
Abstract
Pectoralis major tendon ruptures are rare injuries. We present a case of a pectoralis major tendon rupture incurred while bouldering that required surgical repair. The diagnosis of pectoralis major tendon rupture relies predominantly on clinical examination. Among athletes, outcomes after surgical repair are superior to those after nonoperative therapy in most cases of complete tendon rupture. Although infrequent, pectoralis major tendon ruptures can occur while climbing, and early recognition and expedited surgical treatment are paramount to maximize functional recovery.
Introduction
Rock climbing and bouldering are increasingly popular sports, practiced both indoors and outdoors. Bouldering is commonly described as unroped climbing on large boulders and is a popular form of climbing. Injuries may be incurred during bouldering as a result of acute use, chronic overuse, or a fall. Upper extremity injuries are common in climbing and may be seen in 25 to 90% of all climbing-related injuries, depending on chronicity. 1 -3 These injuries can range from acute sprains, fractures, or dislocations to chronic overuse injuries. 1 -3 Despite the high frequency of upper extremity injury among climbers, to our knowledge, acute pectoralis major tendon rupture during bouldering has not yet been described.
We present a case of an acute torn pectoralis major tendon experienced while bouldering. Although an uncommon injury, a complete pectoralis major tendon tear often requires surgery, ideally as soon as feasible after injury.
Case Report
An otherwise healthy 37-y-old man presented to the outpatient clinic for the evaluation of right shoulder pectoralis pain after a climbing injury. The patient had climbed for 22 y, and his preinjury climbing ability was 5.12 and V6 on the Yosemite decimal and V-grade bouldering scales, respectively. The patient reported performing a mantle maneuver to top out an outdoor boulder problem 3 d prior. As he was attempting the mantle, he felt a tear and a pop at the border of his right pectoralis major muscle and fell. He subsequently noticed a deformity around his right pectoralis region and an ecchymosis around his right bicep (Figure 1). The patient self-rescued and did not seek immediate medical care. The patient endorsed a history of a partial right pectoralis major muscle tear 9 y earlier but had experienced no other injuries to his right torso or shoulder girdle.

Patient after injury. Note ecchymosis at the bicep area (gray arrow) and loss of anatomic axillary contour (black arrow).
On examination, the patient had a full active and passive range of motion of his shoulder with 5/5 strength with an empty can and bear hug testing. There was no bicep tenderness; however, ecchymosis was observed on the anterior aspect of the biceps tendon (Figure 1). On the hands-on-hip test and resisted abduction, he had a deformity of the pectoralis insertion without a palpable pectoralis tendon insertion at the humerus and asymmetry compared with the other side. A magnetic resonance image of the right chest demonstrated an acute, full-thickness, full-width tear in the right pectoralis major tendon, with the proximal tendon retracted by approximately 3 cm with respect to the distal tendon stump and approximately 3.5 to 4 cm from the humeral insertion. Given the activity level of the patient, his desire to return to climbing, and his profession as a trauma surgeon, the patient wished to proceed with open right shoulder pectoralis tendon repair to maximize functional recovery.
The patient was taken to the operating room 7 d after injury and placed in the beach chair position. A deltopectoral incision was made from the midanterior shoulder, veering laterally toward the pectoralis insertion. Subcutaneous flaps were created, and the cephalic vein was identified and protected. The sternocostal head of the pectoralis major and a portion of the clavicular head had ruptured and retracted medially by 3.5 cm (Figure 2). The tendon was debrided to healthy tissue and secured in place onto the humerus using 4 permanent titanium bone anchors in a Krakow fashion. Blood loss was minimal, and the patient was discharged the same day.
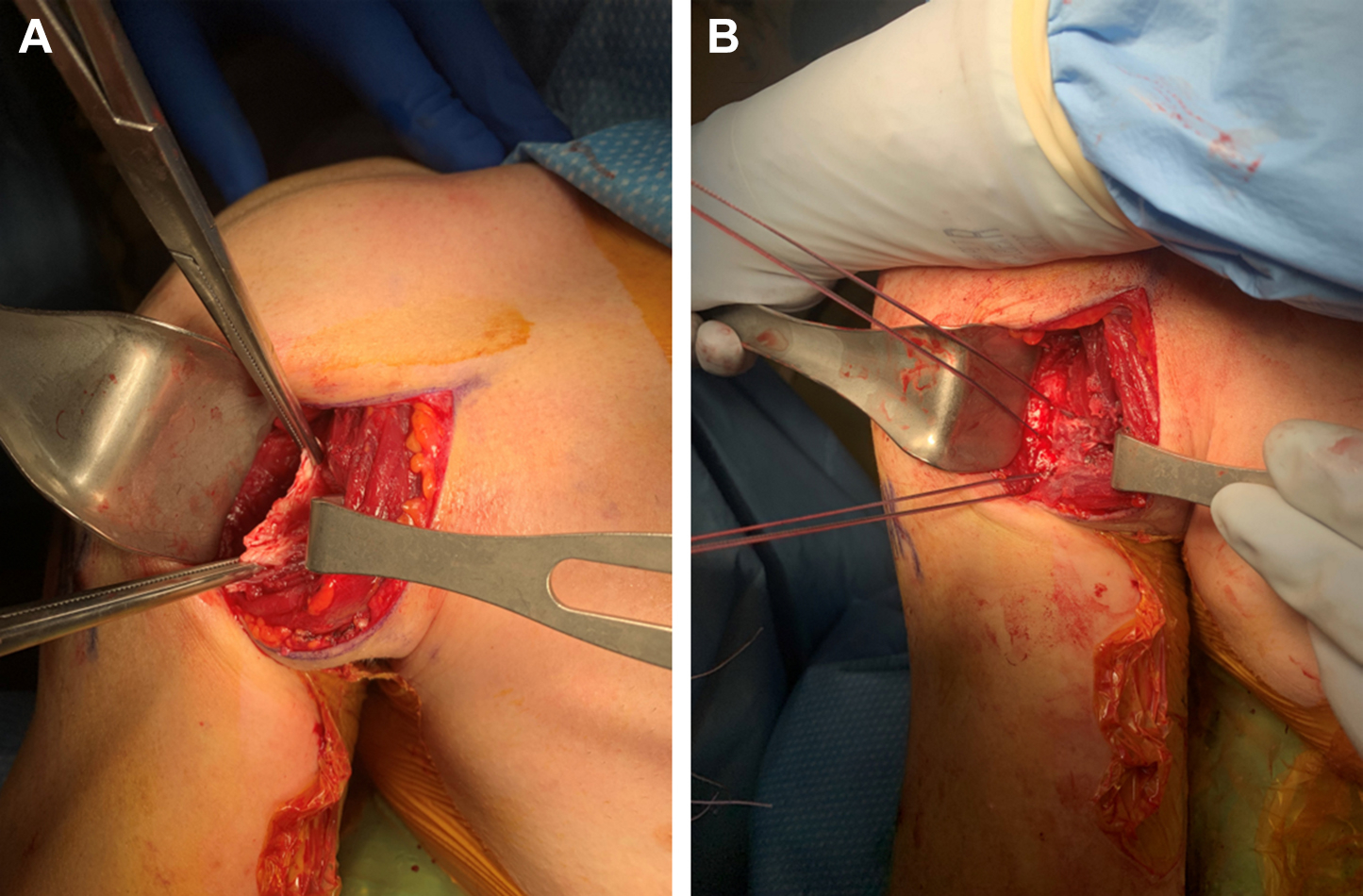
The operative findings during pectoralis major repair. A, Disrupted pectoralis major tendon grasped with Kocher clamps. B, Disrupted pectoralis major tendon secured in place on the humeral insertion.
Full right upper extremity range of motion was achieved at 8 wk. By 4 mo, the patient was bouldering consistently at V4, and by 6 mo, he was climbing at his preinjury level.
Discussion
The pectoralis major is a prominent muscle of the anterior thorax, consisting of a clavicular and sternocostal head. 4 The tendon of the pectoralis major inserts on the humerus at the lateral lip of the bicipital groove. 4 The pectoralis major is vital to adequate adduction, flexion, internal rotation of the humerus, and general dynamic stabilization of the shoulder. 5 To enable power production through a range of muscle shortening velocities, the pectoralis major demonstrates considerable variation across muscle segment lengths. Unfortunately, this range of power production comes at a cost. There may be a considerable amount of force generated at the lower bounds of the tendinous insertion of the lower muscle fibers when the pectoralis major is eccentrically contracted while abducted and externally rotated, predisposing this site to avulsion or tear. 4 -6
Pectoralis major tendon ruptures are rare injuries but may be increasing, with a total of 365 cases reported between 1822 and 2010 and 76% of cases reported after 1990. 5 When present, these injuries generally occur in 20- to 40-y-old male athletes and have been associated with bench press or high-contact sport participation. 5 -8 Of the 365 cases described by ElMaraghy et al, 5 11 were of women, 10 of whom were nursing home residents, suggesting a different mechanism of injury in this group. Pectoralis major ruptures are broadly partitioned into 3 categories: 1) muscular tears (muscle origin and muscle belly), 2) tendinous tears (musculotendinous junction, intratendinous, and humeral insertion), and 3) bony avulsion. 5 Clinical diagnosis can be made by observing a deformity of the anterior axillary fold, ecchymosis on the arm on the affected side, and weakness with resisted adduction and internal rotation. Patients often endorse sharp pain followed by a pop or tear when the humerus is abducted and externally rotated. 9 -11 When the physical diagnosis is not clear, magnetic resonance imaging is the diagnostic imaging modality of choice, although ultrasound may be a useful adjunct in more resource-limited situations.6,11-13
Early and accurate diagnosis of a pectoralis major rupture is important because prompt surgical repair improves functional outcomes, strength, and cosmesis for active patients.6,10 Outcomes for patients undergoing surgery are substantially better than those for patients undergoing nonsurgical management (particularly with acute ruptures), with 90% of surgical patients reporting an excellent or good functional outcome, as reported by the Bak criteria, compared with only 17% of nonoperatively managed patients (Table 1). 6 Early repair within 8 wk, and ideally within 7 d, has been advocated to maximize the likelihood of achieving preinjury physical activity, avoid scar formation, minimize tendon retraction, and decrease the need for an allograft.6,14 Among professional football athletes in the National Football League, the mean time from injury to surgery was 6.8±9.6 d, an aspirational goal for the time from injury to surgery. 10 After surgery, 79 to 95% of patients regain their preinjury functional ability.7,8 Most patients return to their previous activity levels within 4 to 12 mo.11,15
Bak criteria for functional recovery after pectoralis major rupture repair 6
Complete rupture of other large upper extremity muscles and tendons has been described in climbers, more commonly in the biceps or triceps. 16 -18 The repetitive chronic upper extremity stress associated with bouldering and climbing may predispose these athletes to acute injuries superimposed upon chronic microtrauma.1,11 It is also possible that postural changes occur over time in climbers, predisposing a patient to injury, particularly on the anterior aspect of the chest wall or upper extremity. 19 Similar to a pectoralis major muscle rupture, repair of these injuries in an active climber should be treated surgically, given the loss of strength and decreased range of motion associated with nonsurgical therapy. 16 -18
Although rare, a pectoralis tendon rupture may be encountered by wilderness healthcare providers, particularly because an increasing number of climbers are pursuing bouldering further afield. Mantling may be a particularly high-risk move for pectoralis major rupture in bouldering and climbing because of the abduction and external rotation required. Diagnosis can be confirmed via physical examination in most cases. Expedient surgical intervention is critical; hence, evacuation may be necessary if prolonged self-rescue is anticipated, particularly for athletes most likely to benefit from early surgical repair.
Conclusion
Pectoralis major tendon rupture is a rare injury acquired during rock climbing or bouldering. Early identification and treatment of this injury are essential because operative repair provides superior functional outcomes for active individuals.
Footnotes
Funding
Disclosures: JDF has received unrestricted research funding from Varian for an investigator-initiated clinical trial (
Acknowledgements
Author Contributions: literature review, manuscript preparation, and critical review (JDF); acquisition of figures, manuscript preparation, and critical review (DVC); manuscript preparation and critical review (TM); review and final approval of the manuscript (JDF, DVC, TM).
Financial/Material Support: None.
Neither of these leads to conflicts of interest for this article.