
Abstract
Herein we report an unprovoked shark attack on a scuba diver in New Caledonia. The species responsible for the attack was identified as a tiger shark (Galeocerdo cuvier), based on both the victim’s testimony and forensic examination. The victim suffered significant loss of soft tissues from one thigh, which resulted in hemorrhagic shock. Even though the event occurred at a remote location, miles away from the nearest hospital, appropriate first aid, immediate deployment of an alert system, and prompt helicopter transfer by an emergency rescue team allowed the victim to be transferred to an intensive care unit in stable condition and to undergo surgery within 4 h of being bitten. Early coverage of exposed bone was performed, followed up with negative pressure dressing, antibiotic treatment, hyperbaric oxygen therapy, and a split skin graft. In spite of the massive muscular loss incurred, the victim was able to regain her ability to walk within 6 wk of the incident. Shark attacks on scuba divers are rare and seldom reported, especially in New Caledonia.
Introduction
Shark attacks have been reported in New Caledonia (including the Loyalty Islands, Isle of Pines, Belep Islands, and uninhabited islands in the exclusive economic zone of New Caledonia) over the past 4 decades.
1
-3 The annual number of shark attacks has increased over the past 20 y, with up to 2 events reported per year. This represents a twofold rate increase relative to the last 2 decades of the 20th century.
3
Nineteen percent of documented incidents have been fatal,
3
in keeping with global rates reported by the International Shark Attack File (ISAF) maintained by the Florida Museum of Natural History (
The coral reefs and lagoons of New Caledonia have long beckoned recreational scuba divers from around the world. Attracting sharks through baiting is strictly prohibited in this country. 4 Nevertheless, shark encounters are common, especially with schools of grey reef sharks (Carcharhinus amblyrynchos) and with whitetip reef sharks (Trianodon obesus) in passes and on the external slopes of the reefs. Silvertip sharks (Carcharhinus albimarginatus), tawny nurse sharks (Nebrius ferrugineus), great hammerheads (Sphyrna mokarran), and whale sharks (Rhincodon typus) are also encountered occasionally. Species considered dangerous to humans, 1 -3 such as tiger sharks (Galeocerdo cuvier) (Figure 1), bull sharks (Carcharhinus leucas), and great white sharks (Carcharodon carcharias), are rarely encountered by recreational scuba divers in this area. 2

Tiger shark (Galeocerdo cuvier). Photo credit: Yves Lefèvre.
Clinical Case
In late December 2020, around noon, a 42-y-old female divemaster and 2 other divers undertook a reef dive in a remote spot of the western coast of New Caledonia, located 160 km north from the main town, Nouméa. Scuba divers rarely frequent this site because it is not readily accessible. Earlier on the same day, another boat unsuccessfully tried trolling for fish in the same area. The fisherman eventually speared a parrotfish but chose to leave the spot because inquisitive reef sharks, assumed to be grey reef sharks (Carcharhinus amblyrynchos), were seen in the area.
The 3 divers took 5 min to descend a coral reef wall to 36 m (118 ft) depth. Surface water temperature was 26°C (79°F) according to local weather records and is assumed to have been 24°C (75°F) at a depth of 36 m (118 ft). The divers left the wall and swam away into open water, aiming to reach a rock and coral formation a short distance from the main reef. Visibility was around 15 m (49 ft). The divemaster led, while the 2 other divers followed her roughly 10 m (33 ft) behind. She was wearing a black wetsuit, black buoyancy control device, pink mask, gray fins, and no jewelry. A large shark swam into the area suddenly approaching the divemaster from the below and behind, bit her on her left thigh, and went away as abruptly as it had appeared. Profusely bleeding from a deep wound on the injured limb, the divemaster was assisted on her ascent by one of the other divers. No decompression stop was taken, nor was one necessary, as the dive had just started when the accident occurred. The injured diver was pulled out of the water and lifted aboard the dive boat, and an alert was launched 10 min after the incident. A makeshift wound dressing was applied to reduce the bleeding by another diver, who happened to be a medical doctor. The lesion extended high into the gluteal region, preventing the application of a tourniquet as it would have had to be positioned over exposed muscle and bone. Upon reaching the shore, 40 min after the bite, care of the patient was transferred to firefighters and an intensive care anesthetist who was present on site. The patient was immediately transferred to the local medical center. She reached the local medical center less than 1 h after she had been bitten. She was clinically assessed to be in hemorrhagic shock. Vascular repletion with 1 L of crystalloid was initiated along with morphine (7 mg), ketamine (10 mg), and midazolam (1 mg) analgesia intravenously, and oxygen 15 L·min-1 (high flow mask). The helicopter emergency rescue team arriving from the New Caledonia Territorial Hospital, located in Nouméa, landed 85 min after the bite. Two units of packed red blood cells were infused, as well as an antibiotic (amoxicillin-clavulanic acid 2 g/200 mg) and an anti-fibrinolytic drug (tranexamic acid, 1 g). Vascular repletion with crystalloids and analgesia (4 mg of midazolam, 20 mg of ketamine, given as boluses, along with a continuous infusion of 20 mg intravenous morphine hydrochloride) were administrated during the 45 min flight to Nouméa to stabilize the patient. On arrival at the intensive care department of the New Caledonia Territorial Hospital, 2.5 h after the bite, the injured diver remained hemodynamically stable (with blood pressure 88/65 mm Hg and pulse rate 92 beats·min-1 under continuous noninvasive monitoring), but with acute anemia (hemoglobin was 6.4 g·dL-1). She remained conscious, and her pain was under control. A CT arteriogram was performed to assess bone, soft tissue, and vascular damage. A soft tissue lesion on the CT scan showed a 33 cm wide defect in the lateral aspect of the thigh. The soft tissue had been stripped from the femur over a 20 cm stretch without fracturing the bone nor damaging any of the main blood vessels. A certified hyperbaric physician confirmed that no therapeutic recompression was required, according to the French government decompression table. 5
The patient underwent general anesthesia and was transferred to the operating room approximately 4 h after the bite. She received 4 more units of packed red blood cells along with 2 units of fresh frozen plasma, 1 unit of platelet concentrate, and 1.5 g of fibrinogen and was infused with norepinephrine 2 mg·h-1 via a syringe driver pump. The lesion consisted of lacerations of the lateral aspect of the thigh, extending over 33 cm, with complete stripping of soft tissue over a length of 20 cm over the femur, including iliotibial tract, the lower portion of the gluteus medius, vastus lateralis, the upper two-thirds of the vastus intermedius, and one-half of the biceps femoris. Perforating branches of the femoral artery were ligatured. No damage to the common femoral artery was seen. The sciatic nerve was exposed without damage. After debridement, the femur was exposed over the 20 cm (8 in) affected area. Local rotation flaps of lacerated muscle and a biceps femoris split were used to cover bone exposition.
The patient was subsequently treated with a negative pressure dressing. She received amoxicillin-clavulanic acid, 2 g/200 mg 3 times a day, and gentamycin 160 mg daily, as a prophylactic antibiotic treatment. Wound swabs at Day 4 showed contamination with Pseudomonas aeruginosa, Klebsiella aerogenes, and Shewanella putrefasciens. Tazocilline (piperacillin and tazobactam) treatment was initiated at 20 g daily for 14 d due to the persistence of positive P aeruginosa swab at Day 10 postoperatively. In addition, she underwent 16 sessions of hyperbaric oxygen therapy (2.5 atm for 90 min) to potentiate antibiotic against P aeruginosa, protect the skin graft, and mitigate the risk of anaerobic soft-tissue infections. The patient remained contaminated with P aeruginosa until Day 30, when a split skin graft was performed, allowing for discharge from the hospital after 6 wk. Functional recovery was good in the early stages, allowing for knee extension against gravity and weight-bearing with a walking frame at the time of discharge to a rehabilitation center. Three months after the accident, the patient was able to walk up to 10 min at a time without aid.
Forensic examination of the wetsuit the victim was wearing at the time of the attack was conducted a few days after the incident. Both upper and lower jaws of the animal made arc-shaped, single, clear, sharp cuts without any shredding that were fully symmetrical (Figure 2). These findings are consistent with a bite from a tiger shark Galeocerco cuvier, whose teeth are similarly shaped and evenly spaced in both jaws. The diameter of the bite was estimated to be 33 cm (13 in), consistent with the data from the CT scout view of the CT arteriogram (Figure 3). The shark’s size was estimated to be approximately 4 m (13 ft) in length. This matched the description given by the victim, who stated she spotted a 4 m (13 ft) tiger shark swimming away from her immediately after she was bitten. Later examination of photographs of the wound confirmed the identification. Photographs of the wound were taken 4.5 mo after the bite (Figure 4A and 4B). Sharp, clean cuts are still visible on both edges of the wound scar, which are a hallmark of tiger shark bites. 6

Wetsuit worn by the victim at the time of the attack. Photo credit: Claude Maillaud.
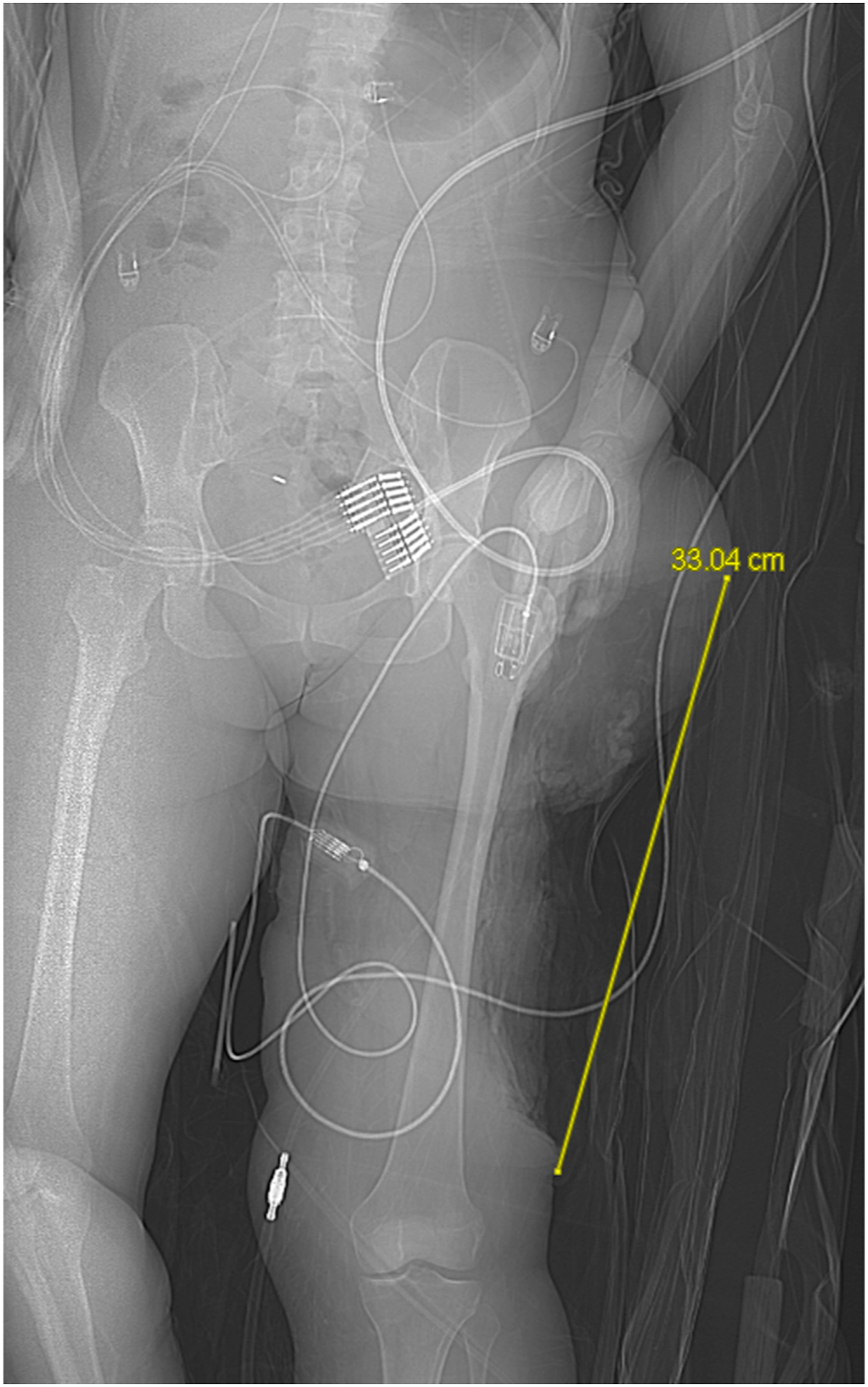
CT scout view of the CT arteriogram of the wound. Photo credit: Joseph Fournier.
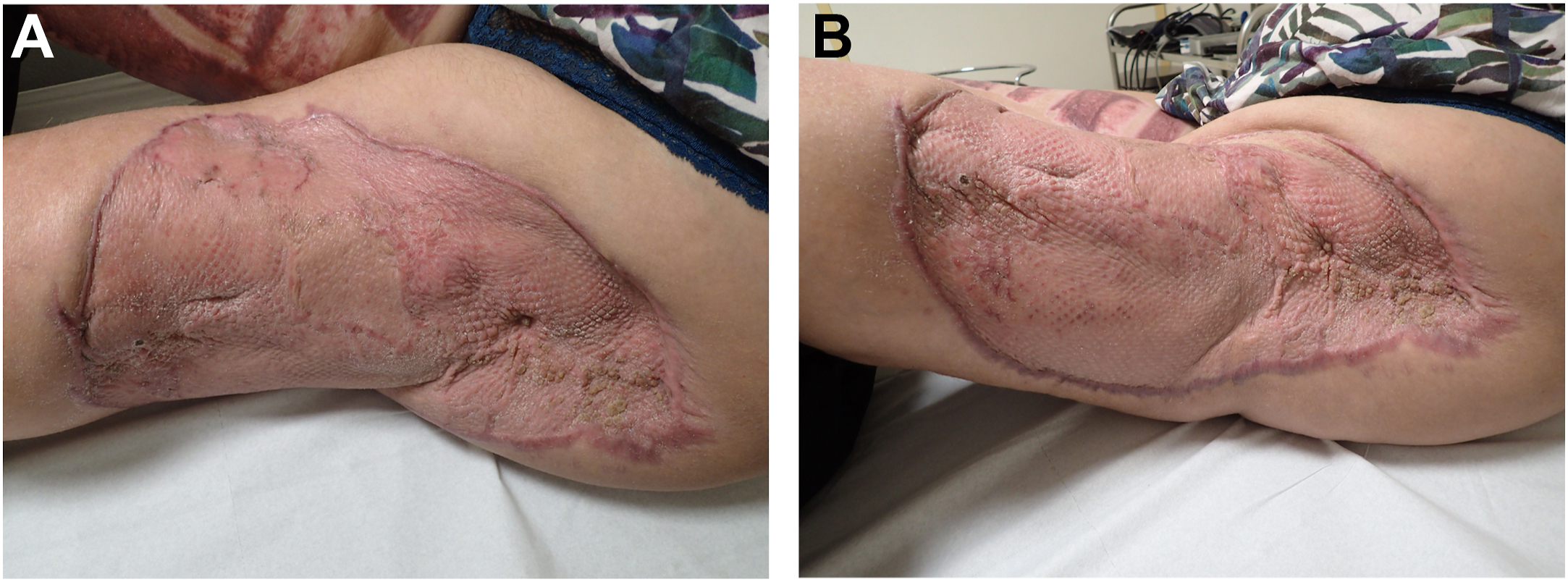
Front (A) and back (B) views of the wound scar. Photo credit: Claude Maillaud.
The case was recorded in the ISAF as No. 6610.
Discussion
Unprovoked shark attacks on scuba divers are considered unusual events.7,8 From 1954 to 2020, the International Shark Attack File recorded 2753 confirmed unprovoked shark attacks worldwide, including those on divers. Over the same period, there were 106 confirmed unprovoked shark attacks on scuba and hookah divers worldwide. Scuba and hookah divers account for only 4% of the victims. Of the 2753 cases, 284 were fatal. An additional 43 cases where the body was not recovered but sharks were implicated were confirmed by witness or gear recovered. Twelve percent of confirmed unprovoked shark attacks occurring between 1954 and 2020 were lethal. By comparison, 21 of the 106 confirmed unprovoked shark attacks on divers (20%) were lethal.
White sharks (Carcharodon carcharias) were involved in 30 confirmed unprovoked attacks on divers. Eight of these were fatal. Thirteen of these occurred in North America, while 11 occurred in Australia. Five attacks on divers are ascribed to the oceanic whitetip shark (Carcharhinus longimanus), 1 of which was fatal. All were reported from Egypt (at the same Marsa Alam location) in 2009 and 2018. Tiger sharks (Galeocerdo cuvier) have been responsible for 8 attacks on divers between 1990 to 2020, 3 of which were fatal. Those cases were recorded in Mexico (n=2, both lethal, at the same Santa Rosa reef, on Isla Cozumel), Western Australia (n=2, including the hookah diver case), Central America (n=2, Panama, Costa Rica), and Pacific Ocean islands (n=2: Fiji, Guam). None have been reported from the French Pacific islands. Fifteen other species have been implicated in confirmed unprovoked shark attacks on scuba and hookah divers. These include bites by grey reef sharks (Carcharhinus amblyrynchos) (5 cases) and the wobbegong (Orectolobus spp) (6 cases, all recorded in Australia).
The primary concern associated with shark bites is blood loss due to blood vessel damage. The relationship between prognosis and the major vessels severed was summarized by the Durban classification. 9 “Beach treatment,” using “Feinberg packs”—emergency packs that allow beach rescuers to provide early primary care to victims, as they contain vascular filling solutions, intravenous infusion sets, morphine and norepinephrine vials, wound dressing, antiseptics, and tourniquets—were promoted in areas of the Natal Coast (Republic of South Africa) where shark attacks were prevalent. 9 More recently, a shark-induced trauma scale was introduced, which scores several factors such as patient’s blood pressure, location of the injury, functional impairment from the injury, and complexity of the treatment required and allows for a determination of the level of the injury to predict prognosis. 10 Nevertheless, based on our experience in shark attack management in New Caledonia, we consider that time elapsed before the victim is given first aid is the most influential factor. The country’s main island is 400 km long and 50 km wide; the total length of the coastline is around 3400 km, and the coral reef extends 8000 km2. The New Caledonia Territorial Hospital is located in Nouméa, at the southern extremity of the main island. It has the only aeromedical emergency rescue team in the country, and it serves the main island and the 4 Loyalty Islands, 180 km away from Nouméa. Thus, for a victim with hemorrhagic wounds, the time elapsed between the onset of the bite and access to an emergency medical rescue team and/or an intensive care unit is crucial; moreover, as shown in this particular case as well as in a previous case, 11 tiger shark bites can result in a hemodynamic shock without any of the major arteries being severed. In this case, the appropriate deployment of first aid supervised by a medical professional and the immediate launch of the alert system allowed a helicoptered emergency rescue team carrying red blood cells to reach the victim within 1 h of being contacted. This made it possible for the victim to reach the intensive care department with ameliorated hemorrhagic shock despite the severity of her wound.
Notwithstanding extensive muscular damage, the patient’s ambulatory function appears well preserved. This is likely a consequence of the lack of vascular or nerve injury from the bite. Early management and coverage of exposed bone, along with negative pressure dressing, antibiotic treatment, and hyperbaric oxygen therapy, resulted in an adequate split skin graft result, despite contamination. Expert advice was sought regarding the use of latissimus dorsi free flaps, which would have necessitated transfer to an off-island referral center, but the patient elected to have treatment in New Caledonia.
Conclusion
Although rare, tiger shark attacks can lead to life-threatening injuries, where exsanguination from blunt trauma can lead to death. Scuba divers are seldom at risk of such accidents. In the case reported here, first aid and resuscitation, followed by prompt intensive care prior to early surgery, ensured the victim’s survival, despite the severity of the wound. The functional prognosis was jeopardized by muscular loss. Early management of the wound followed by skin graft made it possible for the patient to walk 6 w after the attack.
Footnotes
Acknowledgements
Author Contributions: Data acquisition (all authors); data analysis (CM, PT, TB); drafting of the manuscript (CM, JF, ALG); critical revision of the manuscript (all authors); approval of final manuscript (all authors).
Financial/Material Support: None.
Disclosures: None.