
Abstract
Introduction
Ocean rowing is an extreme ultraendurance sport in which athletes push themselves to their mental and physical limits while rowing across an ocean. Limited academic attention has meant health issues facing this population are poorly understood. This report provides a descriptive analysis of the injuries and illnesses encountered by ocean rowers at sea and suggests potential preventative measures.
Methods
Retrospective self-reported data were collected from ocean rowers via an online 29-question survey, classified by medical system, and totaled to produce a report of the most frequently encountered symptoms.
Results
Seventy-one ocean rowers, accounting for 86 ocean rowing attempts, completed the survey. Dermatologic symptoms formed 52% (n=169) of all reported issues, followed by musculoskeletal injuries (14%; n=45), mental health symptoms (11%; n=36), gastrointestinal symptoms (5%; n=16), and neurologic symptoms (2%). Gluteal pressure sores were the most common dermatologic symptoms (24%; n=40), hallucinations the most common mental health symptoms (69%; n=25), hand and finger issues the most reported musculoskeletal problems (36%; n=16); vomiting (38%) and headaches (50%) were the most common gastrointestinal and neurologic issues, respectively. Seasickness was reported in 42% of expeditions (n=33).
Conclusions
This report presents the physiological, mental, and medical challenges facing ocean rowers. Dermatologic and musculoskeletal issues were most common and varied greatly in severity. Over 90% of reported infections occurred as a dermatologic complaint, demonstrating the importance of preventative measures such as hygiene and wound care. Continued work with a larger population is required to further understand the physiological stress and medical complaints associated with transoceanic rowing.
Introduction
Ocean rowing is a burgeoning sport where athletes row unsupported across an ocean, encountering some of the world’s harshest and most unpredictable environments. Participants row in teams or solo across the Indian, Pacific, and Atlantic oceans, living isolated for months while facing unique physical and mental challenges.
Ultraendurance events are emerging from the fringes of sporting endeavor, with the founding of ultraendurance races increasing public awareness and participation.1,2 Ocean rowing is an extreme ultraendurance event, with expeditions lasting weeks or months, far longer than the 6 h generally considered to mark ultraendurance. 3 For those rowing in teams, individual shift patterns can be 2 h on, 2 h off, 1 with each crew member rowing for 12 h in every 24, whereas solo rowers average 10.3±1.1 h. 1 These athletes live and row in specially designed boats, carrying all supplies needed to survive for months at sea. Should rescue or assistance be necessary, emergency beacons and satellite phones provide means to access help.
As this sport’s popularity grows, so must our understanding of the medical challenges involved. Previous research largely focused on individual case studies 4 -7 or small sample sizes, 1 ranging from nonfreezing cold injuries experienced by long-distance polar rowers 5 to physiological changes, 4 physical and psychological experiences, 6 and nutrition. 7 Only 1 study has examined the spectrum of medical issues encountered during a transatlantic race. 1 In contrast, extensive research highlights the common injuries experienced in sailing,8,9 river rowing,10,11 and kayaking/canoeing. 12
This report’s main objectives are to further introduce the wilderness medical community to the growing ultraendurance sport of ocean rowing and provide a descriptive analysis of the medical conditions these rowers face.
Methods
Approval was gained from the King’s College London’s research and ethics committee before data collection for this retrospective descriptive study (reference LRU-19/20-14601).
The Ocean Rowing Society Facebook page is a platform where ocean rowers share knowledge and experience with individuals planning transoceanic crossings. Information on study objectives, use of personal data, and risks of participation (including publication of potentially identifiable information) was made available to page members with the online questionnaire.
Additionally, 88 ocean rowers who had recently attempted an ocean crossing, either as part of a transatlantic race or a publicized independent expedition, were contacted directly via their public expedition email addresses and social media. Only 1 attempt to make contact via email and social media was permitted per rower. As part of the questionnaire, consent was obtained from all participants before completing the survey. All data collected were anonymized and response order randomized to avoid participant identification via date of rower contact and order of survey completion.
Participants completed an online 29-question SurveyMonkey questionnaire covering demographics, weight loss, medical history, medical issues faced at sea and the impact these issues had on their expedition, help sought from external medical teams, medications used, and problems persisting 3 mo post-row.
Data were categorized by medical system and cumulative totals produced, allowing for disease pattern analysis and a descriptive report of common medical issues. Where a participant had completed multiple ocean rows, with no indication allowing for specific row analysis, their data were omitted. Data are presented both graphically and as a total incidence or intracategory percentage, alongside the total frequency where n>10. Where averages were determined, results are noted as mean±SD.
Results
Approximately 70% of responses resulted from direct messaging with rowers or their team. Remaining responses were gathered from the Ocean Rowing Society Facebook page.
Participant and general ocean rowing demographics are presented in Table 1. Data covered 71 rowers aged 37±12 y, reporting on 86 ocean rowing attempts. Most participants were male (58%, n=41) and competing in a race. Time at sea ranged from 2 to 92 d with an average of 46±18 d, and the Atlantic was the most rowed ocean. Body weight changes indicated a loss of 12±6 kg. The majority rowed either as teams of 4 (34%; n=29), in pairs (27%; n=23), or solo (16%; n=14), with the rest in teams of various sizes ranging from 3- to 14-person boats.
Participant and ocean rowing demographics
Eight expeditions were excluded owing to participant errors completing the survey, leaving a total of 78. Eight medical categories were noted from the 323 reported medical issues. Dermatologic problems were the most common, accounting for 52% of the total issues reported (n=169), whereas acute traumatic injuries were the least common (1%).
Specific breakdowns of each category are seen in Figures 1 to 3. An average of 2 dermatologic issues per expedition were reported, with gluteal pressure sores and salt sores/chafing/rashes each affecting over half of all rowers (24% [n=40] and 23% [n=39] of all dermatologic cases, respectively). Blisters accounted for 17% (n=29), infections 14% (n=23), cuts/bruises 10% (n=17), and sunburn 9% (n=15), Figure 1.
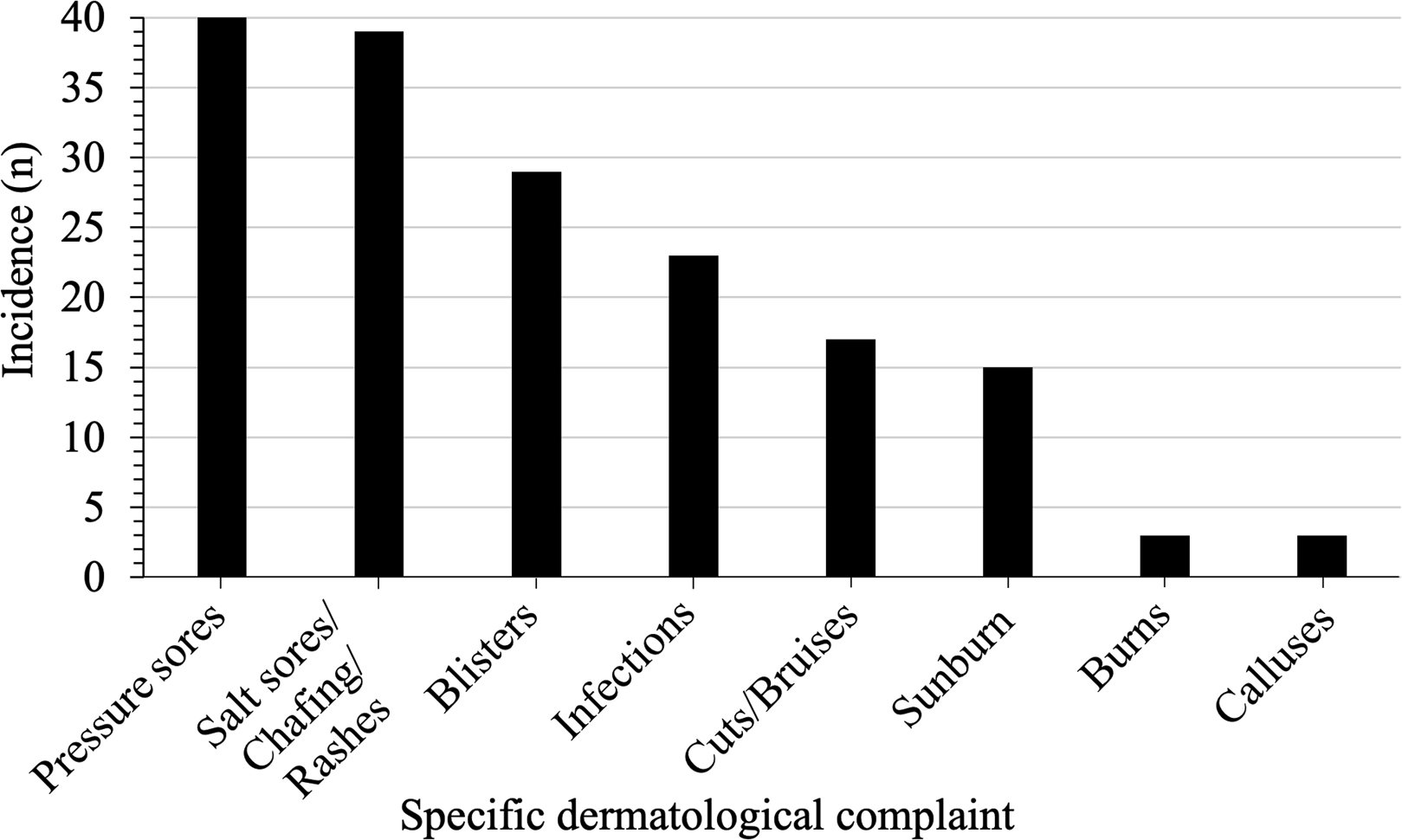
The 169 dermatologic issues experienced by ocean rowers are broken down into 8 subcategories of specific complaints.
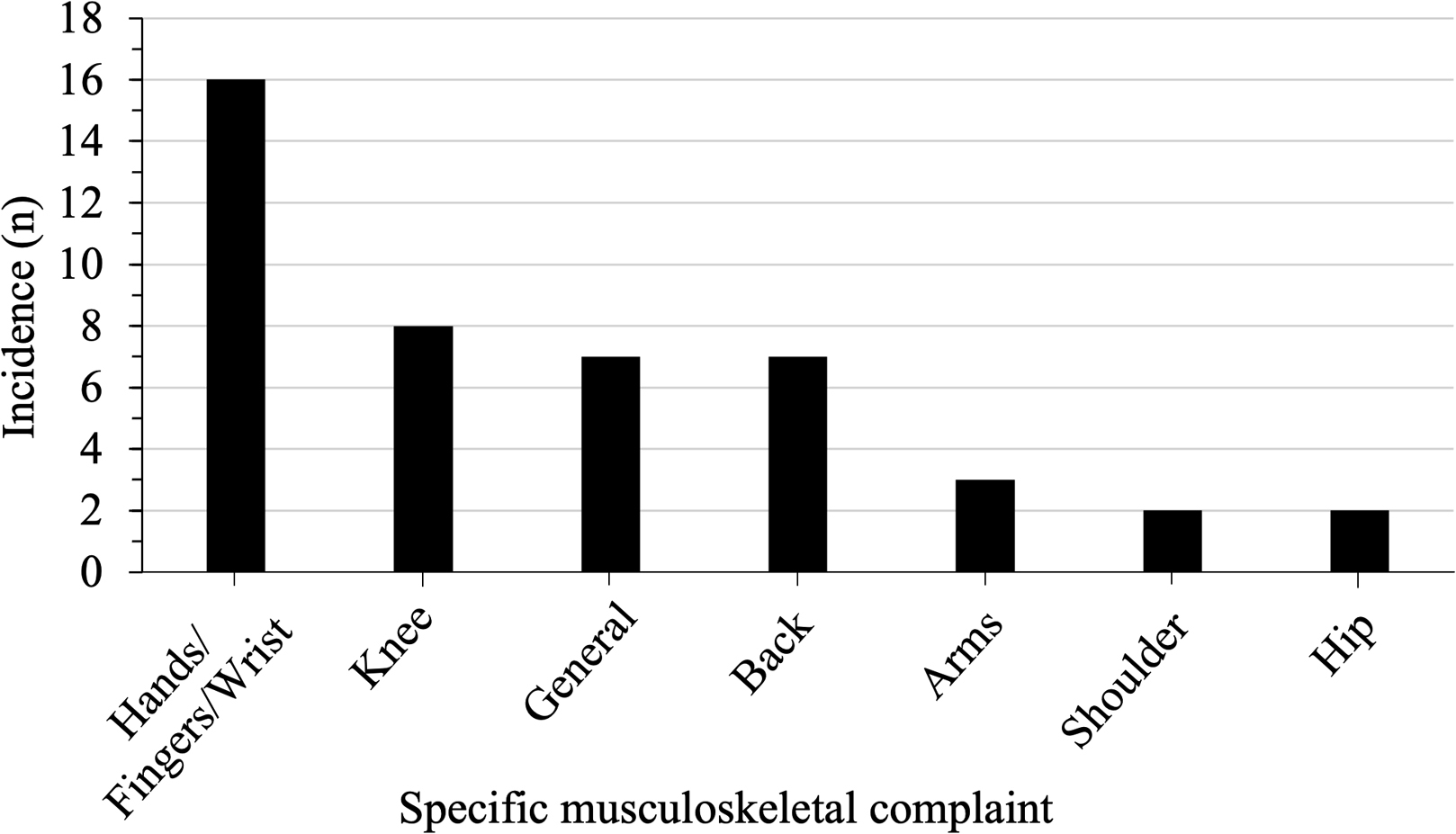
The 45 musculoskeletal self-reported issues could be further grouped into 7 main types. The category specific for general musculoskeletal issues refers to a generalized pain in most joints or muscle groups.
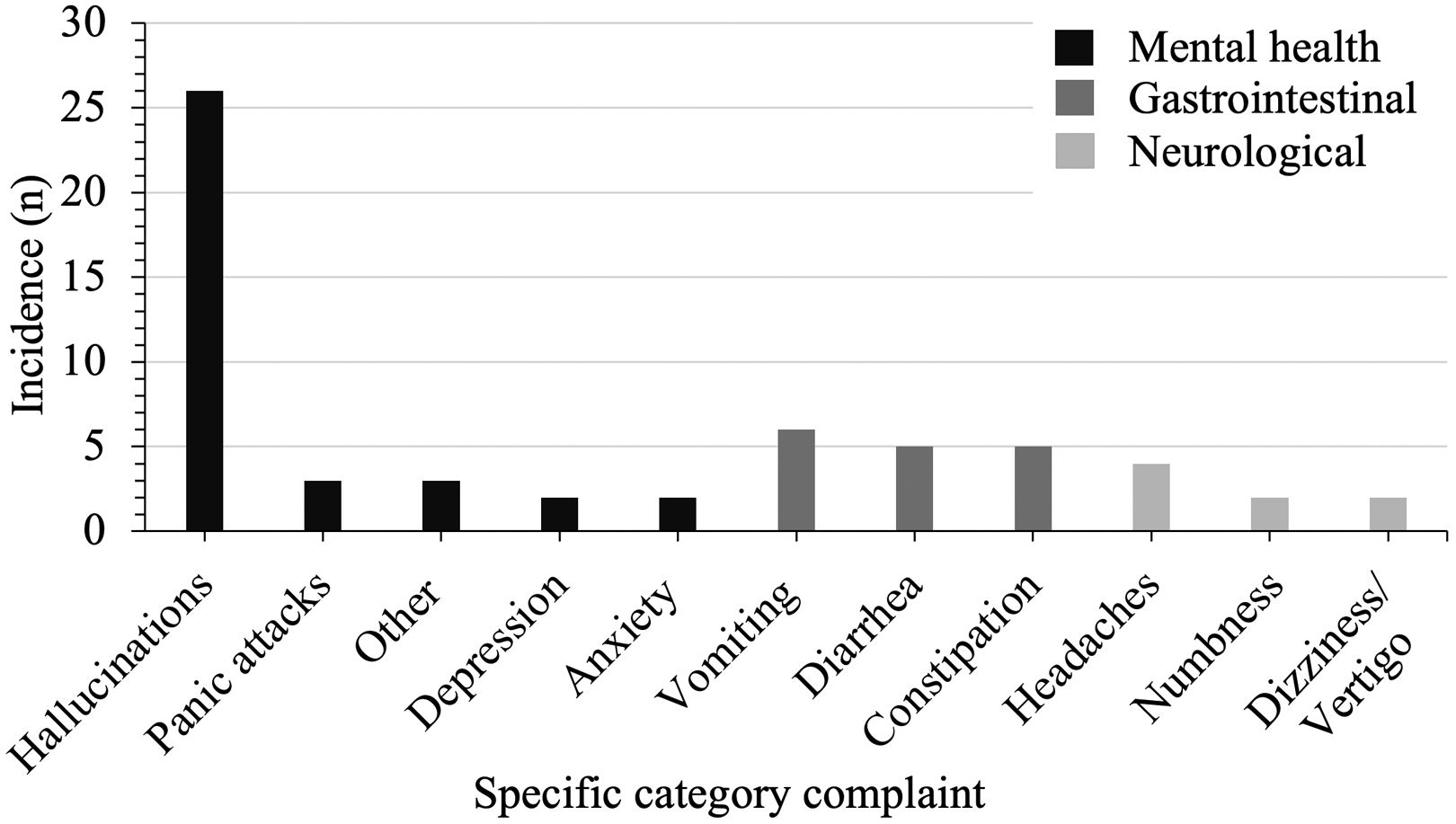
Thirty-six mental health self-reported issues were subcategorized into 5 specific issues, and 16 gastrointestinal and 8 neurologic complaints were differentiated into 3 specific categories, respectively.
Musculoskeletal problems (Figure 2) encompassed injuries to muscle groups or joints, equating to 14% (n=45) of reported issues, with over half of all rowers affected. Hand/Finger/Wrist symptoms represented 36% (n=16) of cases, knee issues 18%, both back and general musculoskeletal complaints 16%, arm pain 7%, and shoulder and hip pain 4% each.
Mental health issues encompassed 11% (n=36) of all reported complaints, present in 46% of expeditions (Figure 3). Hallucinations were the most common symptom reported (72%; n=26), affecting 32% of expeditions. Panic attacks accounted for 8% of cases, and anxiety and depression each comprised 6%. The remaining 8% were symptoms noncompatible with these subsections and therefore listed as “other.”
Seasickness affected 42% of expeditions, representing 10% (n=33) of total medical complaints. Gastrointestinal issues were less common (5% overall; n=16), consisting of vomiting (38%), diarrhea (31%), and constipation (31%) (Figure 3). Neurologic cases accounted for 2% of total issues reported, composed of headaches (50%), specific limb numbness (25%), and dizziness/vertigo (25%) (Figure 3). Four injuries fell into the acute trauma category, including substantial ligament damage, broken bones, and trauma to the face/eye, mainly due to capsizes. Remaining health issues not categorized are classed under “other,” including dehydration (n=4), sleep deprivation (n=3), heatstroke (n=3), loss of appetite (n=1), and other infections (n=1).
Discussion
This report details self-reported medical issues encountered by ocean rowers during these extreme ultraendurance expeditions, providing insight into the demands on both body and mind.
Dermatologic problems ranged from minor to potentially debilitating. Abrasions, cuts, and blisters provided common routes for infection, with over 95% of reported infections occurring secondary to dermatologic complaints. Previous research also confirms infection rates to be as high as 92% in ocean rowers. 1 Confined and humid living conditions may predispose rowers to illness and infection, with gluteal pressure sores potentially at increased risk.13,14 Improved hygiene advice and skin barrier protection may help mitigate risks. Burns from boiling water in turbulent seas could be prevented by the mandatory use of gimbles for stoves.
Regular shift patterns endured by transoceanic rowers result in protracted periods of physical effort, stress, and strain that likely contribute to musculoskeletal issues. Hand symptoms were common, often described as finger dislocation, stiffness, pain, swelling, difficulty with finger extension, or a “claw-hand.” In-shore rowers also report this tightness in grip, where a carpel tunnel syndrome is often seen. 11 All rowers commonly report injury to back, knee, hip, arms, wrists, and shoulders 10 ; however, condition severity in relation to the incidence reported in river rowers remains unclear.
Mental health symptoms occurred in just under half of ocean crossings, in keeping with previous research. 1 Physiological stress, severe sleep deprivation, and extreme exercise have been linked to emotional instability, hallucinations, and psychological issues.15,16 Symptom severity and associated risk factors should therefore be a future research priority. Interestingly, a positive correlation between exertion and positive emotion has been previously reported in ocean rowers 6 and other endurance events, 2 conflicting with the frequency of mental health issues reported here. Further investigation into ocean rowing-specific stresses, such as isolation and physical demands, may indicate whether psychological coping techniques have a place in rower preparation. 6
Surprisingly, seasickness was only reported in just under half of all rowers despite small boats feeling the pitching of the sea more than larger vessels. However, an overlap with gastrointestinal or neurologic symptoms should not be excluded. Further work examining how debilitating seasickness is could aid understanding of its impact on rowers and provide support for familiarizing rowers with recommended medication regimes before departure.
Ocean rowers live on diets of 22.6 to 33.5 MJ (5400–8000 kcal) a day at sea.1,7 This increased daily consumption, together with physiological stresses, constant exercise, and freeze-dried foods, 1 might explain the gastrointestinal issues reported. However, without definitive testing, infective causes such as gastroenteritis cannot be excluded. 17 Further studies may examine the potential benefits of rowers training while eating types and quantities of food similar to ocean diets before departure.
Various neurologic issues, including numbness in the leg/foot, headaches, and dizziness/vertigo, were noted. Leg numbness due to nerve compression is commonly seen in river rowers owing to impingement of the sciatic nerve and poor seat fitting. 11 Ocean rowers have limited space for stretching exercises, so attention should be paid to ensuring seat holes are spaced sufficiently for the ischial tuberosities, preventing nerve entrapment.
Chronic headaches were also reported, backing up previous findings in this population. 1 Both headaches and dizziness/vertigo have various potential etiologies, with stress, tiredness, motion sickness, and dehydration all possible contributors. One hypothesis is that dizziness may be due to the constant rolling motion disrupting inner ear calcium carbonate crystals, but further research is required.
Physiological stress may be demonstrated by the average weight loss reported. Research has suggested that low body mass index is an injury risk factor in those undertaking heavy exercise, owing to increased physical strain through weakened muscle groups. 18 Rapid decreases in muscle mass and body habitus may therefore contribute to a lack of joint stability and abnormal kinetic loading, leading to muscular/tendon pain. However, further research is needed to confirm this association. A previous study looking at 4 transatlantic rowers also noted weight loss, together with heightened proinflammatory cytokines and C-reactive protein, whereas anti-inflammatory markers were suppressed. 4 Although below levels indicative of infection, these markers might suggest background inflammation similar to other ultraendurance events, 19 potentially contributing to reported musculoskeletal and neuropathic pain.
Limitations
These conclusions are limited by several important factors. First, only a small proportion of the total ocean rowing population were surveyed, and conclusions drawn at best indicate trends and reveal areas for future research. Likewise, the implications of variables such as age and sex are yet to be determined, with larger population samples required. Furthermore, the study population was contacted exclusively online, representing only those with access to the ocean rowing Facebook group or race websites. This limited the population and could create a bias toward more recent races and an overrepresentation of a younger demographic, who may also have a greater social media presence. 20 Additionally, participant first language was not considered, with only an English-language version available, and may have interfered with both participation and understanding. Self-reported data could lead to reporting biases wherein similar experiences are reported differently, depending on rower perceptions, or information is forgotten. Some individuals may list all issues encountered, whereas others may only note their most troubling issue. Further work is needed to understand which injuries/illnesses have the greatest impact and to contextualize physiological changes. This could involve linked pain scores, records of medical intervention, determining weight loss as a percentage change from a rower’s departure weight, and sleep data collection. Pre-existing medical conditions, medications, and a comparison control group should also be analyzed.
Conclusions
This report catalogs the experiences of 71 ocean rowers participating in one of the most grueling ultraendurance sports. The study seeks to address the limited discourse about ocean rowing, particularly with respect to understanding the medical conditions encountered. Dermatological, musculoskeletal, and mental health issues most commonly affect ocean rowers, all with the potential to become debilitating. Areas where improved advice and understanding may protect athletes were also highlighted. Future studies have potentially wide-ranging implications for our understanding of ultraendurance events and the long-term effects of intense exercise in extreme environments on mental and physical health. Further research is needed to develop evidence-based advice to reduce risks and provide better medical care and treatment to athletes.
Footnotes
Acknowledgements
Acknowledgments: The authors thank Dr. Marian Huett for her advice and guidance.
Author Contributions: Study concept and design (WJHG, JAJC, RPH); data acquisition and analysis (WJHG, JAJC); drafting of manuscript (WJHG, JAJC); approval of final manuscript (WJHG, JAJC, RPH)
Financial/Material Support: None.
Disclosures: None.