
Abstract
Introduction
Collisions against obstacles (CAOs) on ski areas account for a large proportion of deaths of skiers and snowboarders but are poorly documented. We aimed to characterize the risk factors and injuries of CAOs and to compare occurrences of CAOs with 2 control groups.
Methods
Between 2015 and 2019 in France, data were collected on the injured population by ski area doctors and ski patrollers. Systematic counts were also made to describe the noninjured population on ski slopes. Cases (CAOs injured: 3391 victims) were compared with 2 controls (non-CAOs injured: 198,302 victims and the noninjured population: 121,227 people). Crude and adjusted logistic regressions were performed (P<0.05).
Results
Males, highly skilled participants, skiers, and people aged <26 y had higher risks of being injured after a CAO than a non-CAO. Moreover, CAOs more frequently occurred off-slopes and on very easy slopes; lifts were more often involved. Injuries to the head and neck and trunk were more likely to occur after CAOs than non-CAOs. Medical helicopters were more often used for CAOs than non-CAOs. Compared with the noninjured population, no age, sex, or sport group appeared clearly at risk of CAOs.
Conclusions
Typical victims of CAOs are males, skiers, young people, and highly skilled participants. This population was previously identified for moving fast on the slopes and having risk-seeking behavior, putting them at risk of high-energy accidents. There is a need for adequate prevention, such as awareness campaigns, and protection, such as individual device and padding on obstacles, that focus on protecting against injuries to the head, neck, and trunk.
Introduction
Alpine snow sports are popular activities, with >53 million skier days in France in 2018–19. Natural obstacles, such as trees and rocks, and manmade obstacles, such as tower lifts and snow guns, are located on or close to ski slopes. They are responsible for a small percentage of accidents (5% of ski patrol reports 1 ) but can lead to severe injuries. Collisions against obstacles (CAOs) cause between 35 and 73% of deaths on ski slopes2,3 and 48% of moderate and severe traumatic brain injuries (TBIs). 4
The most recent studies focusing on CAOs were performed before 1994. 5 -7 These studies provided the first description of CAOs: victims were often males and highly skilled skiers. Since then, several changes occurred in the design of ski equipment, such as the size and shape of skis, the development of parabolic skis, and the development of the snowboard, which was not included in the initial studies. 5 -7 In addition, the slope environment has been changed with respect to grooming and the development of protection devices attached to obstacles to protect people in case of a CAO. The more recent epidemiologic studies did not target specific accident mechanisms such as CAOs. These studies mentioned only the percentage of CAOs as the cause of accidents on slopes, 1 head injuries,4,8 or deaths on slopes.2,3
A better characterization of CAOs was required to improve the prevention of some of the most severe accidents on ski areas. The goal in this study was to investigate the distinctive characteristics of CAO-related injuries: the types of injuries, the differences between victims of CAOs and other accidents, and the risk factors for CAOs.
Methods
The Association des Médecins de Montagne (MDM) is a French epidemiological network of ski area doctors created in 1992. It collects information on snow sport accidents from 14 ski areas. The Système National d’Observation de la Sécurité en Montagne (SNOSM) is an entity that has been collecting ski patrol reports from 65 ski areas since 1996. The combination of the 2 databases included all the accidents requiring immediate treatment (Figure 1). In light of the redundancy of some accidents (those rescued by ski patrollers [SPs] and brought to local ski area medical offices) and the anonymity of the databases, which prevented us from excluding these accidents, we chose to conduct a separate analysis on these 2 databases.
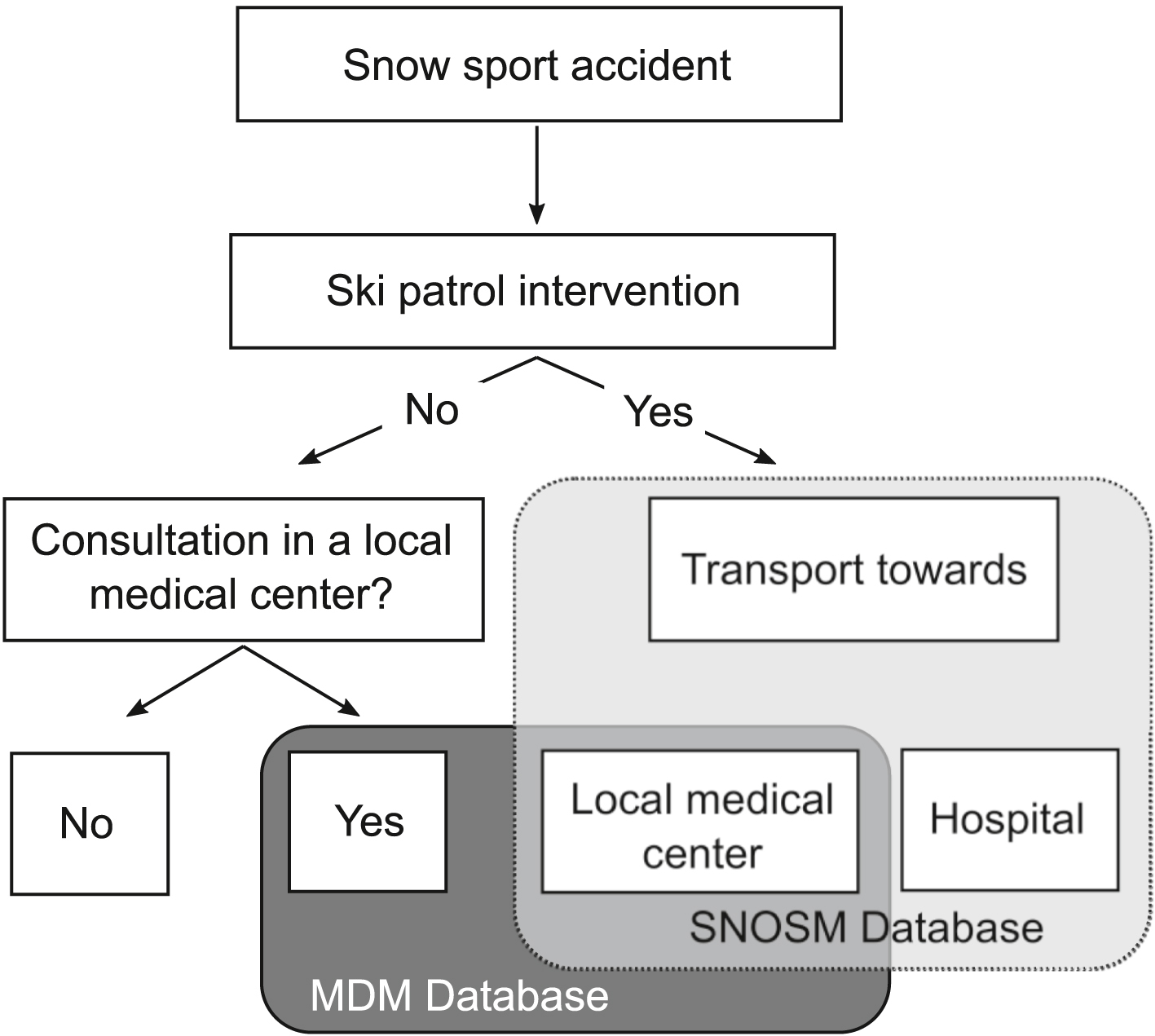
Organization of data collection. MDM, Association des Médecins de Montagne; SNOSM, Système National d’Observation de la Sécurité en Montagne.
An accident was included in the analysis when a victim had an accident while alpine skiing or snowboarding at ski areas, including on-slope, off-slope, and terrain parks. We included only accidents with a mechanism of CAOs (including natural and manmade obstacles but excluding skiing and snowboarding equipment), collision with another person (skier or snowboarder), or a noncollision such as a jump or a fall that led to a ski patrol rescue or a consultation at a ski area medical office. We analyzed accidents reported from the winter seasons 2014–15 to 2018–19. Both databases provided information on the victims (sex, age, and sport) and the injury location (head/neck, trunk, upper extremities, lower extremities, knee, and multiple). An injury was classified as multiple when the victim sustained injuries in different anatomical areas, except for a knee injury associated with another lower-extremity injury, which was recorded as a lower-extremity injury. The SNOSM database also included specific information on the slope difficulty and on the type of area where the accident occurred. The accident area was defined as "lift" when a lift was involved in the accident, accident at lift departure, arrival, collision against a lift tower, etc. The database also included information on the rescue services requested by the SPs after their first evaluation of the victim, such as an on-field intervention of a doctor and the transport of the victim by a medical or a nonmedical helicopter (ie, with or without a doctor in the helicopter). The MDM database contained additional information on the population (helmet use, back protector use, and proficiency level in skiing or snowboarding self-estimated by the victim), on whether the ski patrol transported the patient to the medical facility, and on the injury type (TBI included skull fractures, concussions, and severe TBI). The proficiency level was summarized as “experienced” when the people estimated their proficiency level as advanced or professional. This work was based on a database that obtained the approval of the regional ethical research committee (Comité de Protection des Personnes Sud Méditerranée I, Committee reference: RO-2016/01).
The MDM also performed observations from the bottom of the slopes of representative French ski areas to approximate the population on ski areas. These visual observations were conducted at various times of the winter season and in several ski areas (8 areas in 2014–15 and 2015–16, 6 in 2016–17, 3 in 2017–18, and 2 in 2018–19) to estimate the ages (child, teenager, or adult), sex, sport, and helmet use of people on slopes.
Data preparation was performed using R (R Core Team [2015], Vienna, Austria) and Matlab 2020 (MathWorks, Natick, MA). To characterize the types of CAO-related injuries and the differences with other accidents, 2 case-control studies were conducted using multiple logistic regressions (odds ratio [OR], 95% CI, and associated P value). The analysis was performed on the MDM database with CAO injured (MDM-CAO) as cases and non-CAO injured (MDM–non-CAO) as controls. A similar analysis was conducted on the SNOSM database (cases: SNOSM-CAO, controls: SNOSM–non-CAO). The dependent variable was the occurrence of a CAO. Factors for the crude OR (ORcr) were related to the population, the rescue services, the accident environment, and the injuries. Only factors associated with the occurrence of the accident were kept for the adjusted OR (ORadj) (sex, age, sport, helmet use, back protector use, self-estimated proficiency level, accident area, and slope type).
Another case-control study was conducted to investigate the risk factors of CAO injured with MDM-CAO and SNOSM-CAO as cases and the noninjured population as controls. To better understand the differences observed among MDM-CAO, SNOSM-CAO, and the noninjured population, the MDM-CAO case was divided in 2 cases: MDM-CAO rescued by SPs (MDM-CAO-SP) and MDM-CAO not rescued by SPs (MDM-CAO–non-SP). Crude and adjusted multiple logistic regressions were performed with CAOs as the dependent variable and population parameters (sex, age groups, sport, and helmet use) as adjustment factors. To match the age group definition of the noninjured population (child, teenager, and adult), the CAO population was divided into children (aged <11 y), teenagers (aged 11–15 y), and adults (aged >15 y).
The statistical analysis was performed using R. A parameter was deemed to have a significant effect if the P value was less than 0.05.
Results
During 5 winter seasons, 88,351 accidents were analyzed in the MDM database (3% CAOs, n=2568), 111,342 accidents were analyzed in the SNOSM database (1% CAOs, n=823), and 121,227 people on slopes were observed (Figure 2, Table 1). The CAO victims were most often male (≥57%), younger than 26 y of age (≥53%), skiers (≥85%), experienced (42%), and helmeted (70%) but not wearing a back protector (87%). Among the victims who consulted in a medical facility (MDM-CAO), only 35% were brought in by the SPs. Among the ski patrol rescues (SNOSM-CAO), a doctor was present for 27% of rescues. A medical helicopter was required for 13% of the rescues.
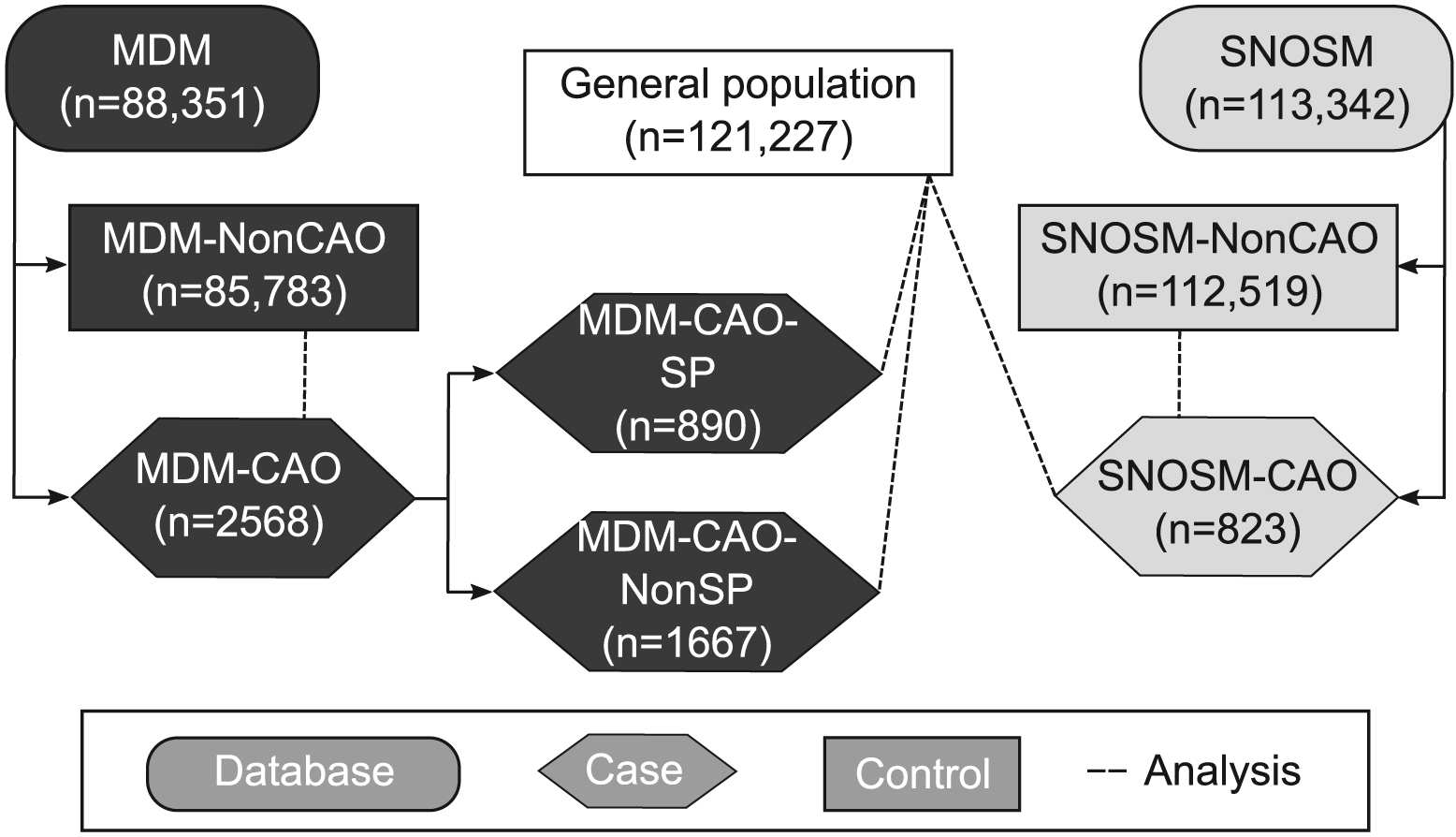
Description of cases and controls. CAO, collisions against obstacle; MDM, Association des Médecins de Montagne; NonCAO, not a collision against obstacle; NonSP, not rescued by ski patroller; SNOSM, Système National d’Observation de la Sécurité en Montagne; SP, ski patroller.
Demographic characteristics of snow sport accidents and general population
MDM, Association des Médecins de Montagne; CAO, collisions against obstacle; non-CAO, not collisions against obstacle; SNOSM, Système National d’Observation de la Sécurité en Montagne; MTI, muscle or tendon injury; TBI, traumatic brain injury.
All data are presented as n (%).
Among all CAO-related injuries, the most frequent injuries were knee sprains (11%), head/neck lacerations (11%), and trunk contusions (11%). Knee injuries were less frequent in CAO accidents (≤20%) compared with non-CAO accidents (approximately 40%) (Table 1). In CAO accidents, injuries to the head/neck (ORcr of 6.8 for the MDM database and 15.8 for the SNOSM database), to the trunk (ORcr of 3.3 and 13.2, respectively), and to multiple areas (ORcr 3.2 and 22.2, respectively) were more frequent than knee injuries (Tables 2 and 3). These injuries represented more than 42% of CAO-related injuries compared with 17% of non–CAO-related injuries. Head/Neck injuries were often lacerations (48%) or contusions (31%), whereas trunk injuries were mostly contusions (64%) or fractures (28%).
Multiple logistic regressions on MDM-CAO compared with MDM–non-CAO
MDM, Association des Médecins de Montagne; CAO, collisions against obstacle; non-CAO, not collisions against obstacle; OR, odds ratio; MTI, muscle or tendon injury; TBI, traumatic brain injury.
P<0.05.
Multiple logistic regressions on SNOSM-CAO compared with SNOSM–non-CAO
SNOSM, Système National d’Observation de la Sécurité en Montagne; CAO, collisions against obstacle; non-CAO, not collisions against obstacle; OR, odds ratio.
P<0.05.
Adjusted logistic regressions highlighted that being <26 y-old, experienced, and wearing a back protector were risk factors of sustaining CAO-related injuries rather than non–CAO-related injuries (Tables 2 and 3). Females, people aged >55 y, beginners, and snowboarders were at lower risk of CAO-related injuries. Off-slopes (ORadj=8.1) and very easy slopes (ORadj=1.6) were areas of greater risk for CAOs. Lifts were more often involved in CAO (ORadj=5.8). After adjustment, only the helmet use was not different between the CAO victims and non-CAO victims. The CAO victims were less likely to go to medical facilities with ski patrol rescue (ORcr=0.9) (Table 2). When CAO-related injuries led to ski patrol rescue (Table 3), a doctor was more frequently involved (ORcr=1.5), as was the use of a medical helicopter (ORcr=6.0).
The population injured after a CAOs and rescued by SPs was not the same as the population going directly to a medical facility (Table 4). The CAO victims who went to the doctors without the ski patrol (MDM-CAO–non-SP) were more likely to be males and adults than those rescued by SPs (MDM-CAO-SP and SNOSM-CAO). Helmet use was not significant in the crude logistic regressions and was excluded from the adjusted regressions. Crude ORs were similar to adjusted ORs.
Adjusted multiple logistic regressions on CAO compared with the population on slopes
MDM, Association des Médecins de Montagne; CAO, collisions against obstacle; non-SP, not rescued by ski patroller; SP, ski patroller; OR, odds ratio; SNOSM, Système National d’Observation de la Sécurité en Montagne.
P<0.05.
Discussion
We performed a double analysis to get an overall vision of snow sport accidents requiring urgent treatment, from accidents in which the victim went to a medical facility on their own to accidents in which the victim had to be transported to a hospital by helicopter. Medical consultations outside ski areas were not included because these accidents did not require an urgent consultation and were, therefore, likely to be associated with mild injuries. We analyzed 2 databases because each database offers a partial overview of accidents on the slopes. The MDM database covered a wide spectrum of injuries (from mild to severe) requiring medical consultations. The accidents included in the SNOSM database required immediate interventions by SPs. Injuries ranged from moderate to severe (requiring medical transport by helicopter to a hospital). The MDM database did not include the most severe accidents directly transferred to a hospital, whereas the SNOSM database did not include accidents in which the victim visited local medical facilities on their own. The 2 databases were also complementary, as the SNOSM database provided general information on victims, accident conditions, injuries, and rescue services and the MDM database provided more detailed information on victims and injuries. The analysis of these 2 databases gave an overall picture of the situation in France. This situation can be generalized to other alpine countries. They have similar snowfall patterns, slope difficulties, and speeds on the slopes.9,10 Generalizing results on a global level would require further analysis that considered the characteristics of each country.
Only 9% of non-CAOs were collisions with another person. The differences between CAOs and collisions with another person were not investigated. This study highlighted the differences between CAOs and other accidents on slopes, especially the higher risk of CAO-related injuries for young people aged <26 y, skiers, males, experienced people, and back protector users. Males, skiers, and experienced people generally have higher speeds.9,10 This population and people aged <26 y more often estimated to have a risk-seeking behavior on slopes.11,12 One possible explanation is that these experienced and risk-seeking skiers/snowboarders might ski off-slopes more frequently than beginners and cautious people. Obstacles at ski areas such as snow guns, lift towers, trees, and rocks are mostly found off ski slopes and rarely on ski slopes. This might explain the higher risk of CAO-related injury for males, skiers, people aged <26 y, and experienced people. The risk factor of being injured after a CAO with a back protector might not be caused by the protection device itself but may be associated with the population that uses it. People who use back protectors are often experienced people with risk-seeking behaviors. This population is identical to the population with a higher risk of CAOs. The use of back protectors might be an indicator of risk-seeking behavior, although this factor was not included in previous studies.11,12 On very easy slopes, there is a higher risk of CAO-related injuries than of other accidental injuries. These slopes are often crowded, frequented by all types of people, from beginners to experts. High speeds are recorded in these areas. 10 There is a need for preventive measures against CAOs on very easy slopes. All the characteristics of CAOs are key elements for future public awareness campaigns, which should highlight the risks.
In CAO-related accidents, victims are at higher risks of sustaining head, neck, and trunk injuries and SPs are more likely to call for a medical helicopter and a doctor than in other accidents. These results agree with the higher severity of CAOs compared with other accidents. This point was suggested in previous studies by the higher proportion of CAOs among severe accidents (48% among moderate/severe TBIs 4 and 35 to 73% among death2,3) compared with all accident severities (5% among ski patrol rescue 1 ). The higher risk of head injuries in CAOs emphasizes the need to promote helmet use on the slopes to reduce the severity of TBIs; unprotected head impacts against rigid surfaces are at high risks of severe head injuries, and helmet use can reduce these risks (depending on the impact speed13,14).
The CAO victims are more likely to visit medical facilities without ski patrol rescue than the victims of non-CAO. The lower proportion of knee and lower-extremity injuries in CAOs may reduce the proportion of injuries limiting the mobility of the victims and preventing them from going to medical facilities without ski patrol intervention.
We analyzed the noninjured population on slopes to investigate whether CAO victims were more often males, young people, and skiers because this population was at higher risk of CAOs or because this population reflected the noninjured population on the slopes. This analysis highlighted the differences observed between CAO victims rescued by SPs and those not rescued by SPs. It could reflect different types of CAO with more severe accidents or more accidents limiting the victim’s mobility among CAOs rescued by SPs. It could also indicate a difference in the request of ski patrol depending on the victims.
Limitations
Our study did not include accidents that could not be identified as CAOs, collisions with another person, and noncollisions, which could change the distribution of accident scenarios. Accidents leading to a medical consultation outside ski areas or to no consultation were also not included, which might underestimate the number of mild injuries and the overall rate of injury. We did not investigate the influence of the shape of the obstacle and the type of protection on the types of injuries.
The analysis of 2 independent databases had several limits. The 2 databases shared 12 ski areas, leading to an overlap of the results; the 201,693 documented cases likely corresponded to a lower number of accidents. Working with anonymous databases prevented us from quantifying and removing the duplicates. We could not avoid this overlap without choosing one database over the other and without excluding either the mildest or the most severe accidents. The definition of some factors was also slightly different between the databases. The identification of injuries and their locations were less precisely evaluated in the SNOSM database, which could have affected the multiple and unknown injury locations. The proficiency level was biased by the self-estimation by the victim. This bias was present for both cases (CAOs) and controls (non-CAOs).
Characterization of the general population was based on visual inspection, leading to potential errors in the estimation of sex and age group of people observed. These observations were performed only in 8 ski areas, providing an approximation of the noninjured population on the slopes.
Conclusions
The CAO victims are more likely to be males, skiers, aged <26 y, and experienced than the victims of other accidents. Previous studies showed that these groups tend to exhibit risk-seeking behavior. They also tend to move at high speed, leading to high-energy accidents. The CAO victims sustain head/neck or trunk injuries more often and more frequently need a transfer with a medical helicopter, underlining the severity of these accidents. The profile of CAO victims suggests a need for dedicated public awareness campaigns to prevent these rare but often severe accidents. It also suggests a need for adequate protection devices such as paddings attached to obstacles.
Footnotes
Acknowledgments
The authors thank all the ski area doctors and all the ski patrollers who contributed to the data collection and all the people who participated in the development of the databases.
Author contributions: Study concept and design (PJA, CM, SR); data acquisition (JDL, CJ, the Association des Médecins de Montagne, the Système National d’Observation de la Sécurité en Montagne); data analysis (MD, JLM); drafting of the manuscript (MD); critical revision of the manuscript and approval of the final manuscript (all authors).
Financial/Material Support: This work was part of a PhD project financed by Domaines Skiables de France.
Disclosures: None.