
Abstract
Introduction
The UK undergraduate medicine curriculum provides insufficient opportunities for medical students to explore the field of wilderness medicine, despite interest in the area. The student-led Cambridge University Wilderness Medicine Society devised a low-cost wilderness medicine teaching weekend that can be replicated at other institutions.
Methods
The weekend course consisted of small-group lessons introducing the roles of the expedition doctor and expedition leader and the assessment and management of acute conditions in remote environments. This was followed by a 3-station circuit to teach the principles of casualty triage, splinting, and construction of rope stretchers. These skills were then practiced in simulations in which participants rotated roles as care providers and patients. Participant confidence was compared before the course and immediately on course completion using the related-samples Wilcoxon signed-ranks test with significance accepted at P<0.05. Usefulness of course content and perceptions of learning were also assessed.
Results
Sixty-one medical students attended the wilderness teaching weekend and completed the structured feedback questionnaires. Participants rated the course highly in terms of usefulness of course content (mean±SD=18.3±1.9, range=12–20) and perceptions of learning (mean±SD=37.6±2.6, range=31–40), with 92% of participants “strongly agreeing” that the course was of high quality. There was an improvement in perceived confidence after course completion (P<0.001).
Conclusions
We have demonstrated that a teaching program consisting of structured, low-cost “teaching weekends” is a potential solution to the lack of centralized national wilderness medicine teaching and can be integrated, with minimal disruption, into the undergraduate curriculum.
Introduction
Wilderness medicine encompasses a range of traditional medical specialties with the aim of providing healthcare in remote, resource-poor settings. There is growing interest in this field among medical students in the UK. For dedicated students, opportunities include the annual student wilderness medicine conference and “Wild Trials” competition. However, wilderness medicine is predominantly treated as a postgraduate discipline and receives very little coverage in medical school curricula. Thus, the onus is on individual university societies to deliver local teaching and promotion of wilderness medicine to the wider student body.
Cambridge University Wilderness Medicine Society (CUWMS) is an example of a student-led group that was founded in response to the lack of wilderness medicine teaching in the university’s medical school and on a national level. Growing evidence highlights the benefits of student-led peer teaching in medical education1,2; as such, CUWMS organizes teaching weekends in national parks across the UK during the academic year. The aims of these courses are to raise awareness of wilderness medicine among Cambridge medical undergraduates, to teach important prehospital skills in an interactive small-group setting, and to improve student confidence in using a systematic approach when managing patients in a high-stress unfamiliar environment. 3
The CUWMS wilderness medicine teaching program was designed based on medical education research. Studies have shown that interactive small-group discussion, simulation, and deliberate practice are more effective than didactic large-group teaching. 4 -6 Furthermore, simulation-based teaching has been shown to be more effective at preparing junior doctors for assessment and management of critically ill patients when applied to related disciplines, such as trauma, 7 emergency medicine, 8 and ENT emergencies. 9
This article describes the teaching program designed by CUWMS and offers an example of a low-cost, easy-to-implement course as an adjunct to an already crowded undergraduate medical education.
Methods
Participants
CUWMS teaching weekends were advertised to current University of Cambridge medical students in the clinical years of their medical degree (years 4–6) through social media and mailing lists. Participants gave permission for the use of their questionnaire responses in this article, as well as photographs taken during the weekends. The University of Cambridge School of Clinical Medicine ethics board deemed ethical approval not required because this study evaluated a teaching project.
Course Itinerary
The course was taught by senior medical students with a specific interest in wilderness medicine and medical education, including student leaders with prehospital trauma life support accreditation and with experience in event medicine and mountain rescue. Senior faculty at our medical school who are experienced physicians with expertise in curriculum design but no specific prehospital training were consulted in the development of a formalized teaching plan and endorsed the weekend courses. We adopted small-group and simulation-based teaching methods for this course, based on participant feedback in previous iterations of the teaching weekends.
Small-group teaching
Upon arrival at the accommodation on the Friday evening (Day 1), participants were divided into 2 groups of 7 to 9 students and introduced to the roles of the expedition doctor (medic) and expedition leader.
Because the role of the “medic” is to identify and treat casualties, this teaching session focused on how to do a coherent primary survey (systematic ABCDE assessment) and provided examples of appropriate management plans for common acute presentations. During the expedition leader teaching session, students were taught how to organize extrication and maintain group safety, as well as effective communication, map skills (eg, taking a bearing, using 6-point grid references), task delegation, and awareness of environmental hazards.
Day 2 (Saturday) included a planned hike and a 3-station circuit to teach and practice core practical skills. The stations included casualty triage, splinting with the use of SAM and Kendrick splints, and making rope stretchers (Figure 1).

Rope stretcher with a tarp.
Scenario-based teaching
During the Saturday and Sunday hikes, 3 scenarios took place based on common prehospital presentations. Members of the group acted as casualties in the scenarios; they were briefed and their injuries simulated with moulage (an example is shown in Figure 2), which is widely used in wilderness medicine teaching. 10 The start of each scenario was announced to the remainder of the students without prior warning, at which point the CUWMS committee appointed 1 or 2 medics and 1 expedition leader for the scenario. For the purpose of the scenario, the remaining students were instructed to assist as non–medically trained bystanders. Participants were encouraged to behave as they would in a real-life scenario and to act out any interventions that they would perform using the equipment provided. An example scenario brief is shown in Figure 3.

Students assessing a simulated patient with head injury.
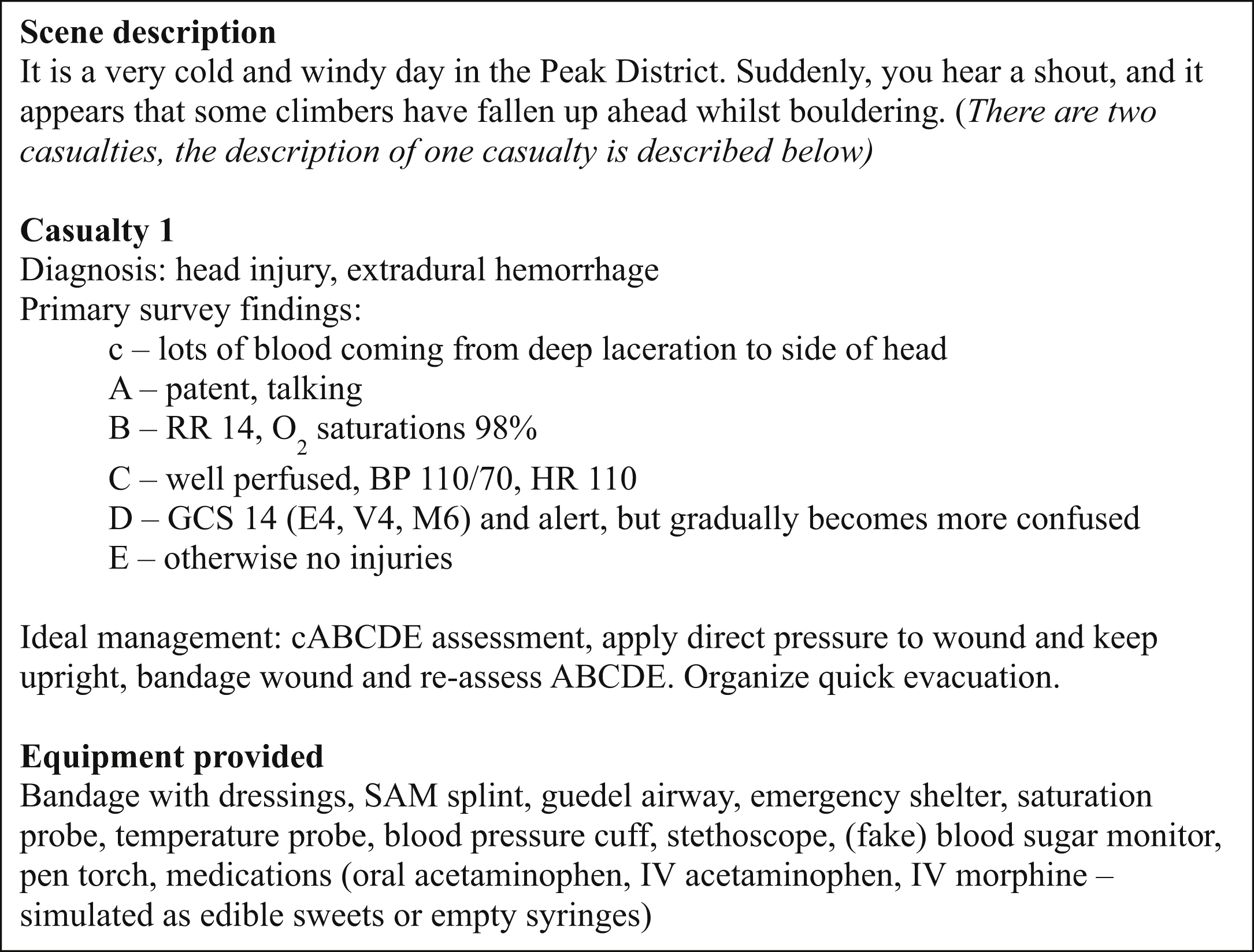
Example scenario brief.
Midway through each scenario, a new set of individuals was appointed to the roles of medic and expedition leader. The individuals from the first half conducted an ATMIST handover 11 and the scenario continued. Committee members observed how the situations were managed, provided patient observations, and gave appropriate prompts when required. Following each scenario, a group debrief allowed the actors, medics, and expedition leaders to explain their actions and to reflect on how the situation was managed. The committee then provided individualized constructive feedback before explaining the optimal management for each of the patients and answering any questions that arose. Over the course of the teaching weekend, each participant had the opportunity to lead 1 scenario as either the medic or expedition leader. The overall structure of a typical weekend course is shown as a flowchart in Figure 4.
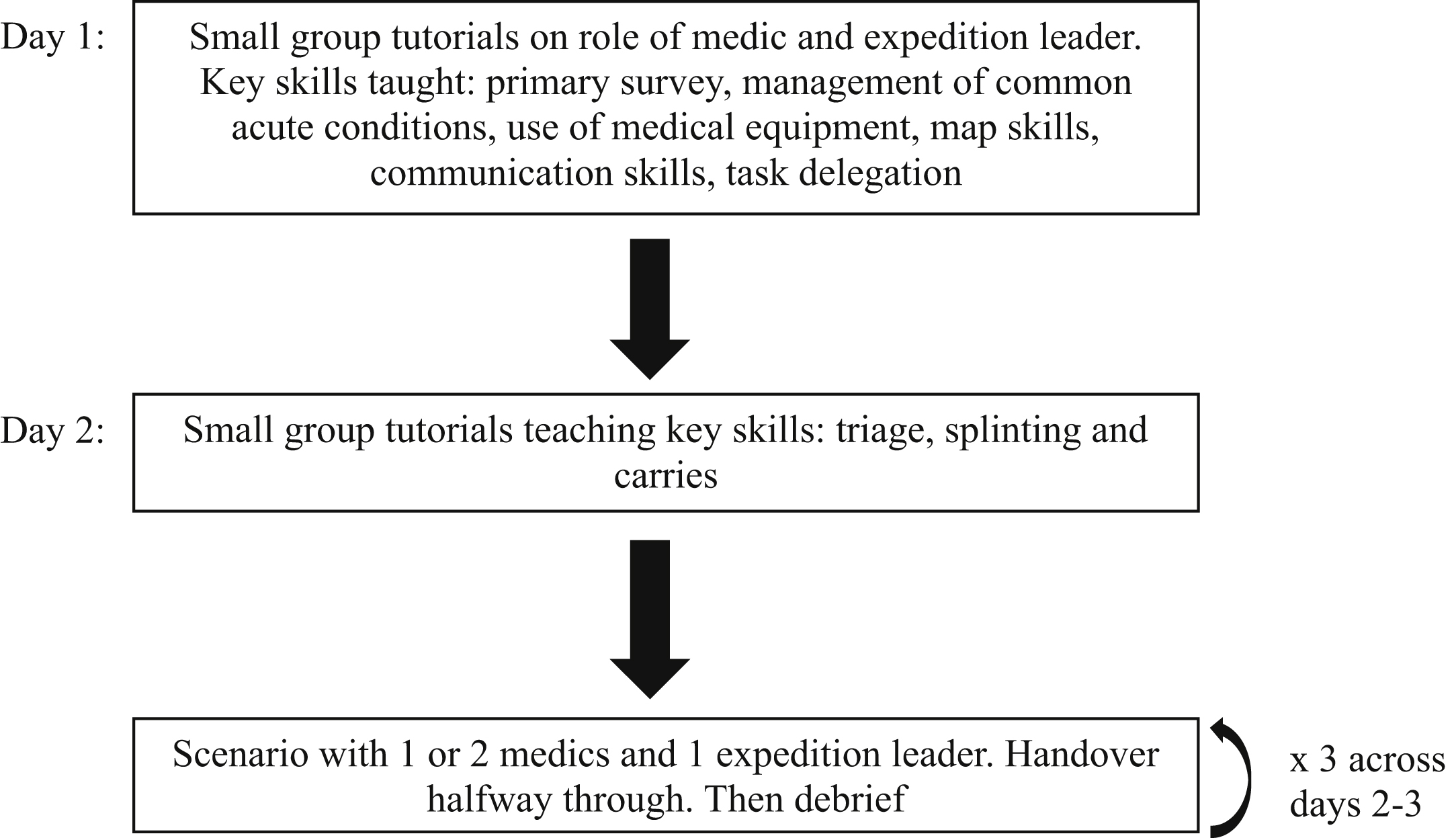
Format of wilderness teaching weekend.
Outcome Measures
Participants were given questionnaires before the start of the weekend and immediately on course completion. Perceived confidence was assessed in 8 domains (primary survey, group management and delegation, navigation and map reading, triage, splinting, making an improvised stretcher, and performance in simulated scenarios—medic role and expedition leader role). The precourse questionnaire also collected demographic information and asked participants to score the educational value of several different teaching methods. The postcourse questionnaire contained additional items to assess the usefulness of course content and perceptions of learning. Questions were formatted using a 5-point numerical Likert scale (1=strongly disagree/not confident, 5=strongly agree/very confident). A free-text question allowed participants to leave a course review and give suggestions for improvement.
Data Analysis
Analysis of participants’ confidence before and after the course was performed using the related-samples Wilcoxon signed-ranks test with significance accepted at P<0.05. Data analysis was performed using SPSS statistical software version 24 and Microsoft Excel for Mac version 16.26. Data are presented as mean±SD with range, as appropriate.
Results
Demographic Data
Five teaching weekends were held across the 2018–2019 academic year with 61 medical students from the University of Cambridge attending. All years of clinical undergraduate training were represented (year 4, 5, and 6), with over half of participants (54%) in their first year of clinical training. Before the course, 54% had exposure to wilderness medicine (Table 1).
Participant demographic characteristics (n=61)
Questions concerning preferred teaching methods were formatted using a 5-point numerical Likert scale (1=worst, 5=best).
Participant-Reported Outcomes
Participants rated the course highly in terms of usefulness of course content (18.3±1.9, 12–20) and perceptions of learning (37.6±2.6, 31–40), with 92% of participants “strongly agreeing” that the course was of high quality (Table 2).
Structured feedback questions and student responses regarding usefulness of course content and perceptions of learning (n=61) a
Questions were formatted using a 5-point numerical Likert scale (1=strongly disagree, 5=strongly agree).
There was a statistically significant improvement in confidence scores after course completion for all 8 individual domains (P<0.001) (Table 3). The largest increase in perceived confidence was seen in the “making an improvised stretcher” topic (precourse 2.2±1.2, 1–5, vs postcourse 4.2±0.7, 3–5).
Perceived confidence scores by key topics and performing roles in simulated scenarios immediately before and after the teaching weekend (n=61) a
Questions were formatted using a 5-point numerical Likert scale (1=not confident, 5=very confident).
Course Feedback
Comments from participants were positive. In particular, the scenarios were well received: “relevant and felt realistic,” “well organized,” “key learning objectives achieved,” and “linked to clinical presentations that we may encounter in hospital.” We received useful suggestions that could be implemented in the next course. A student suggested streamlining the Friday (Day 1) teaching into a shorter session and producing a written guide on the role of the medic and expedition leader as preparatory reading for the course. Another recommendation was to provide more detailed evaluation on performance during scenarios.
Discussion
Medical school provides an excellent platform for students to explore a wide range of specialties; however, there is limited coverage of certain prehospital specialties, such as wilderness and expedition medicine. Our program of wilderness medicine teaching weekends is an attempt to fill this gap in clinical training. Although 54% of participants reported previous exposure to wilderness medicine, this largely consisted of those who had attended informal CUWMS trips before the implementation of this teaching course.
The primary objectives of the CUWMS teaching program were to introduce students to wilderness medicine and to develop skills that are widely transferrable within acute medical specialties. 12 A recent systematic review has shown that new junior doctors are not confident in the assessment and treatment of acutely unwell patients. 13 This is reflected in our precourse data, where participants reported low confidence in key skills such as primary survey and triage (Table 3). Although lack of confidence does not necessarily reflect objective incompetence, it may highlight areas of the curriculum where students have insufficient teaching or clinical exposure. As such, this teaching program emphasized vital skills such as primary survey using systematic ABCDE assessment, handover, leadership, and medical management for common emergencies.
Skills taught in the role of the expedition leader are necessary to extricate patients from remote, dangerous environments to areas of safety where they can eventually access more advanced medical care. Placing students in the role of expedition leader also allowed them to develop important nontechnical skills, such as improvisation, situational awareness, and effective team leadership. These skills have previously been associated with better care in trauma and resuscitation, including higher rates of completion of primary and secondary surveys, fewer delays in initiating basic life support, and decreased time to further interventions such as endotracheal intubation and transfer to operating theatres. 8
Medical school graduates in the United States who took part in a similar wilderness medicine course during their studies reported using such transferrable skills in their clinical practice, both inside and outside of the hospital setting. 3
Teaching on these weekends is delivered via small-group tutorials and scenario-based teaching. Data from the precourse questionnaires suggested that participants prefer such teaching methods in comparison to a traditional, didactic format (Table 1). Committee members act as facilitators to promote discussion and knowledge consolidation. Scenarios allow individuals to use previously learned skills, practice decision making in high-stress situations, and develop communication skills through handovers and explanation to bystanders without the use of medical jargon. This style of learning is modeled on “deliberate practice,” a strategy shown to yield better results than passive experiential learning. 6 The scenarios vary in difficulty across the weekend, and roles are allocated based on the individual’s level of clinical training and previous experience of wilderness medicine, with feedback tailored in accordance with experience. On a group level, we assumed basic life support knowledge because this topic is covered at the start of clinical training. On an individual level, some participants had prior experience of mountain rescue and prehospital medicine, so they were assigned roles in more challenging scenarios. In general, for participants in their first year of clinical medicine, feedback focused on the structure and process of conducting a primary survey. In contrast, final year medical students benefited from detailed feedback and teaching on how to manage specific medical emergencies. This tailored approach to learning needs is an advantage of near-peer teaching: The student leaders are aware of the level of pre-existing knowledge in different year groups.
Barriers to undergraduate medical students attending established wilderness medicine courses in the UK include lack of time outside of mandatory placements and course expense. During the 2018–2019 academic year, we ran this course on 5 separate weekends. This minimized disruption to the undergraduate timetable, meaning students did not need to take study leave, miss core curriculum teaching, or sacrifice their holidays to attend a course. The average trip cost was ∼$65 USD for the entire weekend, including food, transport to and from the venue, and accommodation. We reduced costs by carpooling, batch cooking meals, staying in low-cost bunkhouse accommodation, and subsidizing trips with funding obtained from the medical school. We were therefore able to offer our program for a cheaper price than other popular wilderness medicine courses in the UK, which can cost upwards of ∼$1285 USD. This increased the accessibility of our trips because students did not need to make a significant time or money investment to attend; thus we believe these teaching weekends could be easily integrated into any undergraduate medical curriculum.
Limitations
The nature of scenario-based teaching means it can be challenging to portray medical emergencies with complete accuracy. Furthermore, by virtue of CUWMS being a student-led organization, there is limited input into scenario design from specialists in prehospital or wilderness medicine. With the benefit of such positive feedback from participants, we will be consulting experienced prehospital medicine providers to further develop the course.
Although the course was well received and there was an improvement in perceived confidence scores in all key topics, the data are subjective and therefore limited in evaluating true course efficacy. Healthcare provider confidence has not been previously shown to be correlated with knowledge or competence; however, confidence has been associated with improved patient experience. 14 In a future study design, it would be beneficial to introduce scenario-specific mark schemes, which are more conducive to objective assessment of knowledge and performance in simulations. A standardized marksheet could cover 4 key domains: primary survey (ABCDE), diagnosis, management, and nontechnical skills (communication, leadership, and delegation). Additionally, participants should be assessed at the start and end of the course with reassessment 3 to 6 months after the course to determine whether there is long-term retention of course material. External assessment could also be implemented, whereby senior clinicians who are not present at the course can evaluate video recordings of participants’ performance in simulated scenarios at the start and the end of the course and be blinded to whether the scenario was completed before or after training. Informal verbal feedback could be supplemented with written feedback, which can subsequently be used in a future study to demonstrate objective competencies after training. Long-term follow-up of newly qualified doctors would also help to further evaluate the benefits of course attendance.
We were only able to accommodate 15 to 20 students per course date. Across the 5 teaching weekends, approximately 12% of the eligible student body attended. The study population consisted of students choosing to attend the course, which we acknowledge may indicate pre-existing interest in the subject. Furthermore, because some of the attendees were friends with committee members, they may have given better feedback so as not to seem overly critical, although both positive and negative feedback were encouraged. These are all potential sources of bias in our data.
Conclusions
We have demonstrated that a teaching program for medical students can help further their interest in wilderness medicine and develop skills transferable to acute medical specialties. This program consists of structured, low-cost “teaching weekends” that could be replicated at other institutions.
Footnotes
Acknowledgements
Acknowledgments: We acknowledge all of the work put in by previous CUWMS committees, which has shaped the way we deliver teaching. In addition, we express our gratitude to the University of Cambridge School of Clinical Medicine, which provided us with a platform to promote the teaching weekends to the student body and have supported the society over several years.
Author Contributions: Study concept and design (BT, BVT, JB, GM, YP); acquisition of the data (BT, BVT, JB, GM, YP); analysis of the data (BVT); drafting of the manuscript (BT); critical revision of the manuscript (BT, BVT, JB, GM, YP); and approval of final manuscript (BT, BVT, JB, GM, YP).
Financial/Material Support: None.
Disclosures: None.