
A 55-y-old male presented to the emergency department with a laceration on the medial aspect of the left thigh (Figure 1).

Muscle deep laceration exposing the injured belly of adductor longus and adductor brevis.
What animal caused this injury? How should it be treated?
Diagnosis
Mauling by Himalayan Black Bear
Discussion
The patient heard a sudden barking of dogs while he was grazing goats and sheep. The goats and sheep started bleating and running haphazardly in all directions. Suspecting that a predator was nearby, the patient grabbed his shepherd’s crook and went toward the goats and sheep. There, he found a large black bear that he described as bigger and stronger than he was. Fearing that the bear would attack and injure his goats, the patient tried to scare the bear with his crook. The bear retaliated by attacking him. When the patient tried to escape, the bear pounded on his back with its claws. The patient stumbled, providing an opportunity for the bear to grab him by the hips and bite him on the left thigh. The patient was rescued by his friends, who scared the bear away.
On examination, the patient was alert and oriented with normal vital signs. The laceration measured 10×10 cm, exposing the injured bellies of the adductor longus and adductor brevis muscles. The contents of Hunter’s canal was intact. The patient reported pain of the back and left thigh. There were 3 puncture wounds on his back, with associated contusions. There were also lacerations with contusions on the left lumbar region and right hand. A chest x-ray showed fractures of the left fourth, fifth, and sixth ribs (Figure 2). Arterial and venous Doppler studies of the left leg were normal.
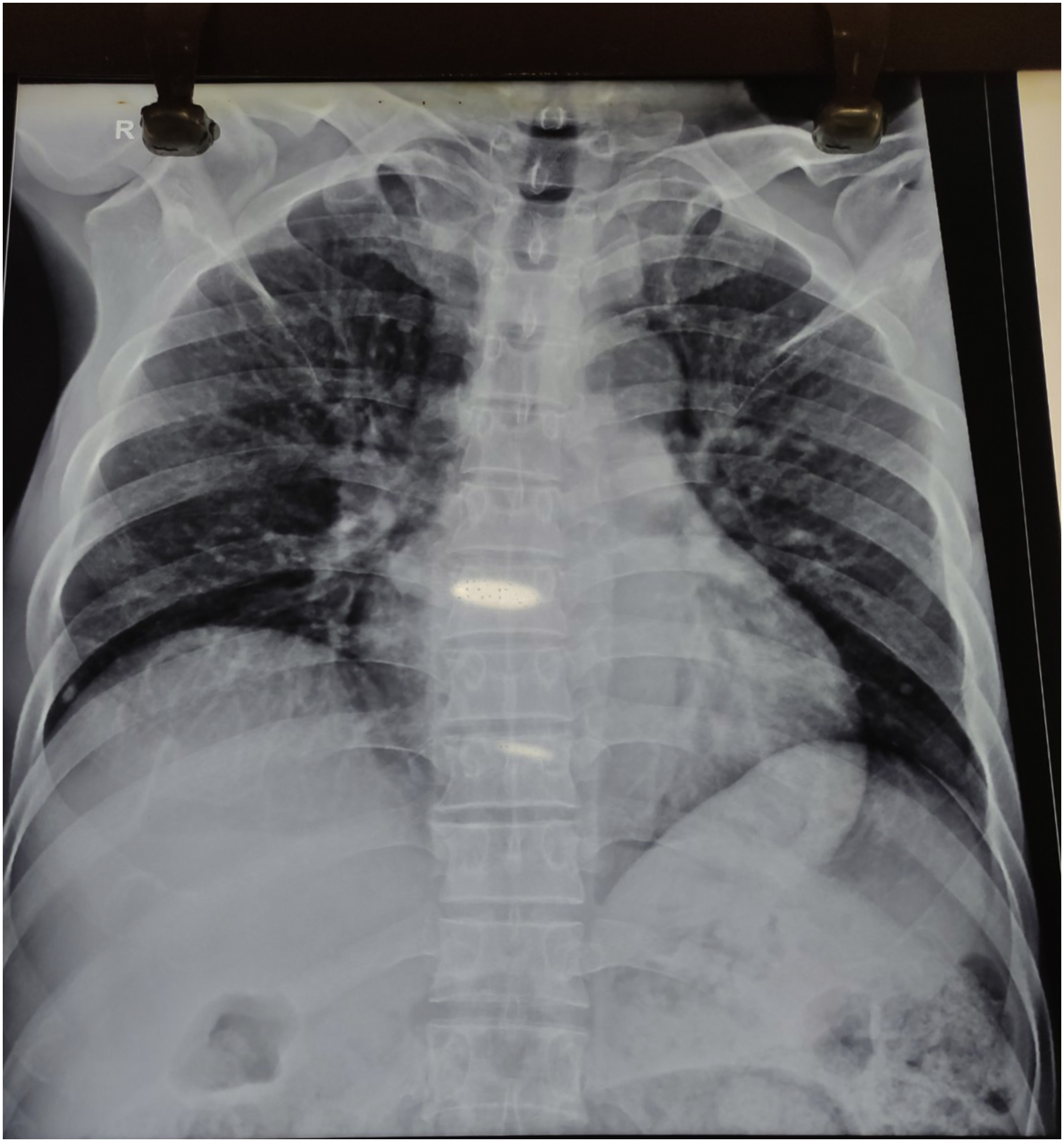
Chest x-ray showing fractures of the left fourth, fifth, and sixth ribs.
The laceration on the thigh was irrigated and debrided to remove necrotic tissue with the patient under spinal anesthesia. The muscle belly was repaired and the wound was closed (Figure 3). The patient received a dose of tetanus toxoid and a course of broad-spectrum antibiotics. After 2 wk, there was a necrotic wound margin. Sutures were removed and wound margins were debrided. Exploration revealed healthy underlying subcutaneous tissue and the previously sutured muscle. There was no sign of infection. The wound was then reclosed with a tension-free closure. The wound was well healed at 1 mo (Figure 4).

The laceration after repair.

The wound after 1 mo.
Written informed consent was obtained for the use of images and medical history for educational purposes, including publication.
Discussion
Three bear species are found in Nepal: the sloth bear (Melursus ursinus), the Himalayan black bear (Ursus thibetanus), and the Himalayan brown bear (Ursus arctos). The Himalayan black bear has a mostly black coat with a white or cream-colored chevron on the upper chest. Adult bears are 70 to 100 cm at the shoulder and 120 to 190 cm long. Males weigh an average of 135 kg. 1 -3 Himalayan black bears, also known as Asiatic black bears, are found in the middle hills of Nepal from 1500 to 3500 m. 3 The incident occurred in the Palpa district, in the middle hills southwest of Pokhara. Although, bear maulings are common, mortality from bear attacks is rare compared to attacks from other predators. 4 Bears attack humans when they feel threatened or to protect their cubs. Sometimes they may seem to attack suddenly without provocation. Bears often attack the victim’s face, necessitating emergency airway management and facial reconstruction.1,2,4,5 In the absence of facial injuries, bear mauling can be identified by the specific pattern of injuries produced by teeth or claws. 3 Sharp claws and teeth with strong jaws can cause deep wounds. Bear bites can penetrate up to 1.5 cm; claws can penetrate up to 4 cm. Although wounds may appear superficial, careful examination is mandatory to rule out underlying injuries. Prophylactic antibiotics are indicated. Amoxicillin-clavulanate is the first-line agent. Tetanus toxoid should be administered if previous vaccination status is unknown or incomplete. 5 Wounds at high risk for infection, including those with extensive soft tissue injuries or involving bones, joints, or vital structures, should not be closed primarily. Close follow-up is mandatory for all wounds because the extent of damage may not be obvious, even with careful examination.
Footnotes
Acknowledgements
Acknowledgments: We thank the section editor, Ken Zafren, MD, for his efforts in editing our manuscript.