
Abstract
Introduction
Skiing and snowboarding are popular winter sports with significant youth participation and inherent potential for injury. We investigated the relationship between age and injury characteristics exhibited by youth skiers and snowboarders.
Methods
In this cross-sectional study, we investigated injury characteristics among youth skiers and snowboarders at a ski resort, examining the association between age and injury type. We compared injury characteristics among young children (aged 3–6 y), school-aged children (aged 7–14 y), and older adolescents (aged 15–17 y) using

Results
Compared with snowboarding, skiing was associated with greater odds of lower extremity (adjusted odds ratio [aOR]=6.8, 95% confidence interval [CI]: 4.89, 9.47, P<0.001) and head/face/neck (aOR=1.63, 95% CI: 1.20, 2.21, P=0.002) injuries. Compared with skiing, snowboarding was associated with greater odds of upper extremity injury (aOR=5.9, 95% CI: 4.6, 7.6, P<0.001). Age group significantly affected injury mechanism (


Conclusions
Youth skiers exhibited predominately lower extremity injuries, while snowboarders exhibited predominately upper extremity injuries. Age significantly affected injury mechanism and injury diagnosis in youth skiers. Specifically, younger skiers tended to suffer more fractures and collision injuries than older youth skiers.
Introduction
Skiing and snowboarding are popular winter sports with millions of participants worldwide that have significantly grown over the last 3 decades.1,2 Skiing and snowboarding injuries have been well described and have been associated with musculoskeletal trauma, head injuries, thoracic blunt abdominal trauma, and even death. 2 -7 Children and adolescents account for 13–27% of the estimated 200 million skiers globally, 1 and 20-30% of the skier/snowboarding population in the United States. 8 In the context of these sports, age has been shown to interact with injury incidence, with higher injury incidence reported in children/adolescents relative to adults.1,8
Understanding injuries among youth winter sports athletes can help inform healthcare teams, parents, coaches, and recreationists on strategies to train, treat, and instruct to mitigate traumatic injury. While injury patterns among skiers and snowboarders have been described, age is one potential factor related to injury susceptibility, mechanism, and severity.8,9 As children grow, physiological changes occur that alter anatomy and coordination, potentially placing tendons, ligaments, or bones at risk of injury among skiers and snowboarders. Youth athletes are particularly vulnerable to musculoskeletal injury due to factors such as growth spurts and relative strength disparities between anatomic structures that change with physiologic maturity. 10 Other factors, besides those related to physiological development, could relate to injury. Maturity status, coordination, skills, ability to assess risk, and use of protective equipment, can all vary significantly as athletes age and modify injury risk or severity. 9
The purpose of our study was to investigate factors associated with different injury characteristics among youth skiers and snowboarders. Primarily, we examined the association between age and winter sports type (ski vs snowboard) with the anatomical location of the injury. We hypothesized that younger athletes would have higher rates of head injuries than older athletes due to their increased head-to-body ratios and relatively weak cervical muscles.11,12 In keeping with previous studies that report on skiing and snowboarding injuries at large,2,6,13-18 we hypothesized that youth skiers would exhibit higher proportions of lower extremity injuries than youth snowboarders and that youth snowboarders would exhibit higher proportions of upper extremity injuries than youth skiers. Here, we describe and compare injury characteristics between discrete age groups of youth skiers and snowboarders, which were divided into young children (aged 3–6 y old), school-aged children (aged 7–14 y old), and older adolescent (aged 15–17 y old) age groups. Secondarily, we examined the association between patient/injury characteristics (age, sex, sport, weight, density of other individuals skiing/snowboarding on the day of injury, snow conditions, and temperature) with the anatomical locations of injury sustained.
Methods
Study Population
This cross-sectional study was conducted at a large ski resort in Colorado during the 2012‒13 and 2016‒17 ski seasons. The study population included people under the age of 18 y injured at the ski area while skiing or snowboarding who received evaluation at the ski area clinic located at the base of the resort. Individuals injured on the mountain who were not independently mobile were brought down via toboggan by ski patrol, triaged, and transferred to the clinic for further evaluation. Those who could ski or snowboard down independently either first presented to ski patrol and were triaged similarly or presented directly to the clinic.
Only injured patients presenting to the clinic who received a diagnosis through physician evaluation and, if necessary, diagnostic tests were included. Furthermore, only patients with musculoskeletal, head trauma, or chest/abdominal injuries were included. Thus, patients with environmental injuries (such as sunburn or frostbite) or illnesses were excluded.
Data Collection
All protocols were approved by the Colorado multiple institutional review board (#13-1730). Injury information was collected from the clinic via retrospective medical chart review. For the 2012‒13 and 2015‒16 seasons, research assistants reviewed hand-written clinic notes that were scanned into a semielectronic health record system (EHR). In 2016‒17, the ski area clinic utilized a full EHR, making data available via online queries. When multiple injuries were reported, the first-listed diagnosis (the most clinically salient in the physician’s opinion) was used for analysis unless the patient sustained head trauma (excluding superficial injuries such as abrasions) or a fracture. If the patient sustained head trauma and a fracture, head trauma was included for analysis, and the fracture was marked as a secondary injury. Rarely ambiguous diagnoses were reviewed by a physician to be categorized. Each clinic patient had a medical record ID linked to the individual and an encounter ID linked to each visit, allowing researchers to exclude follow-up visits that were not the primary injury event. More information on the methodology is available elsewhere (PMID#
Some variables were categorized for analysis. Concussions, closed head injuries, or head trauma (excluding superficial injuries such as contusions, abrasions, and lacerations) were categorized as head trauma. Internal chest injuries, except for uncomplicated rib fractures, were categorized as blunt chest trauma. Internal abdominal injuries were categorized as blunt abdominal trauma. Lower leg fractures included only proximal or midshaft tibial or fibular fractures. Ankle fractures included distal tibial or fibular fractures. Tibial plateau fractures were grouped separately. Femur/thigh and hip/groin injuries were grouped as lower extremity injuries, while pelvic injuries were grouped as abdominal/thoracic injuries for analysis.
Analysis
Data were filtered and quantified in SAS V9.4 (Cary, NC). Statistical analyses were performed using Stata version 15 (StataCorp, College Station, TX), and all tests were two-sided. Before analysis, data were inspected for quality and normality. Means with standard deviations were calculated for continuous variables and frequencies and percentages for categorical variables. We compared the characteristics of skiers and snowboarders using independent samples t tests for continuous variables. For analyses of injury characteristics, skiers and snowboarders were divided into young children (aged 3–6 y old), school-aged children (aged 7–14 y old), and older adolescent (aged 15–17 y old) age groups. Age groups were chosen so patients in each age group share similar stages of physiological development and maturity that could impact their injury profiles. Chi-square analyses were used for assessing the dependence of injury characteristics with age groups of skiers or snowboarders with Bonferroni adjustment and posthoc analysis. Residuals greater than 2 in absolute value were considered significant for statistical comparison of specific population proportions. Child snowboarders were excluded from the χ2 analysis assessing the dependence of injury characteristics on age groups in snowboarders because of a lack of statistical power. We then used binary logistic regression analysis to examine the association between anatomical injury location with several predictor variables, including age, sport, sex, weight, attendance on the mountain on the day of injury, skier density on the day of injury, base snow depth, current day snow total, and temperature, which were all collected and tabulated from medical records taken at the time of injury. Statistical significance was defined as α=0.05, or for logistic regression models, a 95% confidence interval that did not cross one.
Results
We included a total of 1968 injured children and adolescents: 57% (n=1129) were injured while skiing, and 43% (n=839) were injured while snowboarding. Snowboarders had a significantly greater mean weight and age than skiers (Table 1). The proportion of snowboarders who were male was significantly higher than that of the skiers (Table 1).
Descriptive statistics and demographics for injured youth skiers and snowboarders
Continuous data are presented as mean (SD); categorical data are presented as number included (% within group).
There was a significantly greater proportion of injured snowboarders in the older adolescent age group than of injured youth skiers (Table 1). Figure 1 shows injury anatomical locations, diagnoses, and injury mechanisms for injured youth skiers and snowboarders. While the anatomical locations of injuries in youth skiers were independent of age group (


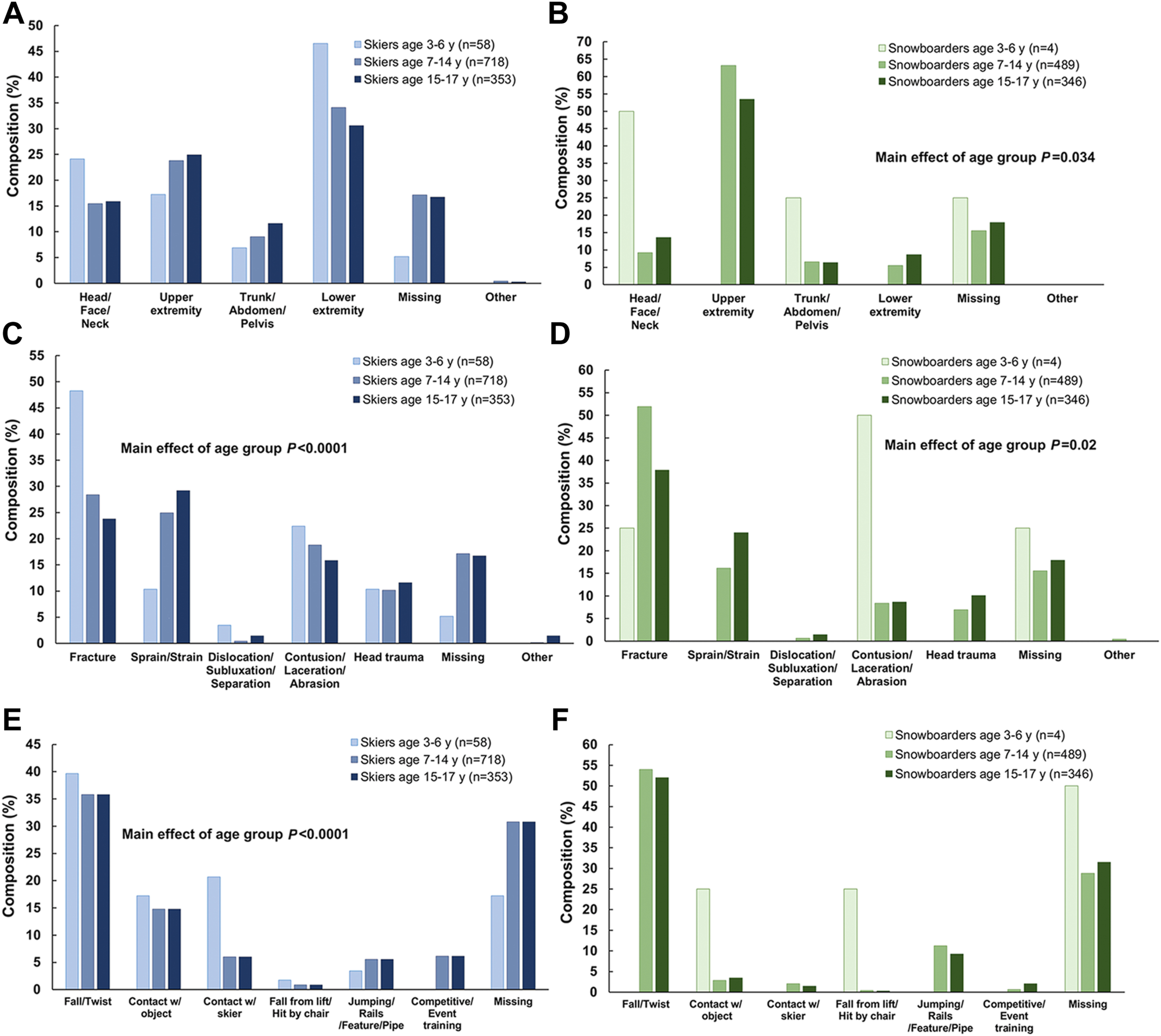
Injury anatomical locations, diagnosis, and mechanisms for age-grouped youth skiers (A, C, E) and snowboarders (B, D, F). ∗Head trauma includes concussions and closed head injuries and excludes lacerations, contusions, abrasions of the head, face, and neck.
Anatomical locations of injuries in age grouped youth skiers and snowboarders
Athlete characteristics associated with anatomical locations of injury
Bolding signifies statistical significance.
denotes P value <0.05
In youth skiers, injury diagnosis significantly depended on age group (

Injury mechanism in youth snowboarders was independent of the age group (


Discussion
The purpose of this study was to describe and compare injury characteristics between different age groups of injured youth skiers and snowboarders and evaluate factors associated with different injury locations. We observed several differences in injury characteristics between age groups of youth skiers and snowboarders, especially among youth skiers. Young child skiers had the highest rates of head injury and lower extremity injury compared with older groups of skiers. We discovered that these lower extremity injuries, which account for over half of all the injuries we observed in young child skiers, were predominately fractures that affected the lower leg, foot, and ankle. This contrasts with school-aged and older adolescent skiers who tended to suffer sprains/strain to the knees. Similarly, school-aged snowboarders also experienced significantly higher proportions of fractures than older adolescent snowboarders. Injuries to the trunk and abdomen were relatively infrequent in all age groups of skiers compared with musculoskeletal extremity injuries and head injuries.
The observation that both young child skiers and school-aged snowboarders exhibited significantly higher proportions of fractures than sprains/strains compared with their older counterparts is potentially explainable and clinically relevant. Biomechanical differences between age groups could account for increased susceptibly to fractures in younger athletes. During the first 2 decades of life, the skeleton grows in both size and density, with the growth plates of young children being particularly vulnerable to fracture.19,20 Prepuberty, bone mineralization lags behind bone length, increasing susceptibility to fractures. 20
Similarly, the hypothesis that younger child athletes would suffer higher proportions of head injuries compared with older school-aged and adolescent athletes, which was supported by our analyses of youth skiers, may be rooted in age-related physiological differences. Compared with older school-aged and adolescent athletes, young children exhibit larger head-to-body ratios with softer, more pliable bones of the cranial vault. Coupled with relatively weak cervical paraspinal muscles, this could account for an increased susceptibility to head injury compared with older athletes.6,11-25 Another factor possibly contributing to the higher proportion of head/face/neck injuries in young child skiers compared with that of older youth skiers involves a potential interaction between injury location and mechanism. We observed significantly higher proportions of collisions in young child skiers compared with those in school-aged and older adolescent skiers. Young child skiers and snowboarders may not follow a predictable direct path down the fall line, which could increase the risk of potential collisions. Such collisions are associated with the increased risk for head, neck, and face trauma observed in young child skiers, and previous studies show that such collisions are a leading external mechanism of fatal head injuries among child skiers. 26 Other factors not related to the athletes were significantly associated with different injury locations. The higher daily temperature was associated with modestly increased odds of a head/neck injury. Similarly, higher attendance was associated with modestly decreased odds of abdominal/trunk injuries.
The most common specific diagnosis for young child skiers was a fracture to the lower leg, ankle, or foot, accounting for 29% of these injured skiers (Table 4). The observation that young child skiers exhibited a higher proportion of lower leg injuries than older youth skiers conflicts with several reports that assert knee injuries are the most common site of injury in skiing.13,15,27-32 In contrast to young child skiers, sprains/strain to the knee were the most frequent specific diagnosis for older adolescent skiers (16% of injuries) and aligned strongly with these studies. School-aged skiers had a leading specific diagnosis of concussion, accounting for about 10% of their injuries, and was a top-three specific diagnosis in each age group of skiers. School-aged and older adolescent snowboarders had lower arm/wrist fractures as the leading specific diagnosis—these data align with previous research that demonstrates snowboarders are most vulnerable to wrist injuries.17,33-35
Top 5 specific injuries for age-grouped injured skiers and snowboarders, including anatomical location and diagnosis
AC, acromioclavicular; Lw, lower
Finally, our results support our hypothesis that skiing is associated with lower extremity injuries while snowboarding is associated with upper extremity injuries, aligning with the results of previous studies.6,13-15,18,27,33 The rationale behind these trends has been described extensively by Weinstein et al. 36 The difference noted is largely due to differences in equipment, overall stance, and fall mechanisms. Skiers tend to undergo more torsional forces, placing the knee at increased risk for ligamentous knee injuries, while snowboarders are more apt to fall onto an outstretched hand. 36 Interestingly, the female sex was also associated with lower extremity injuries independent of sport. In general, female athletes tend to suffer higher incidences of anterior cruciate ligament injuries than male athletes. These are extremely common in skiing, and the underlying factors contributing to this increased susceptibility in female athletes are complex and warrant further research. 37
Limitations
Although we have data on the average number of participants per skier day, one limitation of this database is that it does not include data on the number of participants per day of athletic exposure, making injury rates among skiers and snowboarders impossible to report. We lacked statistical power for injured child snowboarders and could not report on this subset of snowboarders. The low number of injured snowboarders in this age group reflects the reported demographics of snowboarders, which is dominated by adolescent males.38,39 This represents a gap in the data that could be filled with future studies, and there may be undiscovered injury patterns in young snowboarders that we could not describe. By only including one diagnosis per patient, it’s possible to underestimate the prevalence of some injuries. However, by including the first-listed diagnosis, the most clinically important injuries (in the physicians’ opinions) were evaluated. Furthermore, injuries reported to the resort clinic are inherently biased toward more severe injuries that warrant referral to the clinic. The way that injuries were categorized by anatomical location, mechanism, and type makes it difficult to assess injury severity between age groups, specifically when it came to head trauma. Thus, this report does not effectively distinguish between different severities of injuries. This report also does not address how injury characteristics interact (ie, how injury mechanism might affect injury location or type), which can be addressed in future studies using this database. This study was performed in the western United States, and injury patterns might change with different snow conditions in different geographic regions that would have different types of snow and weather. Finally, being a cross-sectional study, we are unable to make any causal inferences and only understand associations between variables.
Conclusions
This study demonstrated key differences in the injury characteristics experienced by youth skiers and snowboarders, specifically among young child skiers, and how their injury profiles differ from older school-aged and adolescent skiers. Young child skiers had the highest rates of head/neck/face injuries and lower extremity injuries compared with those of older skiers. Young child skiers also tended to suffer fractures rather than sprains/strains like older adolescent skiers. Similarly, school-aged snowboarders exhibited a significantly higher proportion of fractures than older adolescent snowboarders. As hypothesized, regardless of the age group, skiers endured lower extremity injuries more frequently than any other body part. Interestingly, in young child skiers, these lower extremity injuries predominately affected the lower leg, ankle, and foot, contrasting to older skiers who tended to suffer lower extremity injuries of the knee. As with the results of previous studies, our data associated skiing with lower extremity injuries and snowboarding with upper extremity injuries. Taken together, these data can inform how athletes, specifically young, new skiers, are trained to mitigate traumatic injury. These data may also be used to educate parents and healthcare personnel on the injuries a young skier may experience to appropriately evaluate the risks of participating in winter sports and help anticipate and treat injured children on the slopes.
Footnotes
Funding
Financial/Material Support: Unrelated to the current study, DRH has received research support from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (R03HD094560), the National Institute of Neurological Disorders and Stroke (R01NS100952 and R43NS108823), MINDSOURCE Brain Injury Network, and the Tai Foundation.
Acknowledgements
Author Contributions: study design and concept (AJP, DRH, MK, KCC); data acquisition (AJP, LAP, RDC, MK); data analysis (DRH, KCC); drafting and critical revision (AJP, DRH, KCC, MK). All authors approved the final manuscript.
Disclosures: DRH has received research support from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (R03HD094560 and R01HD108133), the National Institute of Neurological Disorders and Stroke (R01NS100952 and R43NS108823), the National Institute of Arthritis and Musculoskeletal and Skin Diseases (1R13AR080451), MINDSOURCE Brain Injury Network, the Tai Foundation, and the Colorado Clinical and Translational Sciences Institute (UL1 TR002535-05) and is a stock shareholder at the Scientific/Medical Advisory Board of Synaptek, LLC.
Previous Presentation: Presented in part at a podium presentation at the Pediatric Research in Sports Medicine annual meeting, January 28, 2022, Houston, TX.