown. 11 These rules were strictly enforced by Victorian police, who were authorized by the Victoria Department of Health under the Pandemic Declaration to issue on-the-spot fines of AUD 1652 to individuals for infringement of the emergency measures. 12 By 13 May 2020, the Victorian police had completed 43,829 COVID-19 police checks and issued 2894 fines and 833 warnings. 12 These rules were enforced until a gradual staged reopening began in September 2020, with the state entering COVID-Safe Summer rules on 7 December 2020 and most restrictions lifted except for limits on density and gatherings. 11 In 2020, Melbournians in the capital of Victoria spent 154 days in lockdown, 43 days during the first lockdown from 30 March to 12 May (the “first wave”), followed by 111 days during the second lockdown from 8 July to October 27 (“second wave”). 13 This was one of the longest lockdowns in any region during 2020. 14
Emerging evidence from other countries on the adverse mental health consequences of lockdowns indicates that it is important to specifically investigate these effects in Victoria, Australia, where restrictions were relatively long and onerous. 15 In this narrative review, we aimed to summarize the impact of COVID-19 pandemic restrictions on the mental health of Victoria residents in 2020 and identify the groups with an increased risk of adverse mental health outcomes during the pandemic. The information in this review can assist public health officials and policymakers in decision-making when implementing further COVID-19 pandemic suppression strategies. This review can also provide valuable insight for primary care physicians, psychologists, and other relevant mental health professionals and organizations regarding the impact of COVID-19 pandemic restrictions on the general population of Victoria. This narrative review will also assist in identifying which groups are most vulnerable and at higher risk of developing adverse mental health consequences during a pandemic.
Methods
Literature search strategy
On 16 August 2021, we conducted a search of OVID Medline, PsycINFO, and Embase for publications related to the mental health of residents in Victoria, Australia associated with the COVID-19 pandemic.
The first Medline search included the Medical Subject Headings (MeSH) terms “COVID-19” and “pandemics.” These were combined using the Boolean operator OR in a title and abstract search using the terms “coronavirus,” “SARS-CoV-2,” “COVID-19,” and “pandemic.” The second Medline search included “Victoria*” or “Melbourne” in a title and abstract search. Next, we used the MeSH terms (“Mental Health,” exp “Stress, Psychological,” exp “Suicide,” exp “Anxiety,” “Depression”), combined with title and abstract searches of the terms “mental*,” “psych*,” “mood*,” “psychosocial,” “psycho-social,” “stress*,” “distress*,” “burnout,” “burnt-out,” “burnt out,” “burn out,” “burn-out,” “anxiet*,” “worry,” “worri*,” “fear*,” “depress*,” and “lonel*.” Subject headings were explored when sub-headings were deemed relevant to this review. The three searches were combined using the AND Boolean operator. Results were limited to studies published from “2019-current” to exclude studies prior to the COVID-19 pandemic. The same search was performed in Embase. In PsycINFO, Thesaurus of Psychological Index Terms (exp “Mental Health,” exp “Psychological Stress,” exp “Stress,” exp “Social Stress,” exp “Stress Reactions,” exp “Stress and Coping Measures,” exp “Depression (emotion),” exp “Anxiety,” “Fear,” and “Stress”) were used rather than MeSH terms.
Inclusion and exclusion criteria
The inclusion criteria were all studies that investigated the mental health of Victorians (Australia) during the COVID-19 pandemic.
The exclusion criteria were studies about mental health associated with direct COVID-19 infection, study protocols, clinical correspondence, journal letters, and articles without an available full text. We also excluded studies of psychotic disorders, electroconvulsive therapy, in-patient admissions, and psychiatry treatment practices (e.g., telehealth patterns). However, we included studies reporting emergency department psychiatric presentations.
An ethics review and informed consent were not necessary as the study was a narrative review of existing literature.
Results
The initial search identified 133 articles, 58 from Medline (OVID–All), 6 from PsycINFO, and 69 from Embase. These were imported into Covidence software. 16 Duplicates were automatically removed and the retrieved articles were then checked manually, leaving 88 articles. The title/abstract and then full text of these articles were screened by one reviewer (JJ), according to the inclusion and exclusion criteria. An independent reviewer (HA) subsequently verified the suitability of the included and excluded studies, according to the inclusion and exclusion criteria. Any disagreements were solved through discussion. The results of study selection are shown in Figure 1.

PRISMA diagram.
Ultimately, 15 articles were included in this review, including 7 cross-sectional surveys, 4 retrospective data analyses, 2 qualitative studies, 1 cohort study, and 1 mixed-methods study. Table 1 provides the details of each study.
Summary of selected studies.
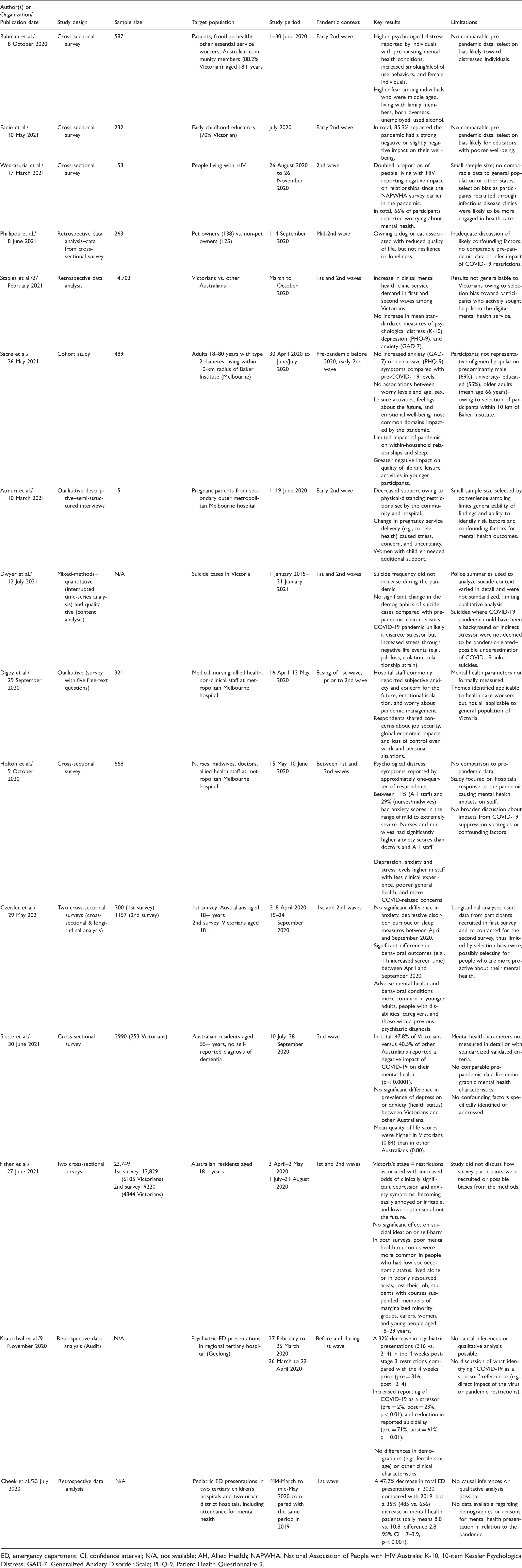
ED, emergency department; CI, confidence interval; N/A, not available; AH, Allied Health; NAPWHA, National Association of People with HIV Australia; K-10, 10-item Kessler Psychological Distress; GAD-7, Generalized Anxiety Disorder Scale; PHQ-9, Patient Health Questionnaire 9.
The 15 articles included different study populations. Rahman, et al., 17 Staples et al., 18 Czeisler et al., 15 and Fisher et al. 19 reported on the general population. The remaining studies focused on early childhood educators, people living with HIV, pet owners, adults with type 2 diabetes, pregnant women, health care workers, older Australians, and children.
The articles included different study periods during 2020. Kratochvil et al. 20 and Cheek et al. 21 focused on the first epidemic wave of SARS-CoV-2 in March to May 2020. Rahman et al., 17 Eadie et al., 22 Weerasuria et al., 23 Phillipou et al., 24 Atmuri et al., 25 and Siette et al. 26 studied the second wave during July to October 2020. Staples et al., 18 Sacre et al., 27 Dwyer et al., 28 Czeisler et al., 15 and Fisher et al. 19 included both the first and second waves. Finally, Digby et al. 29 and Holton et al. 30 conducted their studies between the first and second COVID-19 epidemic waves in 2020.
Generally, the included studies reported that the mental health of Victorians was negatively affected by the COVID-19 pandemic in 2020. However, variability and nuance were apparent amongst studies. In the discussion, we detail the general trends and variation in the findings of the included studies.
Discussion
In this review, we found that during the COVID-19 pandemic in 2020, the general mental health and well-being of residents in Victoria decreased. However, the prevalence and degree of negative effects varied across the included studies. The evidence regarding the impact of pandemic restrictions on anxiety and depression levels was not consistent. Fisher et al. reported a significant increase in clinical depression (to 44.1%) and anxiety (to 32.3%) among the adult population during the lockdown implemented in the second wave of the COVID-19 pandemic in Victoria. These findings were nearly double those reported in other Australian states with less restrictive measures, 19 indicating a negative effect of restriction and social isolation on mental health. Two cross-sectional surveys compared mental health among Victorians with residents of other Australian states and assessed the change in adult behaviors between the first and second waves in Victoria. Depressive and anxiety symptoms were assessed using the Patient Health Questionnaire 9 (PHQ-9) and Generalized Anxiety Disorder Scale (GAD-7), respectively, both of which are well-validated and reliable scales.31,32 Czeisler et al. 15 found no significant difference in the prevalence of anxiety and depressive symptoms among adults in Victoria, based on two separate surveys in April and September 2020. 15 A potential reason for the differing findings of the studies by Czeisler and Fisher and their colleagues15,19 is that the former study relied on longitudinal data from participants in a multi-time-point study, compared with Fisher’s cross-sectional work. 19 It is possible that participants in the multi-time-point study were more pro-active about their mental health compared with participants in a single time-point project. This difference could also be explained by the findings of a cross-country study that found higher levels of anxiety, depression, and stress in Polish participants compared with Chinese participants. 33 The studies by Fisher and Czeisler and their colleagues15,19 did not compare the prevalence of mental health parameters according to the specific cultural and ethnic backgrounds of participants. The population of Victoria is multicultural and ethnically diverse, which could contribute to the variability between these studies.
Poor mental health is associated with a variety of biopsychosocial variables including social isolation, alcohol use, and deficits in cognitive ability.34–37 Czeisler et al. 15 demonstrated significant changes in the behavior of adults during the lockdown, such as having a considerably increased screen time and circumventing COVID-19-related information. 15 Additionally, 10% of participants reported new or increased substance use (e.g., alcohol, legal/illegal drugs, and prescription drugs) to cope during the second wave of SARS-CoV-2 in Victoria. 15 This is consistent with studies in other countries that found increased alcohol use associated with social isolation and lockdown.38,39 Further studies on alcohol consumption post-lockdown during the COVID-19 pandemic are needed to further quantify the extent of drug and alcohol use in the community.
In a retrospective study by Staples et al., 18 the trends in mental health symptoms and use of the digital Mental Health service platform (MindSpot Clinic digital mental health service) were compared with pre-pandemic access to similar services. 18 Although those authors found a significant increase in the use of the digital mental health service during the first and second epidemic waves in Victoria, they did not observe any significant increase in psychological distress (10-item Kessler Psychological Distress, K-10), depression (PHQ-9), or anxiety (GAD-7) among users compared with pre-pandemic levels. 18 The authors argued that an increase in service demand was owing to Victorians with mild or moderate mental health symptoms accessing the service. 18 Therefore, whereas the number of people experiencing and seeking help for mental health symptoms increased, the average severity of symptoms did not. That study supports an earlier systematic review 40 examining global sub-syndromal anxiety, depression, and stress responses to the COVID-19 pandemic in Victoria. 40
Our review highlights the importance of alternative service delivery, such as digital mental health services, to assist with high demands on mental health access during and after the strict COVID-19 pandemic suppression measures in Victoria. Staples et al. 18 also reported a significant decrease in the mean age of users of its digital mental health service, from age 35 years in the early weeks of the pandemic to age 32 years by weeks 29 to 32. 18 Although it can be argued that the negative effect of SARS-CoV-2 on mental health could be a result of the disease itself, the literature in the Australian context shows that adverse mental health outcomes were minimally associated with direct SARS-CoV-2 exposure and strongly associated with restrictions that disrupted work and social functioning. 41
More severe adverse mental health outcomes were commonly observed in women, carers, young people aged 18 to 29 years, people from low socioeconomic backgrounds or those with reduced work or unemployment owing to the pandemic, people with disabilities, and people with a previous psychiatric diagnosis.15,18,19 The vulnerability of these populations to poor mental health outcomes is consistent with other studies in Australia42,43 and other countries.44–48 Children and adolescents were not immune to the negative impact of the COVID-19 pandemic on mental health. An audit of two tertiary children’s hospitals and two urban district hospitals found a 35% increase in mental health-related presentations during the pandemic compared with the previous year whereas total presentations to the emergency department decreased by 47.2%. 21 Additionally, an Australian cross-sectional survey showed worse mental health deterioration in adolescents with a history of depression or anxiety during the pandemic. 49 Two systematic reviews confirmed the findings of studies conducted in Victoria and reported that children are more vulnerable to the negative effects of containment measures such as social distancing, isolation, and school closures, even though they may be less vulnerable to SARS-CoV-2 itself.50,51 These studies revealed higher rates of anxiety, depression, and sleep and appetite disturbance among children and adolescents during the pandemic period. These findings are important for primary health care providers, policy makers, and governments to provide extra training, education, and support for identifying and managing adolescents and younger adults at risk of adverse mental health outcomes. Further research is required to quantify the impacts of COVID-19 pandemic suppression strategies on children in Victoria.
The restrictive measures enforced during the second wave of the COVID-19 pandemic in Victoria have adversely affected other specific groups and populations. Increased psychological distress symptoms have been reported in 25% of frontline health care workers in hospitals throughout Victoria.17,29,30 This could be explained by the relatively higher exposure rates of health care staff working in hospitals with suspected and confirmed cases of COVID-19. 52 Improving understanding of the virus as well as high vaccination rates among health care staff may reshape the initial response of frontline health care workers to the pandemic. Further research is required to evaluate the longer-term mental health challenges among frontline workers owing to the COVID-19 pandemic. People with specific diseases such as diabetes were concerned about engaging in leisure activities, uncertainty about the future, and emotional well-being, 27 and people living with HIV reported a negative impact on their relationships owing to the pandemic. 23 The impact of COVID-19 pandemic restrictions on personal relationships is a global problem,53–55 highlighting the need for strategies to improve social connectedness, optimism, and quality of life.
Several strengths and limitations of this review should be considered. Of the 15 articles found using the search strategy above, only three studies (those of Fisher et al., 19 Czeisler et al., 15 and Staples et al. 18 ) were generalizable to adults in Victoria without being significantly biased toward a specific population group. Many studies were cross-sectional analyses that lacked comparative baseline data; therefore, causal inferences could not be made. The study by Fisher et al. 19 has several advantages over other similar studies. That study had the largest sample size (n = 23,749) and the sample was representative of the general adult population in Victoria. Their study also used national baseline data from the first survey, allowing for a measurable difference to be determined in comparison with the second survey, which was initiated during the second COVID-19 wave in Victoria. However, the study by Fisher et al. 19 also has some limitations, including a lack of discussion regarding the recruitment process (e.g., how the survey was advertised or accessed), which could limit its generalizability. Similar to that research, the design of the study by Czeisler et al. 15 could not demonstrate causality regarding mental health findings and relied on self-reported outcomes rather than diagnostic interviews. The work by Staples et al. 18 had inherent population biases and could only provide information about Victorians who actively chose to engage with its service, who were probably more psychologically-minded and mentally well enough to be motivated to seek help. Lastly, we did not use a measure of bias or study quality when reviewing the included articles.
Conclusion
In the present review, we found that the general mental health of residents in Victoria, Australia was negatively affected by the COVID-19 pandemic restrictions during 2020. Victorians demonstrated mental health help-seeking behavior and used coping strategies in response to the restrictions, such as increased alcohol use. Although the literature is sparse, and in particular, there are insufficient data during the second wave of SARS-CoV-2, the study findings are consistent regarding the groups that were most vulnerable to adverse mental health outcomes as a result of Victoria’s COVID-19 pandemic suppression strategies.
This review identified several populations that are at risk of poorer mental health outcomes, including women, children and young people, carers, and people with disabilities. Demographic risk factors also include pre-existing psychiatric health conditions, low socioeconomic status, unemployment, and marginalized minority groups. These groups were mentioned consistently in the included studies in relation to Victoria, as well as globally. This highlights the importance of future research, policy interventions, and strategies to address poor mental health in the population, particularly focusing on these specific groups in Victoria, as they are most vulnerable to the negative effects of pandemic restrictions.
This review encompasses studies focusing on mental health outcomes in the 2020 COVID-19 pandemic context. During 2021, Victoria experienced recurrent lockdowns and became the city with the most days of lockdown globally (262 days). 56 2021 presented new challenges such as “pandemic fatigue,” with one review finding decreasing adherence to some COVID-19 pandemic suppression strategies, such as physical distancing, as the pandemic continued. 57 Another study suggested that poorer personal resilience and coping skills are associated with lockdown fatigue. 58 Studies conducted in the context of the 2021 pandemic are lacking, with ongoing enforcement of COVID-19 pandemic suppression strategies, increased knowledge of the virus, and the roll-out of COVID-19 vaccines. As the pandemic continues to unfold in Victoria, in Australia, and globally, alongside ever-changing COVID-19 pandemic suppression strategies and vaccination strategies, ongoing assessment of the impact on population mental health will continue to be important issues in future research.
Footnotes
Acknowledgements
The authors would like to thank Anna Lovang (St Vincent’s Hospital Library Service) for her assistance in refining the literature search.
Declaration of conflicting interests
The authors declare that there is no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.