
Abstract
Finger flexor pulley system injuries are the most common overuse injury in rock climbers. These injuries occur rarely outside of rock climbing, owing to the sport’s unique biomechanical demands on the finger. As rock climbing continues to grow and earn recognition as a mainstream sport, an understanding of how to diagnose and treat these injuries also has become important. Our purpose is to describe current concepts in anatomy, biomechanics, clinical evaluation, imaging, prevention, and treatment strategies relating to finger flexor pulley system injuries. Our literature search was performed on PubMed with MeSH terms and keywords as subject headings to meet the objectives of this review. The “crimp grip” used in rock climbing is the mechanism for these injuries. The A2, A3, and A4 pulleys are at the highest risk of injury, especially when loaded eccentrically. Physical examination may reveal clinical “bowstringing,” defined as the volar displacement of the flexor tendons from the phalanges; however, imaging is required for characterization of the underlying injury. Ultrasound is highly sensitive and specific for diagnosis and is recommended as the initial imaging technique of choice. Magnetic resonance imaging is recommended as an additional imaging study if ultrasound is inconclusive. Properly warming up increases the amount of physiologic bowstringing and is thought to prevent injury from occurring. Pulley injuries may be classified as grade I through IV. Conservative treatment, including immobilization, the H-tape method, and the use of a protective pulley splint, is recommended for grade I to III injuries. Surgical repair is reserved for grade IV injuries that are not amenable to conservative treatment.
Introduction
The popularity of rock climbing has increased remarkably, both recreationally and competitively, over the past 30 y. Indoor climbing, primarily, has seen exponential growth globally, and especially within the United States. The proposed debut of competition climbing in the now postponed 2020 Tokyo Summer Olympics speaks to its ever-growing recognition as a sport. 1 “Free Solo,” a rock-climbing film, won best documentary at the 2019 Oscars ceremony, further emphasizing its broad appeal. According to the 2019 annual report by the International Federation of Sport Climbing, 44,500,000 people worldwide climb regularly, with 9,000,000 of those in the United States.2,3
As a consequence of the sport’s growth, climbing-related injuries have increased concomitantly. An average of 2237 climbing injury-related emergency department visits in the United States occurred annually between 1990 and 2007. 4 Lower extremity injuries were most common, and overuse injuries were most frequent in the upper extremities. 4 More recently, 2 large retrospective national database studies estimated an average of 3419 rock climbing injuries were seen in emergency departments annually between 2008 and 2014, representing a 50% increase between 1990 through 2007 and 2008 through 2014.5,6 The injury patterns remained consistent, with the lower extremities being most vulnerable, likely owing to falls that cause most injuries.4,5
Fingers sustain the most overuse injuries in rock climbers. 7 -9 Specifically, isolated closed injury of the finger flexor pulley system (FFPS) is a diagnosis rarely seen outside of rock climbers. FFPS injuries were first described in 1990, and the climbing community has been uniquely susceptible owing to the patterns of training and biomechanical demands on the hands in this sport.10,11 Subsequently, numerous case reports document FFPS injuries as the most common overuse injuries of the upper extremities in rock climbers. 8 -10,12-17 The most recent statistics of injury patterns show that finger injuries are the most common injury, accounting for 41% of all injuries. 7 Pulley injuries of the fingers were the most frequent diagnoses, representing 30% of the finger injuries and 12% of all injuries. 7 The shoulder was the second most common site of injury, accounting for 20% of all injuries. 7 As a further sports rarity, an isolated small case series documented FFPS injuries in baseball pitchers. 18
Our goal is to summarize the available literature and describe current concepts in anatomy, biomechanics, clinical evaluation, imaging, prevention, and treatment strategies relating to FFPS injuries.
Anatomy
The finger flexor tendon system of the hand consists of a series of fibro-osseous sheaths through which the tendons of the flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS) course. 19 The sheath is composed of 2 distinct tissue components, synovial and retinacular (pulley), that serve distinct functions. The synovial component acts as “packing” that allows for movement of adjacent nondeformable tissues, while also lubricating surrounding cartilage. The retinacular or pulley component consists of localized thickenings of the sheath and serves to maintain the flexor tendons adjacent to the phalanges that promote biomechanical efficiency in finger flexion. The sheath, as a whole, prevents anteroposterior and lateral movement of the tendons from the axis of the finger.20,21 The second through fifth digits contain 5 annular pulleys (A1–A5) and 3 cruciate pulleys (C1–C3) interposed segmentally throughout the digit, beginning in the distal palm and ending at the distal interphalangeal joints (Figure 1). 22 Annular pulleys are ring-shaped in configuration, whereas the cruciate pulleys have an eponymous cruciform shape.
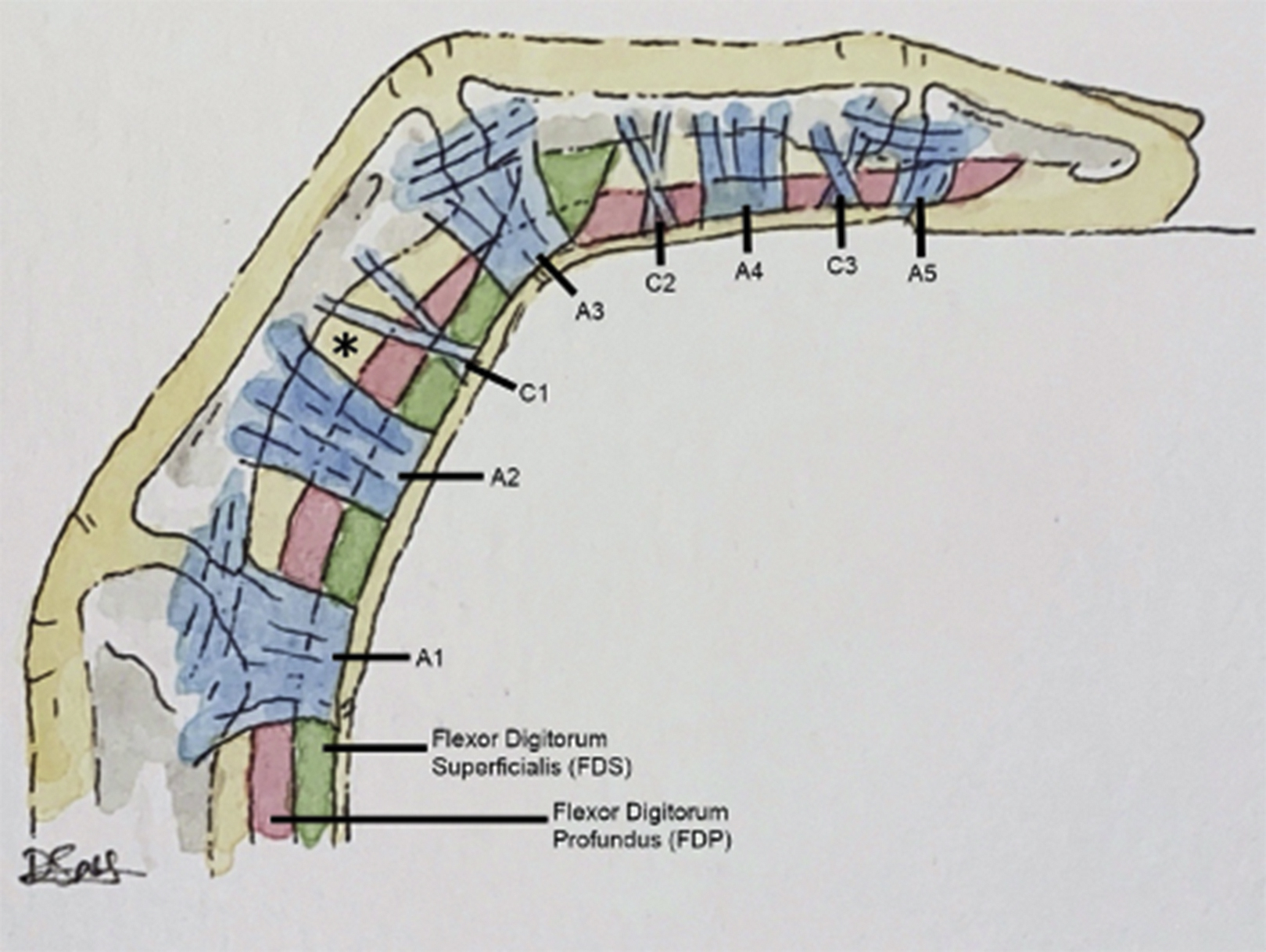
Normal anatomy of the finger flexor pulley system. Flexor tendons (flexor digitorum profundus and flexor digitorum superficialis) and associated annular (A1-A5) and cruciate (C1-C3) pulleys. Intact tendon-to-bone distance (∗).
Annular pulleys can be further subdivided into true fibro-osseous pulleys that insert directly into bone and those that insert onto the volar plate. The volar plate, found on the palmar aspect of the metacarpophalangeal and interphalangeal joints, is a ligamentous structure that functions primarily to prevent hyperextension of the digits. The A2 and A4 pulleys are broader, stronger, and insert directly into bone. Traditionally, they have been considered most important to prevent volar displacement of the flexor tendons away from the phalanges, a phenomenon termed “bowstringing.”22,23 Importantly, an intact FFPS may exhibit a small amount of bowstringing, termed “physiologic bowstringing.” The A2 and A4 pulleys insert directly into the proximal and middle phalanges, respectively. The others (A1, A3, and A5) are less rigid and are not considered true fibro-osseous pulleys. 24 The A1, A3, and A5 pulleys are located over the metacarpophalangeal, proximal interphalangeal (PIP), and distal interphalangeal (DIP) joints, respectively.
The first cruciate pulley is located between the A2 and A3 pulleys and attaches to the proximal phalanx. The second cruciate pulley is found between A3 and A4, distal to the PIP joint. The third cruciate pulley is found between A4 and A5, proximal to the DIP joint. 25 No pulleys are present directly over the distal phalanx.
The lumbrical muscles are intrinsic muscles of the hand that originate from the FDP and insert into the lateral aspect of the extensor tendon mechanism of the fingers. 26 They function to extend the PIP and DIP joints and flex the metacarpophalangeal joints. 26 Although a relatively small muscle, the proximity of the lumbricals to the FFPS renders them important in the grading of FFPS injuries.
Biomechanics
The high frequency of overuse injuries of the fingers in rock climbing can be explained by the sport’s unique biomechanical demands. The upper extremities often support much of the climber’s weight through a few fingers at a time. Specifically, the “crimp grip” is used in rock climbing to maximize contact of the fingertips on rock climbing holds with little surface area. Accordingly, the crimp grip is the mechanism for FFPS injuries.27,28 The crimp grip is characterized by the PIP joints being flexed at about 90 degrees, while the DIP joints are maximally hyperextended (Figure 2).

The crimp grip position.
Anatomically, the crimp grip position puts high levels of stress on the FDP and the FDS as they contract to maintain the conformation of the digits against the weight of the body.29,30 The stress on the FDP and FDS, paired with flexion of the PIP, is counterbalanced by the flexor tendon pulleys as they bend in resistance. The highest tension is on the A2 pulley, with forces 3 to 4 times greater than at the distal phalanges. 24 As a result, the crimp grip position is associated with a higher incidence and distance of physiologic bowstringing compared with other common grip positions (“slope grip,” “pinch grip”) used by rock climbers.27,31
The A2 and A4 pulleys are the least deformable and have a higher breaking strength than the A1, A3, and A5 pulleys.32,33 The A2 pulley typically is estimated to withstand forces of approximately 431 N, equivalent to nearly 45 kg (100 lbs) of force. 34 Recreational rock climbers can load the A2 pulley with forces between 380 N and 700 N, which equates to an average of 54 kg (120 lbs) of force.27,35 These magnitudes of force are well in excess of the normal limit of the annular pulleys; therefore, with the repetitive supraphysiologic loading of the pulleys, overuse injuries occur with disruption of the pulleys.
Injuries
The list of differential diagnoses for an injured finger in a rock climber is broad, including injuries of the tendons, tendon sheath, bones, and FFPS. 36 We will focus on injuries of the FFPS. Injury of the FFPS in rock climbers was first described in a case report in 1990.10,11 Since then, injuries of the annular pulleys in rock climbers have been documented extensively.9,12,14-16,19 The fourth digit (ring finger) is the most commonly affected, followed by the third digit (middle finger). 37 -39 Isolated A2 pulley ruptures are the most frequently reported of all significant finger injuries.40,41
The pattern of FFPS injury is thought to be progressive and predictable, due to the known biomechanical limits of the annular pulleys. Most often, the distal part of the A2 pulley becomes disrupted, and injury can progress from partial to complete rupture, even before the A3, A4, and A1 pulleys become involved. 42
Biomechanical analyses have suggested that injury to the pulleys is most likely to occur when they are loaded eccentrically.31,43,44 Given that the pulleys are not muscular tissue, eccentric loading in this context denotes the direction of movement of the finger (eg, extension that occurs in a sudden opening of the hand). This suggests different pulley capacities under eccentric versus concentric loads.31,43,44 The fourth digit A2 pulley strength is the weakest, whereas the A4 pulley strength is consistently stronger in the second digit (index finger). 33 Although rare, isolated cruciate pulley injuries also have been described in the literature. 45
The grading system for FFPS has 4 levels of injury. 16 Grade I injuries include isolated pulley strains (Figure 3). Grade II injuries are those in which a complete rupture of A4, or partial rupture of A2 or A3, is present (Figure 4). Grade III is a complete rupture of A2 or A3 (Figure 5). Lastly, grade IV injuries are those that involve multiple pulley ruptures, or a single A2 or A3 rupture with involvement of a lumbrical muscle or surrounding collateral ligaments.
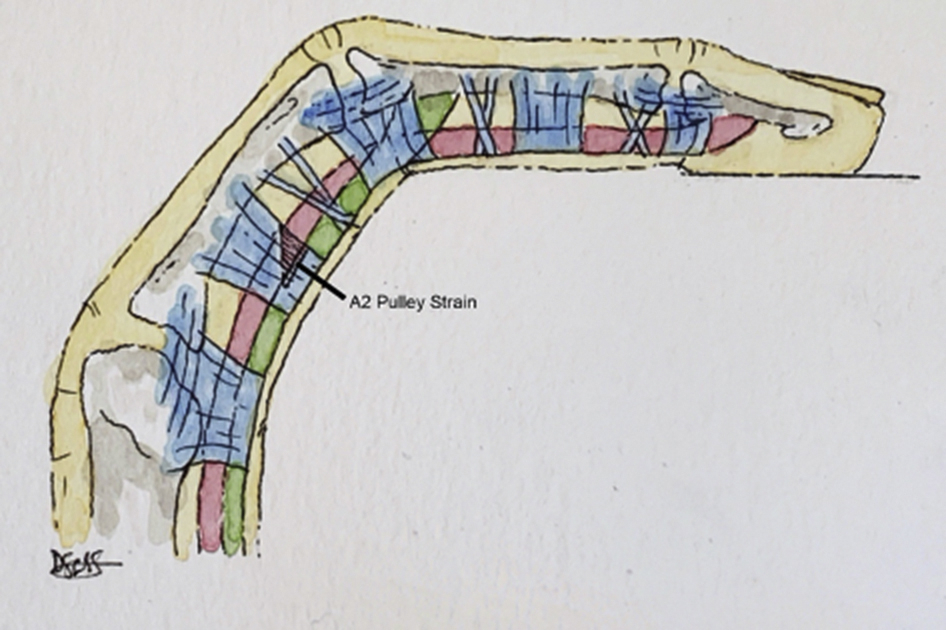
Grade I injury manifested as an isolated strain of the distal aspect of the A2 pulley (triangle).
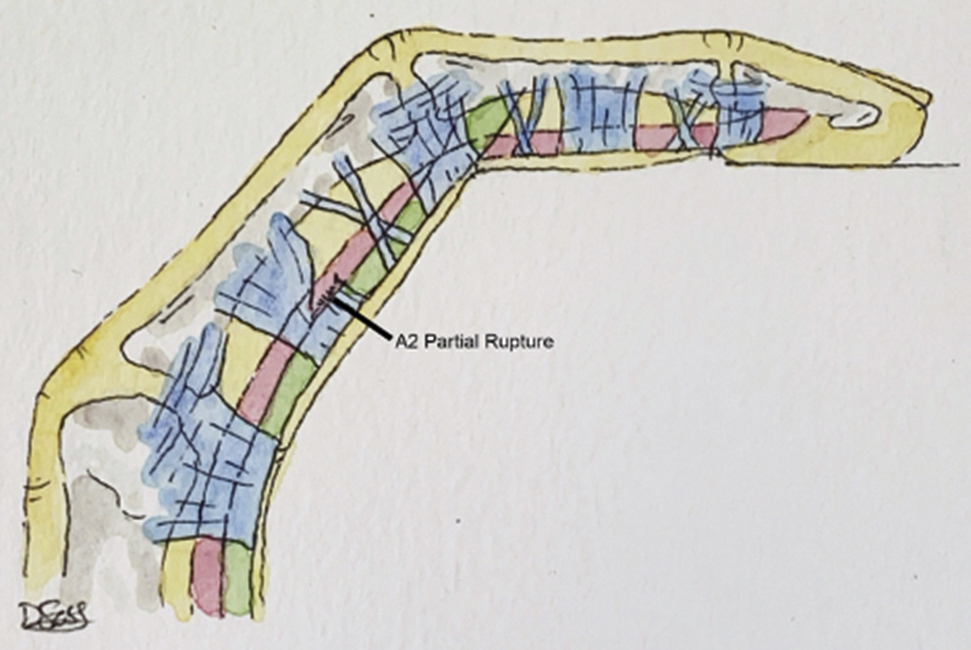
Grade II injury manifested as a partial rupture of the distal aspect of the A2 pulley.
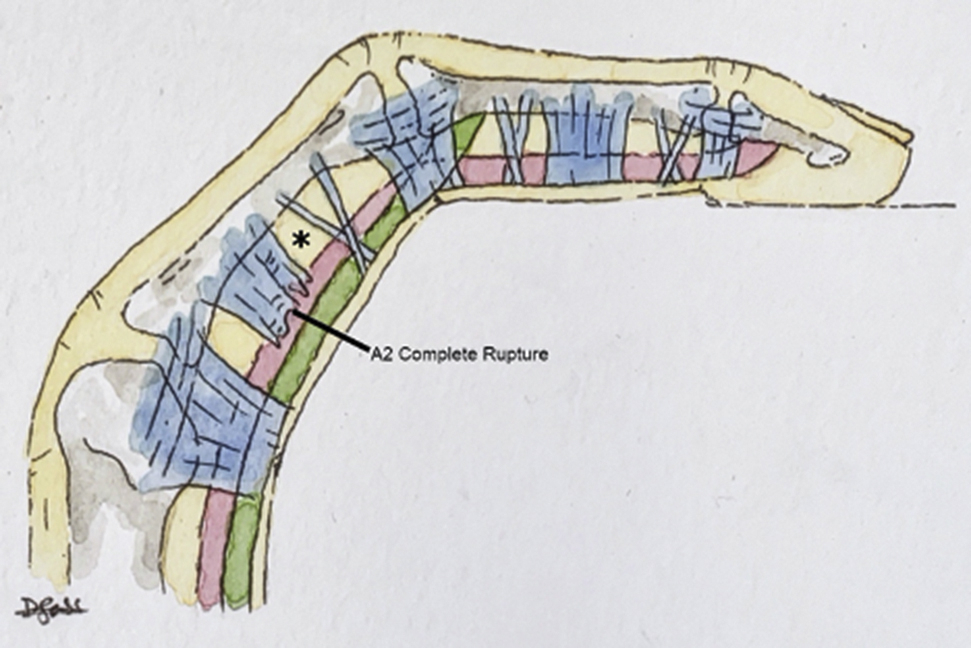
Grade III injury manifested as a complete rupture of the A2 pulley. As a result of the injury, bowstringing is seen, illustrated by the volar displacement of the flexor tendons from the phalanges, resulting in an increased tendon-to-bone distance (∗) (compare to Figure 1).
In summary, the A2, A3, and A4 pulleys have the highest risk of injury, and the A2 pulley is the most frequently injured. The fourth digit (ring finger) is most commonly affected. The risk of injury is highest in the crimp grip position, particularly with eccentric loading, owing to the increased biomechanical demands on the FFPS in this position.
Evaluation of Injury
Climbers who have sustained an FFPS injury report hearing a “pop” while grasping a climbing hold. More commonly, there is a sudden onset of pain and swelling over the affected pulley or pulleys, with possible numbness and local hematoma formation. Many climbers disregard the discomfort and continue climbing for weeks, with chronic pain over the volar aspect of the affected digits. 9
In a 2006 systematic review, the most commonly recommended diagnostic criterion in all 29 papers was clinical “bowstringing” over the volar aspect of the PIP joint on physical examination. 46 Although diagnostic, bowstringing on physical examination does not characterize the extent of underlying injury. If it is the only finding, this does not allow prognostic determination. Furthermore, it is not an infallible diagnostic sign; some less severe injuries of the FFPS may not demonstrate clinically detectable bowstringing, thus yielding a false negative finding. 47 There is no documented relationship between the severity of FFPS injury and presence of clinical bowstringing on physical examination.
A report described an isolated complete A2 pulley rupture that was diagnosed simply by placing a silicone wedding ring over the region of the suspected injury. This resulted in a degree of restored range of motion, provided temporary relief by bolstering the ruptured pulley, prevented anterior movement of the flexor tendons, and confirmed disruption of the A2 pulley without the need for imaging evaluation. 48 However, this method does not reveal the extent of injury and may, if used alone as a method of diagnosis, lead to underdiagnosis of injuries that would have warranted surgical intervention. Furthermore, it is likely that the silicone ring, similar to conventional taping, may compromise the neurovascular bundle of the finger, rendering it a questionable, and perhaps harmful, diagnostic method. 49
Clinical bowstringing, swelling, and tenderness over the anatomic pulleys are helpful signs on physical examination, but no detailed studies have confirmed their diagnostic accuracy, sensitivity, or specificity. Physical examination may be limited because of the presence of pain and soft tissue swelling, and often there is restricted range of motion of the digits. Furthermore, the degree of bowstringing does not predict the extent of injury accurately. Thus, given all these limitations, imaging evaluation should be obtained with these suspected injuries to characterize the injuries accurately.
Imaging
Imaging evaluation is indicated when a suspected injury of the FFPS is present to assess the integrity of the internal structures. Ultrasound (US) and magnetic resonance imaging (MRI) provide adequate visualization of the FFPS and are useful to confirm the diagnosis and degree of pulley injury. The distance between the flexor tendons and the phalanges, termed tendon-to-bone distance, traditionally has been used in both US and MRI as an indirect marker of FFPS integrity or disruption. The tendon-to-bone distance is an objective measurement used to quantify bowstringing, which, using proposed diagnostic thresholds, allows the physician to distinguish between physiologic and pathologic bowstringing that results from a pulley rupture.
Ultrasound
US has been used to evaluate FFPS injuries since 1999, and it is the most widely used imaging technique to detect these injuries. 50 US is inexpensive, noninvasive, and more readily available than computed tomography and MRI. US permits dynamic evaluation of the digits in different degrees of flexion and provides live, direct visualization of the A1, A2, A3, and A4 pulleys and all cruciate pulleys. 51 The disadvantages of US include its accuracy being operator-dependent, and the space the US transducer occupies during the examination that sometimes limits PIP flexion to about 60 degrees.42,46
The normal flexor tendons are visible on US as hyperechoic fibrillar structures. 20 The appearance of the pulleys on US is variable, owing to anisotropy. 20 Anisotropy is an artifact that is seen in musculoskeletal US due to the ability of tissues to conduct or reflect soundwaves differentially based on the angle of incidence of the soundwaves. When the angle of the US beam is perpendicular to tissue being observed, the resultant image appears hyperechoic. Therefore, the volar surfaces of the pulleys generally are visible as thin hyperechoic bands surrounding the flexor tendons.16,20,42 As the insonating US beam degree moves away from the perpendicular position, the resulting image becomes hypoechoic. This is why the lateral aspects of the pulleys often are hypoechoic. 20 A US example of a finger with an intact A2 pulley is shown in Figure 6.
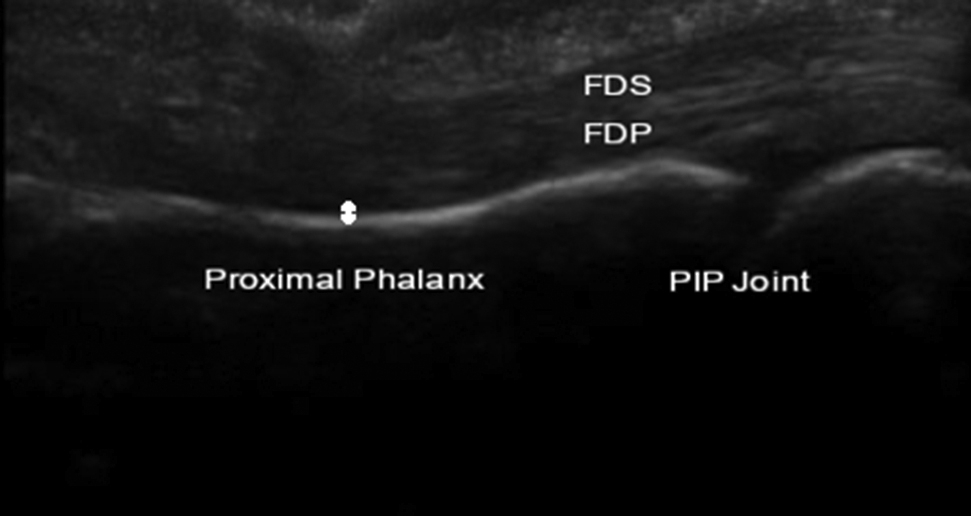
Intact A2 pulley. Ultrasound image in the longitudinal plane of a patient with an intact A2 pulley. Note that the flexor tendons are close to the proximal phalanx (double-sided arrow).
Pulley injury is manifested on US directly as pulley discontinuity and indirectly as bowstringing of the flexor tendons (Figure 7). 52 Regarding specific tendon-to-bone distances used for thresholds to indicate injury, the literature is inconclusive. Tendon-to-bone distances ranging from 1 to 3.3 mm have been recommended as sensitive thresholds to diagnose A2 and A4 pulley ruptures.42,53-55 Despite the wide range of thresholds suggested in the literature, we prefer using a tendon-to-bone distance of >2 mm as an adequate, highly sensitive and specific threshold to diagnose A2 and A4 pulley ruptures. Diagnosis of A3 pulley ruptures via measurement of the distance between the volar plate and the flexor tendons has been suggested, with a distance >0.9 mm providing 76% sensitivity and 94% specificity. 56 The sensitivity and specificity of US to diagnose A2 and A4 pulley ruptures have been reported to be 90 to 98% and 98 to 100%, respectively.16,56 Thus, US is highly sensitive and specific in diagnosing injuries of the FFPS and is the initial imaging technique of choice to evaluate these suspected injuries.
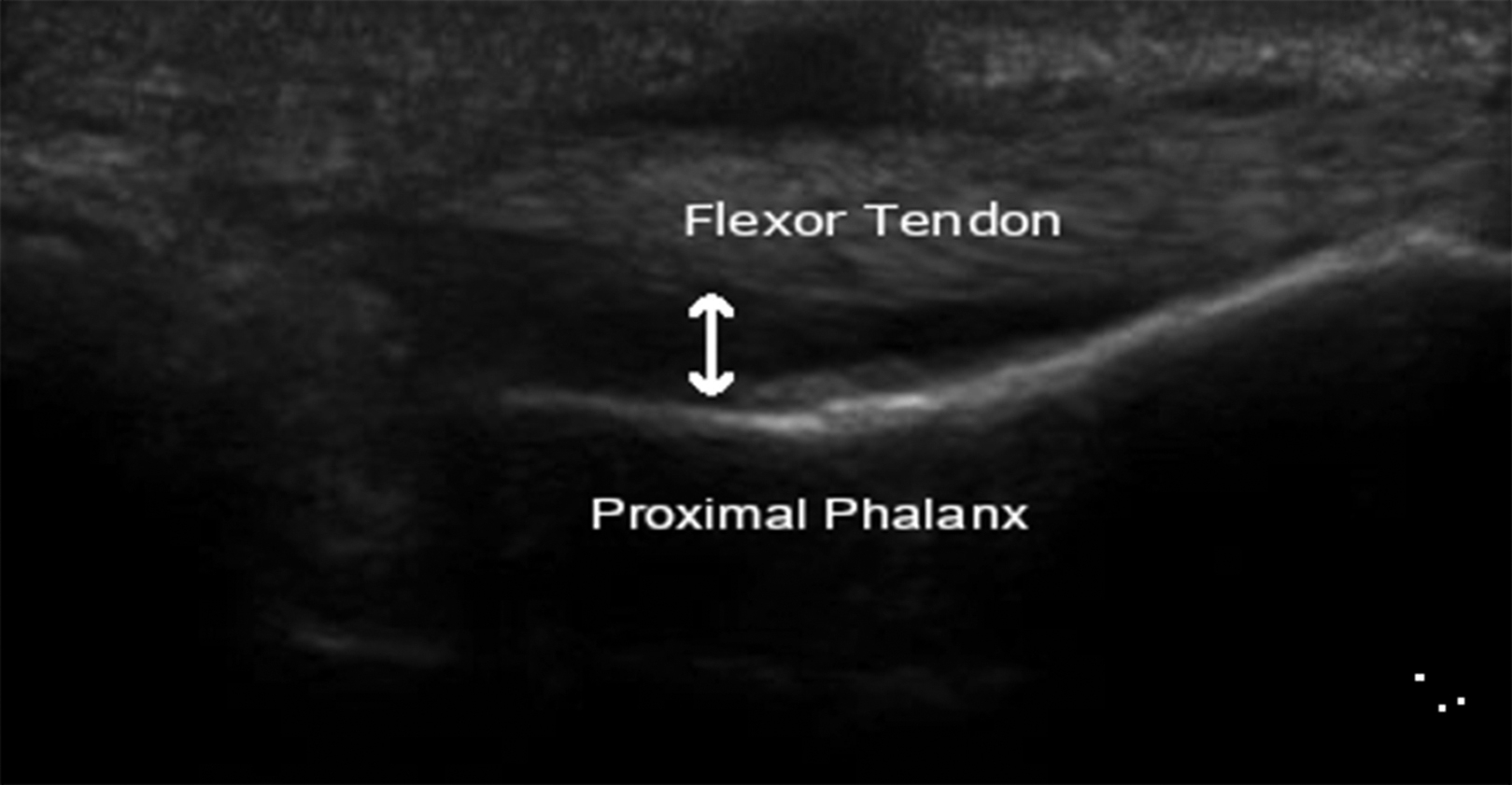
Ruptured A2 pulley. Ultrasound image in the longitudinal plane of a patient with a ruptured A2 pulley. Note the increased tendon-to-bone distance compared to Figure 6 (double-sided arrow).
Plain Film X-Rays
Radiographs are unable to provide necessary visualization of the soft tissue FFPS in suspected pulley injuries. However, the routine use of radiographs in these patients may be useful to diagnose bony injuries, such as fractures and epiphyseal injuries.54,57
MRI
As with most soft tissue musculoskeletal injuries, MRI can provide valuable information about FFPS injuries. MRI was first demonstrated to be sensitive to diagnose FFPS injuries in the late 1990s and early 2000s; it is now widely accepted as a valid imaging technique for FFPS injuries.42,50,58-60 Healthy flexor tendons have low signal on both T1 and T2 images. 25 A 3T MRI allows direct visualization of the annular pulleys, although the thinner cruciate pulleys are difficult to visualize.25,61
Abnormalities seen on MRI that may be suggestive of FFPS injuries include dehiscence of the flexor tendon from bone, discontinuity of the pulley tendons, hematoma between the phalanx and flexor tendon, and tilting of the flexor tendon toward the ruptured side.16,25 MRI was reported to be 100% sensitive and specific to diagnose A2 and A4 injuries in cadaveric digits. 42
When available, 3T MRI with dedicated surface coils allows for the highest resolution imaging of the digits.25,62 Transverse images using gadolinium-enhanced and fat-saturated T1-weighted sequences provide the best visualization of the FFPS.61,63 The use of crimp grip positioning during MRI evaluation enhances the sensitivity and specificity of pulley injury diagnoses.64,65
Semidynamic MRI of the digits, defined as consecutive images obtained in various degrees of flexion, may aid in the diagnosis of A3 pulley injuries. 66 Because of its insertion onto the volar plate, the A3 pulley places traction force on the volar plate during finger flexion. This force promotes palmar motion of the volar plate, and the distance created is termed the “volar plate translation distance.” Therefore, palmar displacement of the volar plate is dependent on the integrity of the A3 pulley; decreased distances have been used to diagnose A3 pulley ruptures. 67 Volar plate translation distances of <2.8 mm and volar plate-tendon distances of >1.4 mm may be used as thresholds to diagnose A3 pulley ruptures. 56
MRI may be preferred over US in clinical settings when experienced ultrasonographers are not available and when visualization of an injured pulley requires greater than 55 to 60 degrees of PIP joint flexion. MRI has the disadvantage of cost and an inability to provide dynamic imaging of the digits, as US is able to do. Despite its disadvantages, MRI is recommended as an additional imaging study, particularly if US is inconclusive.16,46
Prevention
A structured warm up as part of any rock-climbing session has been shown to increase the amount of physiologic bowstringing of the flexor tendons, specifically in the crimp grip position, by up to 30%. 27 Warming-up in rock climbing involves climbing routes of a less difficult grade than a climber may be able to climb normally. This is analogous to a runner, for example, who may warm-up by running a mile at a slower pace than normal. Specifically, a warm-up of 100 individual climbing moves of increasing intensity increases the amount of physiologic bowstringing. 27 Importantly, this increase in physiologic bowstringing has not been shown to prevent injuries from occurring and is only inferred to do so. Additionally, the author suggests that warming up may make the course of the flexor tendons more even, preventing peak forces at distinct points of the flexor tendon sheath. 27 Therefore, it is recommended to set a goal of 50 moves for each hand, for a total of 100 moves, with increasing intensity, as a proper warm-up to prevent pulley injuries.
When climbers experience discomfort over the area of the pulleys, some may circumferentially tape the affected finger at the level of the pulley in question, with the rationale that this will prevent a pulley injury (Figure 8). However, biomechanical evidence does not support the validity of this concept.49,68 This style of taping decreases the amount of bowstringing by 3% and only absorbs approximately 10% of the force that is demanded from the pulley. 49 Another study found no statistical difference when testing the A2 pulley’s load to failure in digits that were taped, compared with those that were not. 68 These studies used simple inelastic cloth adhesive tape.49,68 Therefore, circumferential taping is probably an ineffective method to prevent injury. Nonetheless, a theoretical positive effect of circumferential taping is that flexion of the PIP joint is limited to less than 80 to 90 degrees if the tape is applied over the PIP joint, which limits the force acting on the A2 pulley. 49

Circumferential taping over the A2 pulley of the third finger of the left hand.
In addition to prevention, taping of the digits around the pulleys is also commonly done after injury. Circumferential taping, H-taping, and figure of 8 taping are 3 different taping techniques used. Their roles following a pulley injury will be discussed in the “Conservative Treatment” section.
Treatment
Less severe injuries of the FFPS allow for relatively unimpaired function and tend to self-resolve after a period of rest. 69 More extensive injuries that do not resolve with rest or that result in functional impairment require treatment. Both conservative and surgical treatment of FFPS injuries can be effective. Until 2003, there were no therapeutic guidelines for these injuries. Table 1 depicts the grading system with an accompanying therapeutic decision tree that was revised recently. 70 Owing to the lack of other literature on therapeutic guidelines, we will focus our discussion on that proposed grading system and treatment strategy.
Pulley injury grading system and therapeutic guidelines (adapted from Lutter et al. 69 )
Conservative Treatment
The majority of pulley injuries are managed conservatively. Conservative strategies include immobilization and rest from climbing, anti-inflammatory agents, physical therapy, and pulley protection using different taping methods or a protective splint. 16
The gradual return to climbing after a pulley injury always should be done under pulley protection. A device called the pulley-protection splint, specifically designed for conservative treatment of pulley ruptures, has shown good clinical results. 49 The device is recommended to be placed shortly after injury and to be worn for 6 to 8 wk. 49 When used correctly, the pulley-protection splint reduced the initial bowstringing at the A2 and A4 pulleys by 50 and 40%, respectively. 49 The device’s unique shape is one of its main advantages over alternative methods, with collateral bulges designed to prevent compression of the surrounding neural and vascular supply of the finger, while still maintaining close apposition of the flexor tendons against the phalanx. 49
The use of inelastic tape is the most widely used method to provide pulley protection after an injury. Taping of the fingers at the level of the A2 and A4 pulleys is thought to act as a replacement bolster for the injured pulleys. It is frequently done both to decrease the strain on an already injured pulley and to prevent further, or new, injury. Three different techniques of taping after a finger flexor pulley rupture have been studied: the circumferential, H-tape, and figure of 8 methods.
Circumferential taping around the proximal phalanx in the area of the affected pulley is only minimally effective in decreasing the demand on the injured pulley. 71 Circumferential taping has a greater, albeit still minimal, effect when the tape is applied over the distal end of the proximal phalanx, as opposed to the proximal end. 72 The figure of 8 method is applied by crossing the tape strips over the PIP on the palmar side of the digit. 71 Figure of 8 taping does not reduce the tendon-to-bone distance significantly. Therefore, the circumferential and figure of 8 taping methods are not recommended as a conservative treatment after pulley injury. 71
The H-tape method has shown promising results in restoring the normal tendon-to-bone relationship and strengthening the injured finger. 73 The H-tape method focuses on placing tape circumferentially around the digit at the level of the A3 pulley in finger flexion (Figure 9). This method decreased the tendon to bone distance by 16% in an injured finger and is the only taping method to reach a statistically significant difference. The H-taping method also resulted in a 13% increase in strength of the injured fingers in the crimp grip position, compared to other taping methods. 73 Leukotape was used in this study. 73 Taping of the injured finger with the H-taping method should be done for 3 mo in grade I to III injuries and for at least 12 mo in grade IV injuries.
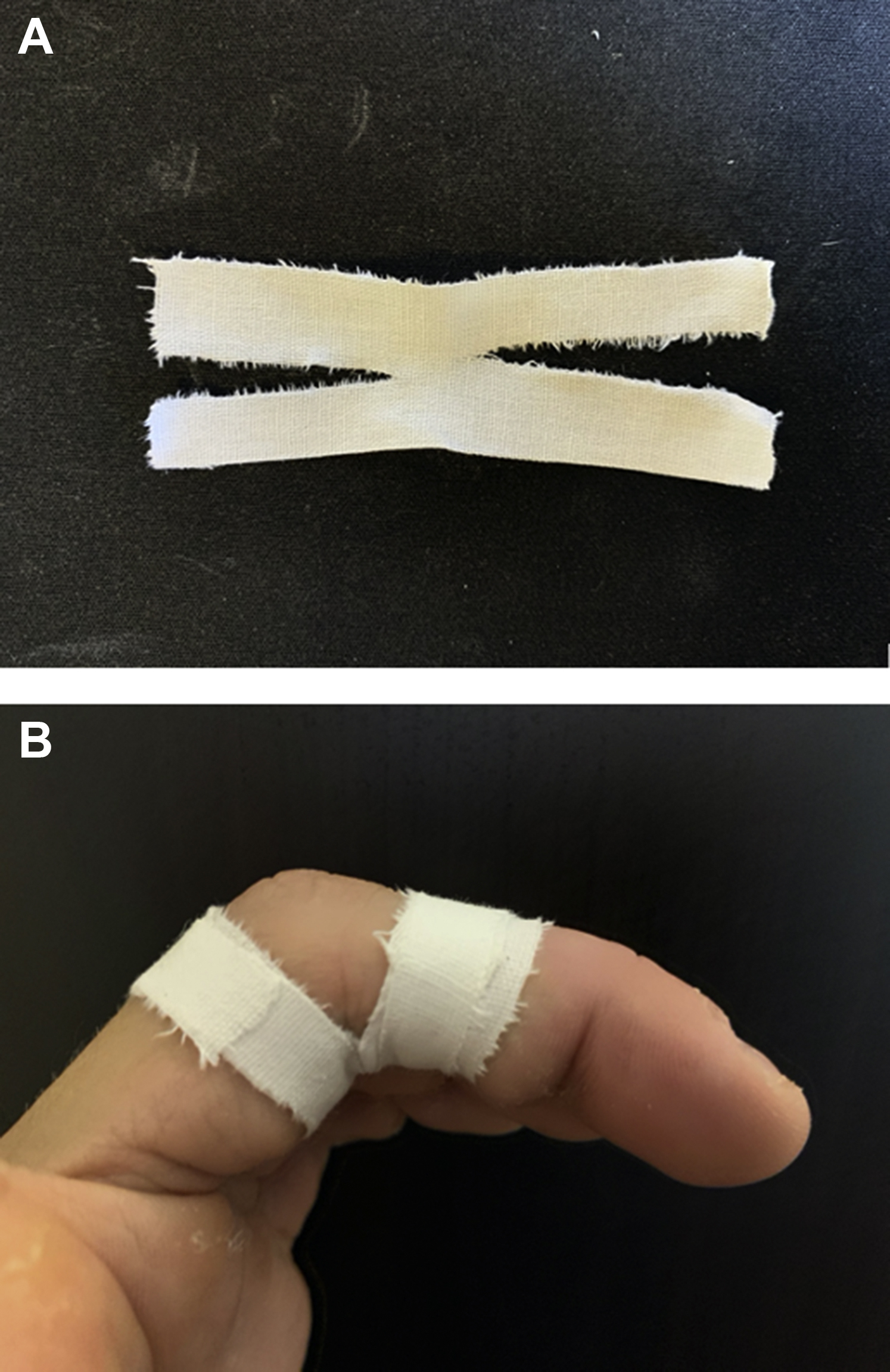
The H-tape before (a) and after application (b) on the third finger of the left hand.
The H-tape method is the only method that has been shown to be effective in decreasing the tendon-to-bone distance and increasing the strength of the injured finger. 73 It is recommended after a pulley injury. 73 There is no evidence to support the use of H-taping for prophylaxis of these injuries, however.
Surgical Treatment
Surgical repair of pulleys is reserved for patients with multiple closed pulley ruptures, persistent pain, or dysfunction after 2 mo of conservative management, or when there is a flexion contracture as a result of the pulley injury. 74 These are all grade IV injuries, according to the aforementioned grading system. Although surgery is the acknowledged treatment of choice for grade IV injuries, occasionally they can be managed conservatively.
Surgical repair restores the tendon to joint relationship, while also providing good biomechanical outcomes. 75 Several different pulley reconstruction techniques have been described, including the “belt-loop,” the “single loop,” the “loop and a half,” and the “triple loop” techniques. 76 -79 Pulley reconstructions are performed with grafts, or most commonly with a combined repair technique. 80 -82 Nevertheless, these encircling techniques can lead to atrophy of the cortex of the proximal phalanx. 83
Postoperative care generally includes immobilization via a ring splint, such as the pulley-protection splint. The duration for ring splinting is not well defined, with recommendations ranging from 14 d to 6 wk.57,79 We recommend full arm and finger splinting for 2 wk after surgery, followed by 4 wk of pulley splinting. Recommendations regarding when to initiate finger motion therapy and the use of postoperative supportive taping vary widely.68,72,73
Summary
FFPS are the most commonly diagnosed overuse injuries in rock climbers. FFPS injuries have increased over the past 2 decades as a result of the sport’s sustained growth and popularity. The crimp grip used in rock climbing is the mechanism for these injuries, due to the supraphysiologic demand of the annular pulleys in this position. The A2, A3, and A4 pulleys are at the highest risk of injury, especially when loaded eccentrically.
Evidence of FFPS injuries on physical examination includes tenderness over the anatomic pulleys when the patient reports pain and, in some cases, clinical bowstringing. Physical examination of a suspected FFPS injury often is clouded by limited range of motion and soft tissue swelling. For these reasons, physical examination alone is insufficient for diagnosis and extent, hence the need for imaging.
Imaging evaluation permits visualization of the FFPS and is imperative to establish the correct diagnosis and extent of injury. US is the preferred initial imaging technique for suspected injuries of the FFPS system because it is highly sensitive and specific and provides direct visualization of the structures in question in a dynamic fashion. MRI is the recommended additional imaging study if US is inconclusive.
Warming up appropriately is critical and is the only approach thought to prevent injuries of the FFPS. 27 Treatment of grade I to III injuries generally is conservative, with surgical intervention reserved for grade I to III injuries that are refractory to treatment, or any grade IV injury not amenable to conservative treatment. The use of the pulley protective splint or taping the digits in the H-tape method after injury decreases the likelihood of further injury and provides adequate support to the damaged pulleys. In surgical cases, the involved digit should be immobilized and splinted for at least 2 wk postoperatively, and many authors recommend even longer durations of splinting.
Footnotes
Acknowledgements
Author Contributions: Study concept and design (PM, Ev); acquisition of the data (PM, DS); drafting of the manuscript (PM, Ev, DS); critical revision of the manuscript (PM, Ev, VS, DS); approval of final manuscript (PM, Ev, VS, DS).
Financial/Material Support: None.
Disclosures: None.