
Abstract
Bees and wasps (order Hymenoptera) are commonly encountered worldwide and often deliver defensive stings when in contact with humans. Massive envenomation resulting from >50 stings causes a toxic reaction and life-threatening complications that typically result in rhabdomyolysis and disseminated intravascular coagulation. Two male patients who were stung over 80 times by wasps experienced severe coagulation abnormality. Consecutive examination by thromboelastography (TEG) guided by heparinase treatment during their hospitalization evidenced heparin-like coagulation dysfunction despite no clinical use of heparin-like substances. Numerous tests were also conducted to confirm whether the coagulation abnormalities could be attributed to hyperendogenous heparinization and allergic reaction, rhabdomyolysis, and vascular endothelial cell injury without apparent disseminated intravascular coagulation, which might all be affected by the production of endogenous heparin. The reduced coagulation potential caused by hyperendogenous heparinization was associated with the binding of antithrombin and the activation of fibrinolysis. In addition, TEG-identified coagulopathy was moderated using protamine for heparin neutralization. The massively envenomed patients survived and were discharged after completion of medical care. We also review clinical manifestations from other published case reports, including topical treatment. Our study provides clinical evidence and guidance for diagnosis via TEG and appropriate intervention with protamine for patients with massive wasp envenomation.
Introduction
The most common injury caused by an animal is a wasp, hornet, or bee sting, with an incidence as high as 49%. 1 Stings cause local reactions and generalized symptoms, such as vomiting, diarrhea, dyspnea, redness and swelling, acute renal failure, and hypotension. 2 One reported case of massive wasp stings presented with disseminated intravascular coagulation (DIC), stroke, and acute renal failure. 3 Patients experiencing insect sting-related anaphylactic shock have also exhibited clinical and laboratory features of a severe acute generalized fibrinolytic state, but not DIC. 4 The distinctive manifestation of coagulopathy in patients stung by wasps (Vespa affinis, common species in Xiamen, Fujian, China), with severe coagulation abnormalities, has been observed (case collections from our hospital).
Two male workers (weed-whackers for cutting grass fields in Xiamen) accidentally disturbed a wasp hive and were subsequently attacked. The physical examination identified numerous stings in both. They were immediately brought to the outpatient clinic for a dermatology assessment and were given dexamethasone 10 mg intramuscularly. One day after the wasp stings, they presented to the clinical nephrology department. In this case report, we present biochemical and physical examination findings, treatment regimens, and the progress of envenomations. Both patients provided written consent allowing the case to be published.
Case Reports
Case 1
A 58-y-old man presented to the nephrology department with dark brown urine and muscle soreness. He became jaundiced around 6 h after the initial clinic visit. He was conscious with normal vital signs, including a blood pressure of 133/96 mm Hg, heart rate of 72 beats·min-1, and a respiratory rate of 18 breaths·min-1. He was admitted to the nephrology inpatient department 15 h later. On physical examination, 121 wasp sting wounds with pus were found on his back and shoulders. He had a normal abdominal palpation examination, without renal percussive pain. The results of laboratory investigations are shown in Table 1 and Figure 1. Urine analysis showed protein 1.0 g·L-1, occult blood 300 Ery·μL-1, white blood cell 35.6 p·μL-1, and glucose 28 mmol·L-1. Urine culture was negative. Routine blood examination showed a white blood cell count of 14.1×109·L-1 and neutrophil count of 12.8×109·L-1.
The biochemical measurements of 2 wasp sting victims
ALT, alanine aminotransferase; AST, aminotransferase; BN, indirect bilirubin; BUN, urea nitrogen; CKMB, creatine kinase myocardial band; Cr, creatinine; LDH, lactate dehydrogenase; TBIL, total bilirubin.
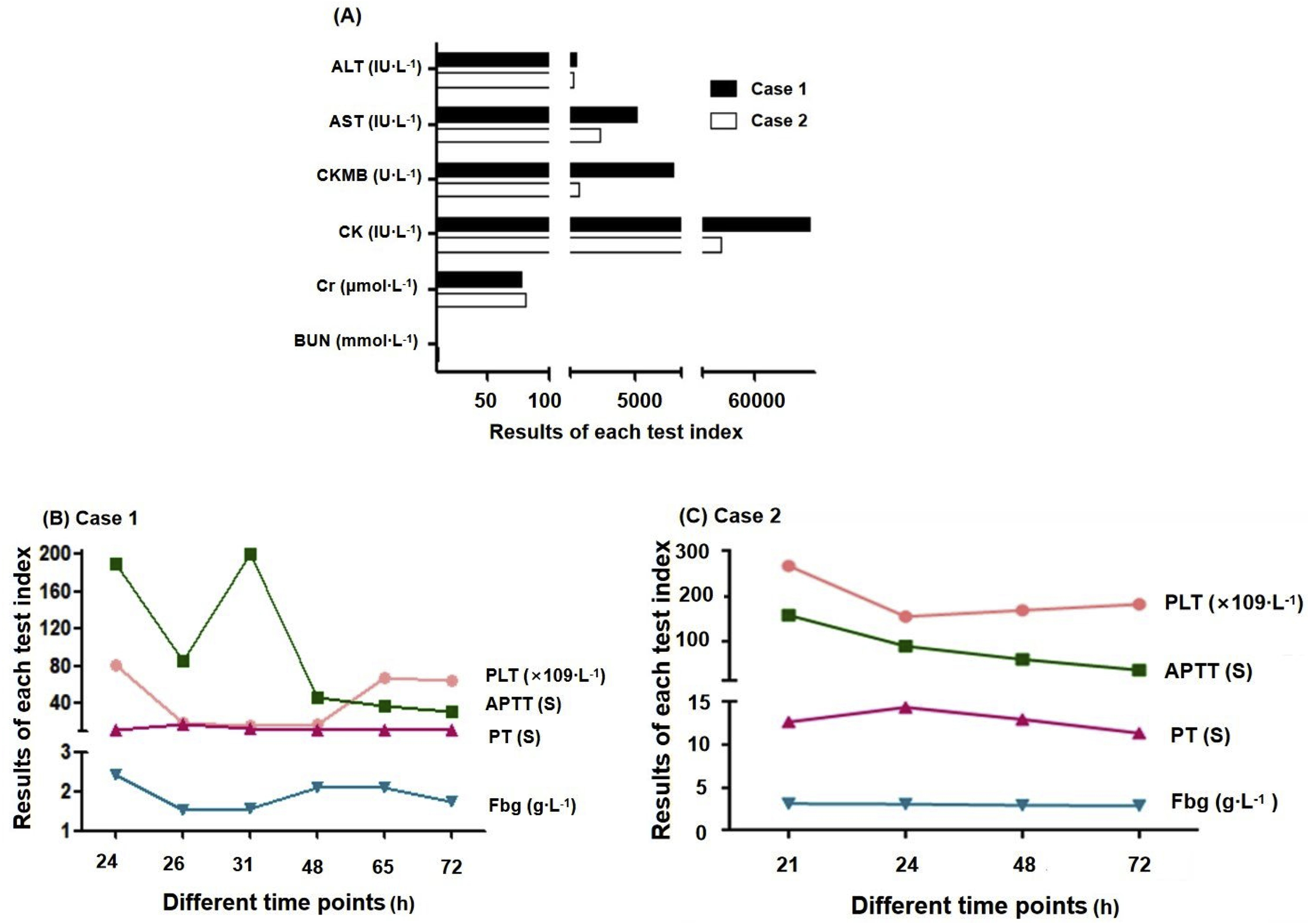
The laboratory examinations of the wasp stings patients in various time period. (A) 2 cases at hospital visit time; (B) case 1; (C) case 2. Aspartate aminotransferase (AST); alanine aminotransferase (ALT); creatine kinase (CK), creatine kinase isoenzyme (CKMB); creatinine (Cr); urea nitrogen (BUN); activated partial thromboplastin time (APTT); prothrombin time (PT); fibrinogen (Fbg); platelet (PLT).
The patient was diagnosed with greater than 120 wasp stings, rhabdomyolysis, and liver function failure. Owing to his poor clinical presentation, he was admitted as an inpatient 24 h after the initial wasp stings. Multiple organ dysfunction, including liver and kidney failure and abnormal coagulation, was confirmed, and he was transferred to the intensive care unit immediately and treated with methylprednisolone 30 mg intravenously (IV), vitamin C 3.0 g IVgtt (intravenously guttae), sodium bicarbonate 1.2 thrice daily orally (po), and fluid infusion of 1600 mL IV gtt. Emergent hemoperfusion and plasma exchange were completed within 4 h after consultation with a doctor in the hematology and infectious diseases department (sodium citrate was used as an anticoagulant during plasma exchange). He was again treated with methylprednisolone 40 mg IV gtt, ademetionine 1.0 g, reduced glutathione 1.2 g, ornithine aspartate 7.5 g, loratadine 10 mg 4 times daily po, antihistamines, and fluid infusion therapy.
Deteriorated coagulation function was observed on the second day of admission, and previous venipuncture sites exhibited bleeding. Cryoprecipitated antihemophilic factor (10 units) and platelets (2 units) were infused, following reports of critical platelet values (18×109·L-1). Compromised hemostasis was also shown by the following: A hematoma about 5 cm in size was observed at the puncture site of the left femoral artery; thrombin time (TT) results exceeded the maximal detection, D-dimer was 550 ng·mL-1 DDU, and fibrin degradation product was 6.4 ug·mL-1 (Figure 1).
Unexpectedly, without evident use of heparin-like substances in clinical practice, all thromboelastography (TEG) and routine coagulation examined values showed the evidence of heparin-like activity, with R time 15 min, K 6.8 min, Angle (α) 25.5°, MA 39.3 mm, activated partial thromboplastin time (APTT) 190 s, and prothrombin time 11.7 s at 24 h after the wasp stings. The clinician confirmed that no heparin-like drugs were used in the patient. On sample neutralization with heparinase, TEG values were improved, with R time 5.2 min, α 59.6°, and MA 43.8 mm (Figure 2A). When symptoms of overreactive heparinization occurred, provision of 40 mg protamine IV resulted in pronounced improvement in coagulation function (R time 8 min, α 47.6°, MA 41.0 mm) at 0.5 h posttreatment. At 48 h after the wasp stings, however, TEG and coagulation values were deranged again, with R time >60 min, APTT >200 s, and prothrombin time 13.8 s. After sample neutralization by heparinase, all TEG values were improved, with R time 11.9 min, α 33.4°, and MA 32.7 mm (Figure 2B). After a second injection of 40 mg protamine IV, coagulation function also showed improvement (R time 7 min, α 49.1°, MA 45.0 mm) at 0.5 h posttreatment. Platelet count progressively decreased from 81×109·L-1 at 24 h after the initial wasp stings to 17×109·L-1 at 48 h. After infusion of platelets with 2 therapeutic doses at 48 h after the wasp stings, platelet counts gradually increased and recovered to normal level on the fourth day. After the wasp stings, fibrinogen was decreased from 2.4 g·L-1 (at 24 h) to 1.5 g·L-1 (at 48 h).
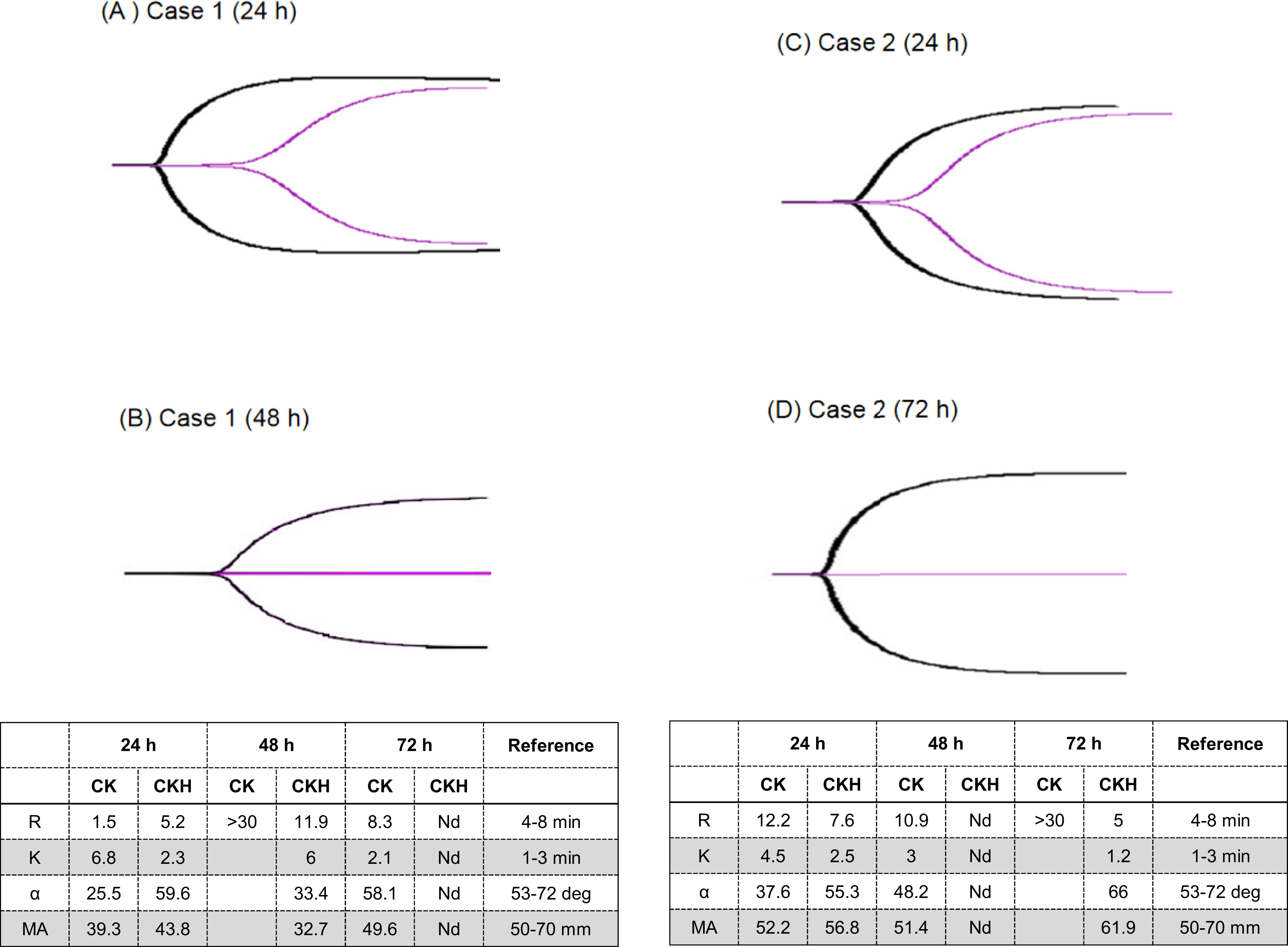
The profiles of thromboelastography (TEG) in the wasp stings patients. (A) case 1 (24 h), (B) case 1 (48 h), (C) case 2 (24 h), and (D) case 2 (72 h). Note: X-axis: the readout of each index. Y-axis: various test index. The purple curve is the result of control and the black curve is the result of heparinase coating. The curve with a short R time is the image after neutralization with heparinase. Normal range: R time: 8–10 min, α: 53–72°, K: 1–3 min, and MA: 50–70 mm. CK: standard; CKH: neutralization with heparinase. Nd: non-detection.
Other key results were as follows: increased plasmin-a2-inhibitor complex (PIC) at 2.1 μg·mL-1 (<0.8 μg·mL-1), decreased antithrombin (AT) at 41% (82–121%), tissue plasminogen activator inhibitor 1 complex (tPAI-C) at 34.7 ng·mL-1 (<10.5 ng·mL-1), and IgE at up to 295.6 KIU·L-1 at 24 h after the wasp stings (Figure 3). The percentage of B lymphocytes increased from 5% (at 24 h) to 8% (at 48 h), and the absolute count increased from 1.2 to 2.9×1011·L-1. On the fourth day, wet rales were auscultated throughout the lungs, and cefazolin 2.0 g 4 times daily IV gtt was given as a precaution against infection. At 72 h after the wasp stings, blood coagulation function recovered. In total, the endogenous heparinization lasted for 36 h. When the patient’s condition improved and became stable, he was transferred out of the intensive care unit and into the infection nursing unit. Liver, renal, and coagulation functions all gradually returned to within normal limits, and the patient was discharged on day 10.
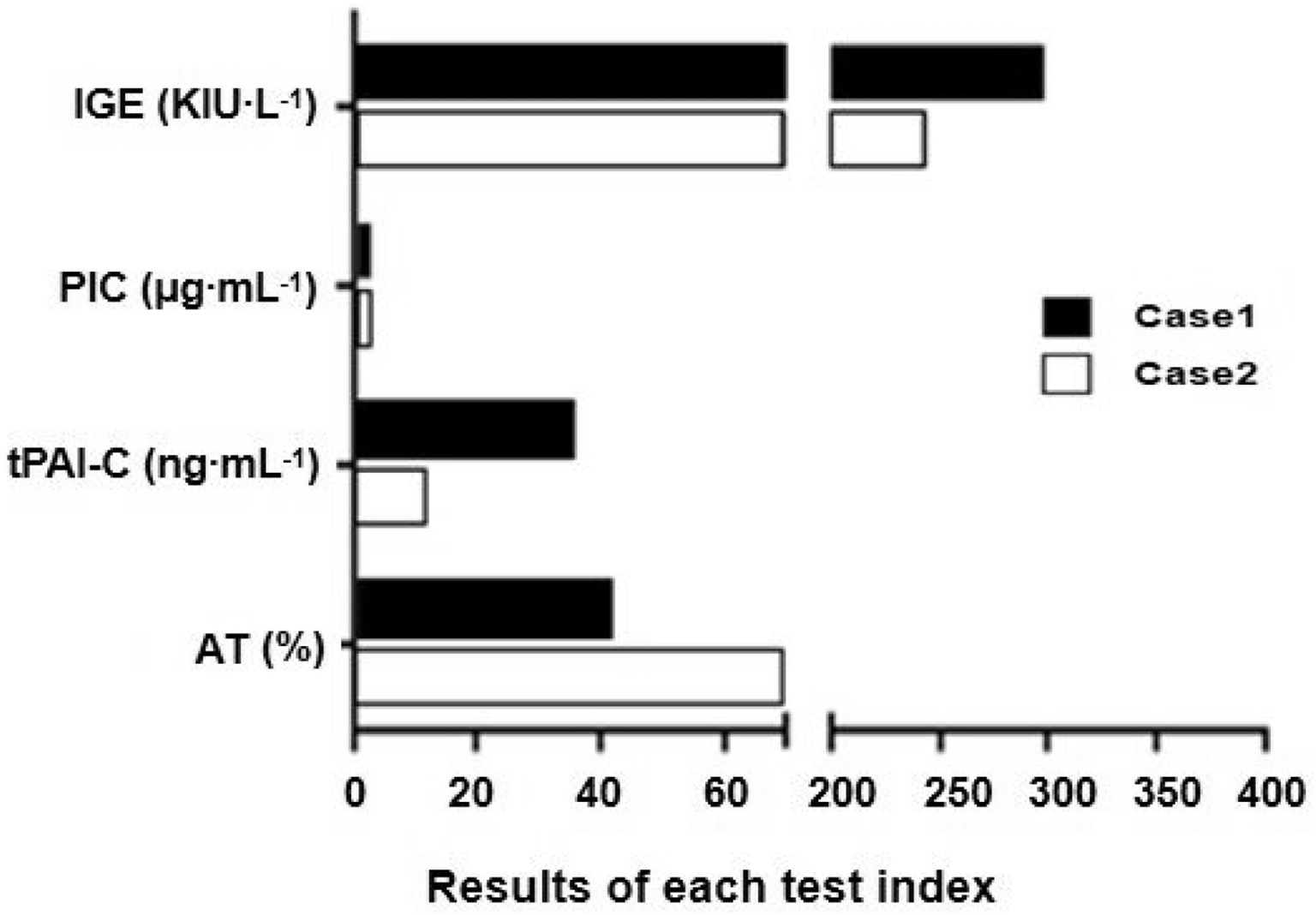
Coagulation tests of the wasp sting patients. PIC: Plasmin-a2-inhibitor complex (normal range: 0-0.85 µg·mL-1); tPAI-C: tissue plasminogen activator inhibitor 1 complex (normal range: 0-17 µg·mL-1); AT: antithrombin (normal range: 82–121%); IGE: Ig E.
CASE 2
A second 42-y-old man presented to the nephrology clinic. The patient stated his urine had turned dark brown 12 h before the clinic visit. The patient was conscious with normal vital signs, including a blood pressure of 123/85 mm Hg and respiratory rate of 18 breaths·min-1. He was admitted to the nephrology inpatient unit. On physical examination, 86 red and swollen wasp sting wounds with pus were found on his chest, back, and upper and lower limbs. His heart rate was 98 beats·min-1, and abdominal palpation was normal, without renal percussive pain. Platelets decreased from 221×109·L-1 to 156×109·L-1. Coagulation recovered gradually at 48 h after the wasp stings. Clinical manifestations of organ dysfunction, including some abnormalities in liver and kidney function (Table 1) along with abnormal coagulation, were observed, similar to Case 1.
He was treated with methylprednisolone 30 mg IV, vitamin C 3.0 g IV drip (IV gtt), sodium bicarbonate 1.0 3 times daily po, and a fluid infusion of 1600 mL IV gtt. Without using heparin-like substances in clinical practice, at 24 h after the wasp stings, all examined values were suggestive of heparin, with R time 12 min, α 37.6°, MA 52.2 mm, APTT 159.2 s, and TT results exceeding the maximal detection. After sample neutralization with heparinase, TEG values were improved, with R time 7.6 min, α 55.3°, and MA 56.8 mm (Figure 2C). This again confirmed a heparin-like effect. At 0.5 h after injection of 40 mg protamine IV, the patient’s coagulation function on TEG manifested improved (R time 8 min, α 50.4°, MA 50.0 mm). PIC was increased to 1.9 (<0.8 μg·mL-1), AT was decreased to 68% (82–121%), and tPAI-C was 10.8 (<10.5 ng·mL-1) (Figure 3). The percentage of B lymphocytes increased from 9% (at 24 h) to 11% (at 48 h after wasp sting). The absolute count increased from 5.3 to 12.0×1011·L-1, and IgE was 241.6 KIU·L-1 at 24 h after the wasp stings. After active rehydration, liver protection, antioxidation, antiallergy, inflammatory reaction reduction, and other treatments, the myozyme was significantly decreased, and the patient was discharged 3 d later.
Discussion
Insect venom-induced allergic reactions are potentially life-threatening. Clinically, insect stings can cause severe anaphylaxis and lead to cardiovascular collapse and death. The mortality rate is estimated to be 1 to 5% in different countries. 5 Ordinarily, injuries caused by mild stings can be corrected by routine antiallergy and anti-infection therapies. Recently, a transient deranged coagulation profile (transient coagulopathy) with a normal platelet count resulting from wasp venom anaphylaxis was reported. 6 Moreover, a previous report on massive bee envenomation observed the occurrence of DIC due to delayed toxic reaction. 7 In severe cases, patients may die of DIC after severe wasp stings. 8
Case 1 presented to nephrology with dark brown urine and muscle soreness. Wasp stings lead to necrosis of myocytes, and myoglobin and other contents are released into the blood circulation, subsequently causing biochemical disorders and organ function damage. Because the half-life of myoglobin (partly depending on the formation of oxidized adducts and individual elimination kinetics) in serum may be up to 6 h, 9 and low levels of myoglobin in blood circulation can be phagocytosed and cleared via mononuclear macrophage. Once muscle damage occurs, a large amount of myoglobin released in the blood exceeds the binding capability of globin. Therefore, free serum myoglobin causes myoglobinemia that results in the appearance of reddish-brown blood or dark brown urine. A rapidly implemented regimen with correct diagnosis is critical for a successful treatment strategy.
Coagulopathy featuring DIC is predominant in many published cases of mass bee sting envenomation; however, the etiology of coagulation dysfunction has rarely been comprehensively investigated. Interestingly, our cases showed dysfunctional coagulation owing to hyperendogenous heparinization, as evidenced by TEG guidance. TEG guidance more typically aids in resuscitation and blood product transfusion.10,11 In Case 1, the patient did not evolve to DIC because of timely neutralization of endogenous heparin after administration of protamine and plasma exchange. The timely identification and targeted treatment of hyperendogenous heparinization was an important and effective strategy that reversed the coagulopathy. Protamine is currently the most widely used drug for the reversal of heparin anticoagulation and is used to treat bleeding after injection of excessive heparin-like substances. In this report, 2 patients were effectively treated with protamine without other substitutes to neutralize the endogenous heparin-like substances. We found that endogenous heparinization plays an important role in coagulation dysfunction in patients with wasp sting, owing to similar symptoms caused by venom. 12 Of note, autoheparinization has been previously found in a few studies, including drowning-related asphyxia and acute traumatic coagulopathy. 13 -16 The mechanistic actions of acute traumatic coagulopathy have demonstrated protein C activation, endothelial glycocalyx disruption, depletion of fibrinogen, and platelet dysfunction, indicating that the injury of vascular endothelial cells causes the release of endogenous heparin-like substances, which is consistent with a previous report. 16 These multifactorial processes lead to hypoperfusion, decreased clot strength, autoheparinization, and hyperfibrinolysis.14,16
Heparin is an acid mucopolysaccharide that is mainly produced by mast cells and basophils and is widely found in human vascular endothelial cells, liver, intestine, and muscle tissues. Once mast cells and basophils are activated in allergic reactions, the production and release of heparin or heparin-like substances may be an important source for hyperendogenous heparinization. Hyperendogenous heparinization is not directly caused by toxic or allergic events. Mostly, it is triggered by the release of toxic substances such as bee venom peptide PLA2 in the body from allergic reactions and poisoning. PLA2 can destroy the integrity of the lipid bilayer by hydrolyzing membrane phospholipids, resulting in vascular endothelial damage. 17 In the presence of melittin, PLA2 also has a strong prohemolytic effect and is a potential factor in rhabdomyolysis in wasp sting victims. After vascular endothelial injury and rhabdomyolysis, a large amount of endogenous heparin-like substances will be released and cause deranged coagulation. Moreover, when rhabdomyolysis and liver failure occur, a large amount of heparin and heparin-like substances are released from injured muscle tissues and hepatic vascular endothelial cells. 8 The main manifestation in our cases was that, without use of heparin-like substances, the clinical R time was significantly prolonged and the α (fibrin polymerization function) was considerably decreased in TEG analysis. In addition, APTT was significantly increased 2- to 4-fold, and TT was also abnormal.
In general, heparin plays an indirect anticoagulative role, mainly enhancing the activity of AT, and the inactivation rate of serine protease by AT is dependent on heparin. We found the AT was decreased in both cases. This may be ascribed to the consumption of AT after anticoagulation with endogenous heparin. One study has demonstrated that heparin-like substances could cause excessive consumption of platelets and concurrent bleeding. 18 In the present report, we found a progressive decrease in platelets with the persistent production of endogenous heparin. Furthermore, 1 study also confirmed the antifibrinolytic effects of heparin-like substances. 19
In our report, fibrinogen was decreased in the 2 patients when hyperendogenous heparinization occurred. The measurements of PIC and tPAI-C, which represented the activation of the fibrinolytic system as well as vascular endothelial cell injury, increased. Vascular endothelial cell injury may cause the production of endogenous heparin, the activation of PIC, and a decrease in fibrinogen, indicating increased fibrinolysis. Moreover, these changes reversed when heparinization disappeared.
The patients’ symptoms varied significantly, perhaps related to the number of wasp stings. The levels of cPAIC and PIC were significantly higher in Case 1 than in Case 2, suggesting that a higher number of stings may cause more serious conditions, such as liver damage, rhabdomyolysis, and vascular endothelial injury, as well as more significant fibrinolysis. The present report also found coagulation abnormalities reported in previous observations, 20 and our observations and those of other investigators suggest that coagulopathy after mass hymenopteran stings is probably due to activated mast cells that release mediators such as heparin and tryptase. 21 -23 Although the mechanisms of heparinization and hyperfibrinogenolysis via phospholipase A2 have been described in vitro and in vivo in animal trials and a human clinical setting,24,25 some reports still maintain that the occurrences of these abnormalities excluded heparin use and bleeding that caused the prolonged clotting times and the low fibrinogen level.4,26 Recurrent coagulopathy may have occurred because of sequestration of a large amount of venom in the integument. Hyperendogenous heparinization was solely observed in the 2 patients in our report and has not been previously reported in the literature.
Conclusion
We found distinctive coagulation abnormalities in 2 cases of massive wasp stings and further demonstrated that this unique phenomenon could be the cause of hyperendogenous heparinization. Our observations have shown that TEG guidance and coagulation tests are imperative for the management of mass wasp stings. When hyperendogenous heparinization is identified, protamine is the main intervention of choice to achieve maximal recovery.
Footnotes
Acknowledgements
Acknowledgments: We thank Professor Yaw-Syan Fu (Kaohsiung Medical University, Taiwan) and Dr May-Jwan Tsai (Taipei Veterans General Hospital, Taiwan) for their critical review of this manuscript.
Author Contributions: TY, LD, and CF participated in research design, data analysis, and manuscript preparation. LD and TY carried out laboratory tests and collected experimental data. ZJ and CF designed the study and critically reviewed the manuscript. All authors reviewed and approved the final version of manuscript.
Financial/Material Support: None.
Disclosures: None.
Supplementary data
Supplementary data to this article can be found online at
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.