
Abstract
The purpose of this report is to describe a case of urticarial dermatitis, or erucism, caused by the white flannel moth caterpillar (Norape ovina) in central Virginia. Many caterpillars are known to cause erucism, with the puss caterpillar (Megalopyge opercularis) being the most reported culprit in the United States. White flannel moth caterpillars are expected to cause erucism as they belong to the same family as the puss caterpillar (Megalopygidae) and have similar venom-containing hairs, but no reports of the reaction or clinical course have been documented in the medical literature. A subject was stung by a white flannel moth caterpillar after it fell on his neck while clearing brush with a machete. The subject experienced immediate pain and developed a raised, erythematous rash where the caterpillar had fallen. The rash, referred to as erucism, was painful for 1 d and improved slowly over the course of 2 wk, but a small area of discoloration remained 2.5 mo after contact. Symptoms were managed by the subject at home and no medications were administered. The white flannel moth caterpillar inflicts erucism similar to that caused by the more commonly mentioned puss caterpillar. If only local symptoms are sustained from contact with a white flannel moth caterpillar, it can be safely and effectively managed with over-the-counter medications similar to the management for erucism induced by other caterpillar species. Irrigation and removal of urticating hairs with adhesive tape may help reduce the pain and is recommended, though not performed in this case.
Introduction
Caterpillars are the larval stage of moths and butterflies belonging to the order Lepidoptera. There are over 50 species of caterpillars, referred to as stinging caterpillars, that are considered toxic and have urticating hairs that secrete venom when broken or placed under pressure. 1 This venom is irritating to humans and can cause a painful, local urticarial dermatitis known as erucism. Systemic symptoms, referred to as Lepidopterism, include diffuse urticaria, headache, nausea, vomiting, and wheezing. 2 The exact makeup of caterpillar venom is not known, but it does contain peptides, hyaluronidase, phospholipase A, and a histamine-releasing substance. 2 The puss caterpillar (Megalopyge opercularis) is the venomous caterpillar most reported to cause erucism in humans with over 3,000 cases reported to a Texas poison center from 2000 to 2016. 3 Though several other species of caterpillars in North America are known to cause erucism (Table 1), reports of human encounters with them are not common in the literature.
Scientific classification of a select North/South American caterpillars known to have urticating hairs
The white flannel moth caterpillar (Norape ovina) is a type of caterpillar native to North America that ranges from Washington, DC to Missouri and south to Florida and Texas. 4 While the adult moth is white, the caterpillar is yellow, black, and red with 11 pairs of yellow spots from which arise clusters of short needle-like urticarial hairs or spines (Figure 1). Because it is in the same family (Megalopygidae) as the puss caterpillar and has urticating hairs, it is thought to cause similar symptoms as the puss caterpillar, although there are no human reports of an encounter with a white flannel moth caterpillar. We report the first case in the literature of a human exposure to a while flannel moth caterpillar resulting in erucism to illustrate the similarities in treatment to other Megalopydigae caterpillar encounters.

White flannel moth caterpillar (Norape ovina). Original photograph by Nathan Charlton.
Case Report
One summer in central Virginia, a 43-y-old male was riding a lawn mower while clearing brush under a tree with a machete. As he was cutting overhead branches, he felt a severe, searing pain on the left side of his neck. Initially, he thought that he had been poked by a branch, but when he reached up to brush off his neck, a caterpillar fell onto the lawn mower (Figure 1). He felt pain on his hands immediately after brushing off the caterpillar but that soon subsided after 2 min and no rash developed. The severe pain on his neck lasted 40 min, but a constant burning persisted for 1 d following the sting. He reported the sting feeling more severe than a bee sting but less severe than a previous caterpillar sting from a buck moth caterpillar (Hemileuca maia).
A wheal surrounded by erythema developed on the neck at the site of caterpillar contact. Progression of the rash is documented in Figure 2. A slight skin discoloration remained 2.5 mo after the sting with no associated symptoms. The subject did not seek any medical care and did not use any pain medication or antihistamines. He did not irrigate or decontaminate the site of contact with the caterpillar. No systemic symptoms or clinically significant long-term sequalae were reported.
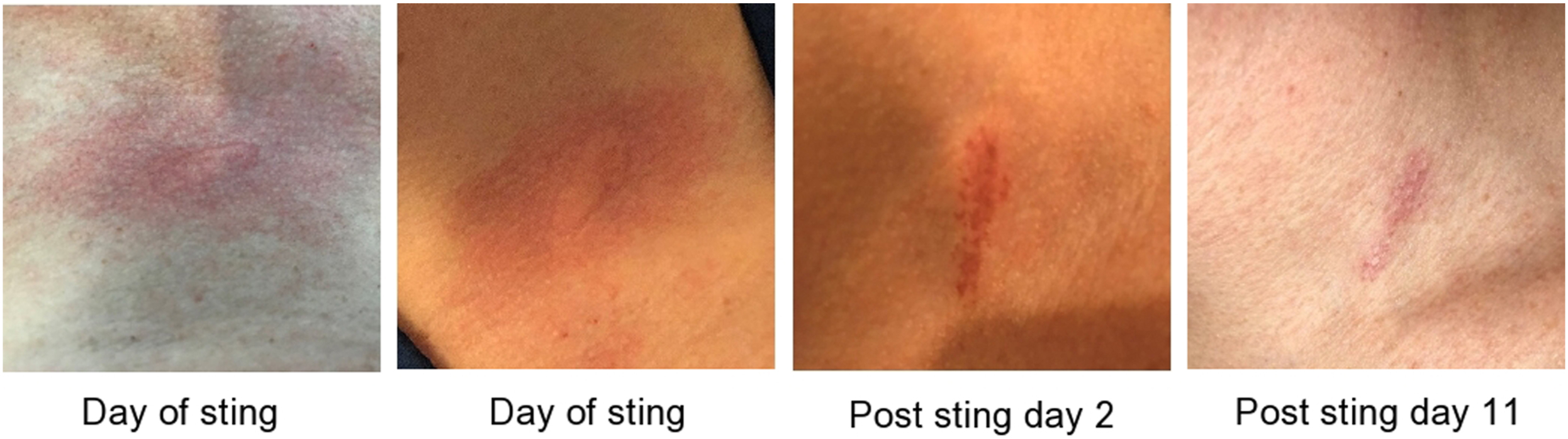
Progression of rash caused by white flannel moth caterpillar sting (Norape ovina). Original photographs by Nathan Charlton.
Discussion
True stinging caterpillars are known to cause severe pain and cutaneous symptoms upon contact with their urticating hairs. While systemic symptoms or anaphylaxis can occur after a caterpillar sting, the most common reaction is local pain and a rash at the site of contact. 3 While erucism from the puss caterpillar (M opercularis) is the most commonly reported in the literature, this is the first reported case of such induced by the white flannel moth caterpillar (N orvina). The erucism in this case caused less severe pain when compared to the sting of a buck moth caterpillar (H maia); however, the skin discoloration persisted for months before eventually subsiding.
Caterpillars are thought to cause skin irritation and pain through multiple different mechanisms. Urticating hairs can cause dermatitis through direct irritation or from venom associated with the hair. 5 Contact with nonvenomous urticating hairs (setae) in caterpillars results in delayed local itching, swelling, and erythema from local irritation and inflammation. 5 Although few data are available, the symptoms likely take longer to develop than the symptoms from a venomous caterpillar sting. Stings from true venomous caterpillars result in immediate local symptoms within minutes including pain, erythema, and swelling secondary to venom components deposited when the hair breaks the host’s skin.1,5,6 The immediate pain caused in this case supports the presence of venom in the hairs of the white flannel moth caterpillar.
General treatment of caterpillar stings includes decontamination of the urticating hairs with adhesive tape and irrigation in addition to symptom control with medications such as ibuprofen, acetaminophen, topical corticosteroids, and antihistamines. 1 -3 The majority of North American puss caterpillar stings reported to poison centers are managed at home. 3 If symptoms are severe enough and the patient presents to the hospital, parental analgesics may be required for pain control. One study in South America found that local injections of lidocaine may also quickly alleviate severe pain. 6 Although there is an antivenom for the dangerous Lonomia obliqua caterpillar found in South America, which can cause life threatening coagulopathy, none exists for North American caterpillars. 7 Systemic Lepidopterism and anaphylaxis are less common than the localized dermatitis seen in this case, but it is pertinent to monitor for symptoms after an encounter and seek medical care immediately if symptoms arise.2,8
Conclusions
Although this is only a single case, the limited local dermatitis suggests that symptoms from an encounter with a white flannel moth caterpillar (N ovina) are similar to those from the puss caterpillar and the expectation is that symptoms can also be safely managed at home. No interventions were performed in this case, but removal of the caterpillar hairs with adhesive tape is recommended and may have helped to decrease the duration of pain and skin discoloration in this case. The patient should be monitored for systemic symptoms or allergic reaction and additional guidance could be obtained from a local poison center or primary care provider.
Footnotes
Acknowledgements
Author Contributions: Study concept and design (AEM, NPC); drafting and critical revision of the manuscript (AEM, RJC, EPH, NPC); photography (NPC); approval of final manuscript (all authors).
Financial/Material Support: None.
Disclosures: None.