
Abstract
Rock climbing was recognized as a sport at the 2020 Tokyo Olympics. Despite its increasing participation, there is no knowledge synthesis of head injuries (HIs), defined as any injury to the head, associated with climbing, making it challenging for clinicians to provide evidence-based care. Our aim was to synthesize HI literature within rock climbing and identify knowledge gaps. Six databases (Medline, Embase, Sports Medicine & Education Index, SPORTDiscus, CINAHL, and Cochrane) were searched. Two reviewers screened 345 studies and 31 studies were selected for data abstraction. We found the quality of individual studies mainly “fair” to “good.” Both HI and traumatic brain injury (TBI) had inconsistent definitions and categorization. The HIs represented between 0 to 36% of reported climbing injuries. Between 11 to 100% of HIs were TBIs, defined as an HI with permanent or temporary neurological sequelae. The most common causes of HIs were outdoor falls and falling objects. Climbing-specific factors associated with the causes were infrequently examined in the literature. Data sources of safety practices were incomplete. Overall, there was a lack of literature examining HIs, mechanisms of injury, and safety practices associated with climbing. To improve the tracking of HIs in climbing, we suggest the use of consistent reporting standards and the creation of a climbing injury surveillance system.
Introduction
Rock climbing has been steadily growing as a sport and debuted at the 2020 Tokyo Olympics.1,2 With the increasing participation, climbing injuries are on the rise. In the United States, climbing injuries grew approximately 10% per year between 2008 and 2016.2,3 These injuries occurred in all climbing disciplines, posing unique management challenges.4,5
There are several different forms of rock climbing disciplines. 5 In traditional and sport climbing, climbers wear a harness with an attached rope to provide safety during falls. 5 The lead climber ascends while the belayer controls the rope and maintains adequate tension in case the lead climber falls. 6 Traditional lead climbing has the lead climber placing temporary safety gear during ascent, such as cams, in natural rock as fall protection. 6 In contrast, lead climbers use anchors bolted into natural or artificial walls to clip in safety gear when sport climbing. 7 Other disciplines are bouldering and speed climbing. Bouldering, which occurs on natural rock or artificial surfaces, involves ropeless climbing on routes limited to a few meters in height with crash pads and spotters for safety. 7 Speed climbing occurs when a climber races up a predetermined artificial route alongside a competitor in a short sprint-like fashion. 8 Speed climbers are protected with an automatic belay device. Rock climbing can occur on different settings, including natural rock (outdoor) or artificial surfaces (indoor). 7
A variety of injuries occur within rock climbing.4,5,9 However, head injuries (HIs), defined as any injury occurring to the head, have not been studied to the extent of extremity injuries.4,5,9–13 Within the HI spectrum is traumatic brain injury (TBI), defined as an HI with transient or permanent neurological sequelae. 14 As TBIs are associated with morbidity when an athlete undergoes premature return to activity,15,16 national sport organizations (NSO) require concussion protocols. In fact, certain jurisdictions such as Ontario, Canada, have laws that mandate concussion protocols within NSOs.17,18 When Climbing Escalade Canada, a new NSO, was required to develop a concussion protocol, it sought clinician input. 17
Because of the limited HI literature in climbing, clinicians are challenged when developing concussion protocols, or caring for climbers with HIs. It would be useful to understand the relative distribution of HI and TBI among injured climbers, injury mechanisms, and risk factors. Our objective was to examine what is known about HI in all disciplines and settings of rock climbing to identify the knowledge gaps.
Methods
We chose the scoping review because it allowed us to examine the evidence broadly and distill it into themes. 19 We used the preferred reporting items for systematic reviews and meta-analysis extension for scoping reviews guidelines. 20
We included published outdoor or indoor rock climbing injury literature with HI data. The literature without HI data was excluded. We excluded climbing literature not involving rock climbing such as alpinism, ice climbing, or mountaineering, as well as review articles, non-English language publications, and grey literature.
Injury definitions were adapted from the International Mountaineering and Climbing Federation (UIAA). The UIAA classifies mountaineering and climbing injuries as those resulting from a mechanical external or internal force while climbing. 21 An HI was defined as injuries of the head or face. 21 Traumatic brain injury was a head injury associated with transient or permanent neurological symptoms. 14 Mild traumatic brain injury (mTBI) or concussion were TBI with a Glasgow Coma Scale (GCS) score of ≥13. 14
Six databases were searched from 1946 to July 2020: Medline, Embase, Sports Medicine & Education Index, SPORTDiscus, CINAHL, and Cochrane (Table 1). The duplicates were removed and the final search was exported into a review software Rayyan.ai (Rayyan Systems, Cambridge, MA, USA).
Search strategy
MeSH, medical subject headings; UIAA, Union Internationale des Associations d’Alpinisme
indicates a wildcard search made.
Two independent reviewers screened the studies. Eligibility was reviewed from the titles and abstracts and then all selected papers subsequently underwent full text review. The review process was unblinded after each step. To critically appraise included studies, we used the National Heart, Lung, and Blood Institute quality assessment tool. 22 A third independent reviewer resolved any disagreement after unblinding, or after critical appraisal.
Two reviewers developed a standardized data abstraction form, which was calibrated with a random sample of 5 studies through joint extraction. Afterward, the reviewers independently extracted data and discrepancies were resolved through consensus. If consensus was not reached, a third reviewer independently examined the data to provide resolution. Data charting was prospective and progressive. If the data could not be categorized in the standardized form, they were charted on a modified data abstraction form after team input.
Abstracted data included study characteristics such as sample size, demographics, data collection methods (database review, surveys), and study design. We documented HI proportions (relative to cases), HI classifications, TBI presentations, mechanism of injury (falls, falling objects), climbing discipline, and setting (inside and outside). We also collected information on safety practices such as helmet use.
We used Microsoft Excel (Microsoft, Redmond, WA, USA) for data collection and analysis. The HI proportion was presented as standard ratios. When the total case numbers were unavailable, the total number of climbers were used as a proxy measure to calculate proportions. TBI proportion was defined as the number of identifiable TBIs divided by the total number of HIs. Cohen’s Kappa was calculated to assess inter-rater agreement between the reviewers for full text selection.
Results
During study selection, a third reviewer resolved 24 screening and 9 full-text discrepancies. Given relevant findings, 3 abstracts without full text were included in our review (Figure 1). 23 –25 The inter-rater reliability of final synthesis was Cohen’s k=0.81. We critically appraised 31 papers and determined 9 were good, 15 were fair, 4 were poor, and 3 were indeterminate quality. The study descriptions are outlined in Table 2. Two studies only reviewed HI in rock climbing.23,26 Twenty-nine studies reviewed HI in addition to other injuries, such as musculoskeletal injuries.
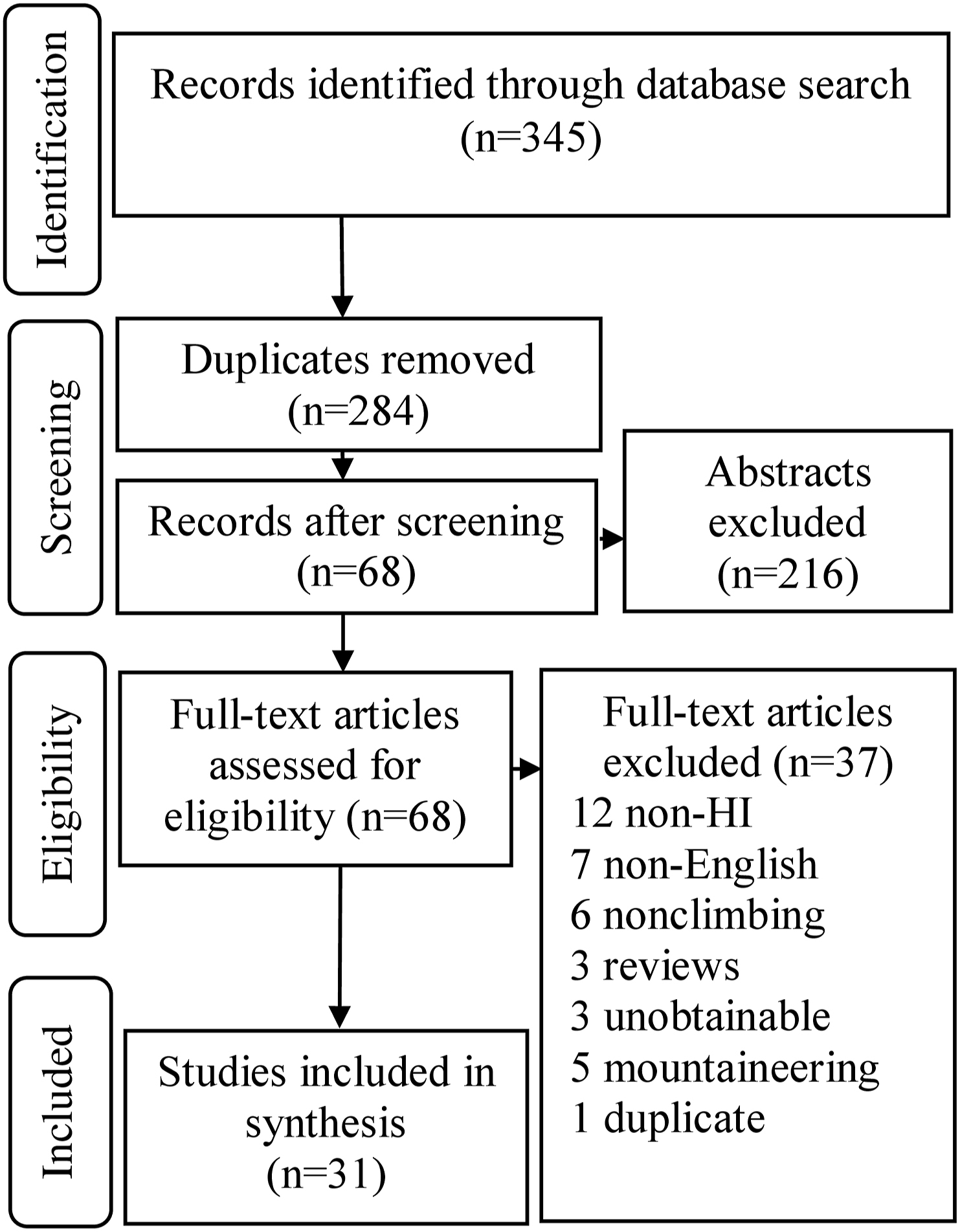
Preferred reporting items for systemic review flow diagram of study selection. HI, head injuries.
Table of results summarizing findings of studies examined in the review
ED, emergency department; HI, head injury; TBI, traumatic brain injury; OR, odds ratio; ICH, intracerebral hemorrhage; mTBI, mild traumatic brain injury; LOC, loss of consciousness; AIS, abbreviated injury scale; GCS, Glascow Coma Scale; n/a, not applicable.
Head injury only.
Head and facial injury.
Head and neck injuries.
Not specified.
Combined head neck and facial injuries. a–e Indicate the anatomical areas reported as a single injury number with head injury.
Study quality determined by the NHLBI rating tool. 22
Proportion of head injury relative to all injuries documented in the study.
The reporting of HIs was heterogeneous and incomplete. The HIs were reported in combination with injuries from different anatomical regions of the head, neck, and face (Table 2). The injuries included the following: combined head, neck, and face, combined head and neck, combined head and face, and head only. When multisystem trauma was reported, minimal description was provided, making it difficult to identify presence of HI.
Similarly, TBI data were heterogeneous and inconsistent. We found that many studies reported an mTBI without defining it.5,7,26,32,33,35,37 Although using the same registry, different studies reported different HI and TBI rates.2,26,37 There were also studies that did not differentiate HIs from TBI or minor injuries, such as a facial laceration.2,3,10,24,25,27,30,32,38,39,41,44 However, if studies reported HI with major trauma,27,30,38,39,44 high injury severity,32,41 or loss of consciousness,29,32,38 we categorized these injuries as TBIs because they fulfilled our definitions.
Among injury cases, HIs ranged between 0 (0 HI of 836 cases) and 36% (18 HI of 50 cases). Climbing TBI was between 11 and 100% of HI (Table 2).4,5,7,23,26,29,32,33,37,38,45 The mTBI was between 11 and 50% of HI.26,32,37 We found that self-reported mTBI rates were higher in survey studies.5,7
For mechanisms of injury, outdoor falls were the leading cause of HI. 26 Though >6 m (>20 ft) falls were associated with all-cause fractures and hospitalizations,2,25,37,45 the association of fall distance with HI-related morbidity is unclear. A few studies found >6 m (>20 ft) fall-related HI was associated with morbidity 26 and hospital admissions;25,26 however, others did not find any association.27,32,37,41–45 Three studies suggested there were climbing-specific protective factors during falls, such as rope elasticity, reducing overall injury.41,42,45 Studies have proposed that climbing HI was infrequent because harnesses rotate the body to a foot-first falling position.27,37,41 Consequently, studies have suggested there would be a higher risk of spine or lower limb injury in falls.27,32,37,43,44
The second mechanism for climbing HI was falling objects.23,26,37 For the setting, outdoor traditional and outdoor sport climbing had more HIs than indoor climbing.4,5 Examining the discipline, there were no discernable differences in HI rates between outdoor sport and traditional climbing.4,5,42 Although outdoor HIs were more common, occasional indoor HIs occurred,5,33,34,39 from human error at gyms 33 or competitions. 34 However, other competitions reported no HIs.28,40 There were no studies determining which indoor discipline had the most HIs.
For helmets, 8 studies reported 5% to 36% use.5,7,10,23,26,27,30,45 Helmets were regarded as beneficial;27,45 however, many studies had incomplete data.5,10,23,26,27 One study found helmets did not influence overall HI severity, but the paper concluded this was from selection bias. 27
Discussion
This review examined climbing HIs, mechanisms, discipline, settings, and safety practices. We found gaps in the literature on climbing HIs, as well as factors influencing mechanisms, such as fall distance. In a sport with increasing participation,2,3 there is a rare but serious risk of HI, which can lead to hospitalization.25,26 A better understanding of climbing HI may help development of clinical guidelines, protocols, and safety parameters.
The TBIs are important to identify since under-recognition can lead to morbidity. In the sports literature, there is evidence that TBIs have significant consequences. In boxing, severe TBI with loss of consciousness is associated with subdural hemorrhage and death.46,47 Acceleration and deceleration forces during impact can cause diffuse axonal injury leading to transient neurological symptoms. 46 There are potential links between an mTBI and neurodegenerative disease, such as chronic traumatic encephalopathy. 48 Climbing TBIs could potentially have the same morbidity and mortality as other sports.
There is evidence to suggest that climbing HI is under-recognized and under-reported, and the true incidence is unknown. Because of inconsistent data collection and categorization, climbing literature poorly differentiates between TBI or minor injuries. Although not ideal, we needed to deduce if a study was reporting a TBI with injury scores such as the HI abbreviated injury scale >2 (“moderate” severity including transient loss of consciousness >15 min). 49 The limitations of TBI data are not unique to rock climbing. Some injury registries are only able to capture sport TBIs when it is the primary diagnosis. 50 Furthermore, the diagnostic codes for sport TBIs are limited and underused. 50 Despite this, an improvement in recognition and surveillance led to the increased reporting of sport mTBI. 50
If severe or mild TBIs are not registered, TBIs would be under-reported. It is estimated that 94 to 97% of climbing deaths occur prior to emergency department arrival. 3 Severe HIs causing death would not enter the hospital or be registered. We also found that self-reported mTBI rates were higher than injury registries. This suggests that climbers with an mTBI do not seek hospital care. Sports literature has recognized the limited ability to capture the true prevalence of mTBI because the injured are less likely to seek care in a healthcare settings.50,51 Similarly, because climbers infrequently seek medical care for injuries,5,10,36 mTBI would likely be under-reported.
For mechanisms related to climbing HI, there were knowledge gaps. Studies found that falls >6 m (>20 ft) were associated with HI morbidity.23,25,26 It is unclear why longer falls were associated with morbidity as there are multiple factors that can contribute to or prevent injury, such as climber experience, human error, environment, protection placement, fall factor, or rope drag.41,42,45 We found studies stating that rockfall was a cause of HI, but no further data was provided.23,26,37 Another study described rockfall risks, such as loose holds, freeze thaw cycles, or belayer positioning. 52 The specific mechanisms of climbing falls or falling objects are out of this review’s scope, and the authors recommended that climbers consult local experts, mountaineering organizations, and climbing guides. There is an opportunity for further study by examining these factors more readily in the medical literature.
For discipline, most HIs were associated with outdoor traditional and sport climbing. However, HI risk might be related to the outdoor setting rather than the discipline. We also hypothesized that we found less HIs indoors since route-setters specifically design climbing routes to be safe. Given the lack of indoor climbing HI data, we could not make any conclusions on discipline risk.
Helmet use is standard of practice in outdoor climbing given its safety benefits. However, there is a lack of data on helmet use in climbing compared to other sports, such as skateboarding. 53 Although a few studies reported low rates of helmet use,5,27 the barriers to wearing helmets while climbing are unknown.
Overall, there is evidence of HIs and TBIs in climbing. Given the knowledge gaps, there is an opportunity improve our knowledge on HIs and climbing through further research. This would help develop guidelines for the management of climbers who have sustained HIs.
Limitations
There was a limited amount of literature on climbing HIs. To acquire as much literature as possible, we included non-peer–reviewed abstracts. These sources had greater potential for bias. For feasibility, we excluded papers in non-English, limiting data sources.
We also included studies where the primary objective was not examining HIs. Consequently, the study methods were heterogeneous, resulting in wide variation of HIs and TBIs. In addition, HI data were inconsistent or lacking detail, especially when combined with other injuries. This limited our ability to make firm conclusions.
The quality of study designs was low, with individual study execution being “good” to “fair.” Most of the studies were hypothesis-generating and used observational designs, which may predispose the risk of selection or information bias. The studies using online surveys could have recall bias. Most of studies had small sample sizes and none of the studies were powered to detect association between risk factors and HI.
Because of the knowledge gaps and limitations in the literature, there is an opportunity to improve climbing-related HI research with consistent and high-quality data, which includes climbing-specific injury mechanisms. First, the inconsistent definitions and categories could be organized though the Orchard Sports Injury and Illness Classification System (OSIICS) endorsed by the UIAA.21,54,55 The OSIICS provides consistent categorization of injury by anatomical sites, and facilitates reporting injury types, which reduces ambiguity. Applying this approach would allow for improved injury comparison in climbing literature. Secondly, to collect injury mechanism data, we suggest a rock climbing injury surveillance system, independent of alpine or trauma registries. Alpine and trauma registry diagnostic codes are not specific to sport injuries. 55 Additionally, mountaineering injuries differ from rock climbing.56,57 This surveillance system should be developed by climbing experts and researchers to capture relevant data related to climbing HI. Collected data through injury reporting forms could address current knowledge gaps examining rock climbing specific injury mechanisms, helmet use, climbing discipline, and setting. This is not a new concept. Sports such as cricket have used surveillance systems to guide injury prevention.55,58,59 Development of rock-climbing surveillance systems could guide future research efforts to improve safety standards. 58 –60
Conclusion
There are HIs in rock climbing with TBIs possibly representing a significant proportion of such injuries. The HIs from climbing were mainly outdoors and mechanisms included falls or falling objects. We found a knowledge gap on HIs from climbing and its relationship to injury mechanisms, discipline, setting, and safety practices. There is a need for continued higher quality studies. We suggest the creation of a climbing-injury surveillance system, aligned with OSIICS, to promote consistent data collection to improve climbing research.
Footnotes
Acknowledgments
Author Contributions: Study concept and design (all); acquisition of the data (JY, WA, EP); analysis of the data (JY, WA, IC, ND); drafting of the manuscript (JY, WA); critical revision of the manuscript (all); and approval of final manuscript (all).
Financial/Material Support: None.
Disclosures: Neil Dilworth and Ivy Cheng previously received personal fees for the development of concussion guidelines with Climbing Escalade Canada.