
Abstract
Introduction
Seattle Mountain Rescue (SMR) is a nonprofit, volunteer organization that provides mountain rescue services in King County, Washington. This study analyzed the medical care provided by SMR over 14 y to understand the challenges in patient care in the region and to perform data collection and monitoring.
Methods
A retrospective review of mission reports submitted from 2004 to 2017 was conducted. Date, location, demographics, activity, callout reason, chief complaint, treatments provided, extraction means, and helicopter utilization were analyzed. Data are presented as mean±SD, with range as appropriate, unless otherwise noted. Linear regression was used to estimate changes in mission volume over time.
Results
There were 552 missions involving 756 subjects during the study period. Mission totals increased by 4 (95% CI 2–6, P<0.001) per year. Four locations accounted for 38% of mission volume. Subject age was 36±18 y, and 59% of subjects were male. The most common activity leading to rescue was hiking (80%). Injuries or illness precipitated 58% of callouts, whereas lost, stranded, or overdue subjects comprised 40%. For subjects requiring medical treatment, 81% involved a traumatic injury, 64% were packaged in a litter, and 35% required splinting.
Conclusions
The frequency of mountain rescue missions in King County, Washington, has increased in the past 14 y, with traumatic injuries most frequently requiring medical care. Missing data were common in most categories, and nonstandardized reports challenged research efforts. This study provides a baseline for future research and data collection and adds to the literature regarding the medical care provided during mountain rescue incidents.
Introduction
The Seattle metropolitan area is 87 km west of Snoqualmie Pass, the lowest and most heavily traveled pass 1 through the Cascade mountain range that divides Washington State. This highway corridor affords Seattle’s growing community of outdoor enthusiasts 2 year-round access to hundreds of thousands of acres of national forest. 3
Seattle Mountain Rescue (SMR) is a nonprofit, volunteer, county-based search and rescue organization accredited with the national Mountain Rescue Association (MRA). 4 SMR provides remote and extended care to subjects in need, specializing in technical and mountain rescue. Care is generally at a basic life support level. The majority of SMR volunteers have wilderness first aid or wilderness first responder level training. Search and rescue (SAR) is administered by the King County Sheriff’s Office (KCSO); sheriff’s deputies are responsible for coordinating resources for search, rescue, and recovery incidents in the county. SMR is 1 of 8 volunteer rescue resources managed by KCSO; depending on the needs of a rescue, multiple agencies may be involved. SMR is the only county resource that provides technical rescue in mountainous terrain. SMR also responds to requests from nearby jurisdictions, such as Mount Rainier National Park, when those entities request additional support beyond their own resources.
SMR maintains an electronic database of archived mission reports dating back to 2004. Reports are prepared by team members who respond on the mission in question and are kept on a password-protected server. They contain information including location and responder lists and a narrative of the mission logistics, rigging operations, and medical care. This study was undertaken with the goal of analyzing the types and frequency of medical care provided by SMR and to understand the epidemiology of mountain rescue in an area with increasing numbers of outdoor recreationalists.
Methods
Archived reports for SMR missions from January 1, 2004 through December 31, 2017 were accessed via a secure web portal available only to SMR members. Evidence searches (requests by law enforcement to search terrain for items pertaining to a criminal investigation), missing persons in urban areas, animal rescues, body recoveries, and turn arounds (incidents in which SMR personnel turned around before making subject contact) were excluded from the analysis because they do not provide an opportunity for SMR to administer medical care. Total mission callout numbers for the same years were also extracted from the online King County Search and Rescue Association (KCSARA) database for comparison with mission reports pulled from the SMR web portal to determine if reports were missing from the SMR electronic database. Data were extracted from the SMR mission reports by the authors into a predesigned data collection form in Microsoft Excel. No patient-level identifying data were contained in the SMR database. The University of Washington human subjects division determined this study to be exempt research.
Data collected included date of mission, mission identification number, location, number of subjects involved, subject(s) age and sex, activity at time of incident, callout reason, primary chief complaint, medical treatments provided, means of extraction, nature of subject handoff, use of technical rescue, and helicopter involvement. Each author coded one-fourth of the reports. Each author also individually coded the data of 2 other authors; any discrepancies in coding were resolved by discussion between authors. The data were then collated into descriptive statistics and analyzed using Microsoft Excel IBM SPSS, version 22 (Armonk, NY). A linear regression model was applied to the annual mission data to determine the average increase in total number of missions over the study period. The frequency of missions based on months of the year and days of the week was compared using the general z-test for proportions. Statistical significance was indicated by a 2-tailed alpha level ≤0.05. Data are presented as mean±SD, with range as appropriate, unless otherwise noted. Maps were rendered using Google Earth Pro (version 7.3.2.5491).
Results
A total of 1425 SAR missions were recorded in the KCSARA database from 2004 through 2017. This includes all SAR missions called in through KCSO. For 60% (851 of 1425) of these missions, SMR was involved, as evidenced by a county mission identifier with SMR listed as a responding SAR team. Of these missions, 552 were included in this analysis, representing 65% of all recorded SMR missions during the study time frame; 299 missions were excluded based on a priori criteria (Figure 1). Among these 552 missions, 23% involved multiple subjects; there were 756 subjects in total on the included missions. Of those for which sex was recorded (72%), 59% were male and 41% were female, with an age of 36±18 (8–81) y. The summer months of July and August were the busiest (z=4, P<0.001), and weekends had the highest mission counts throughout the year (z=2, P=0.04). Over one-third (38%) of SMR missions occurred in 4 popular hiking destinations: Mount Si (12%), Rattlesnake Ridge (11%), Mailbox Peak (10%), and Tiger Mountain (5%) (Figure 2).
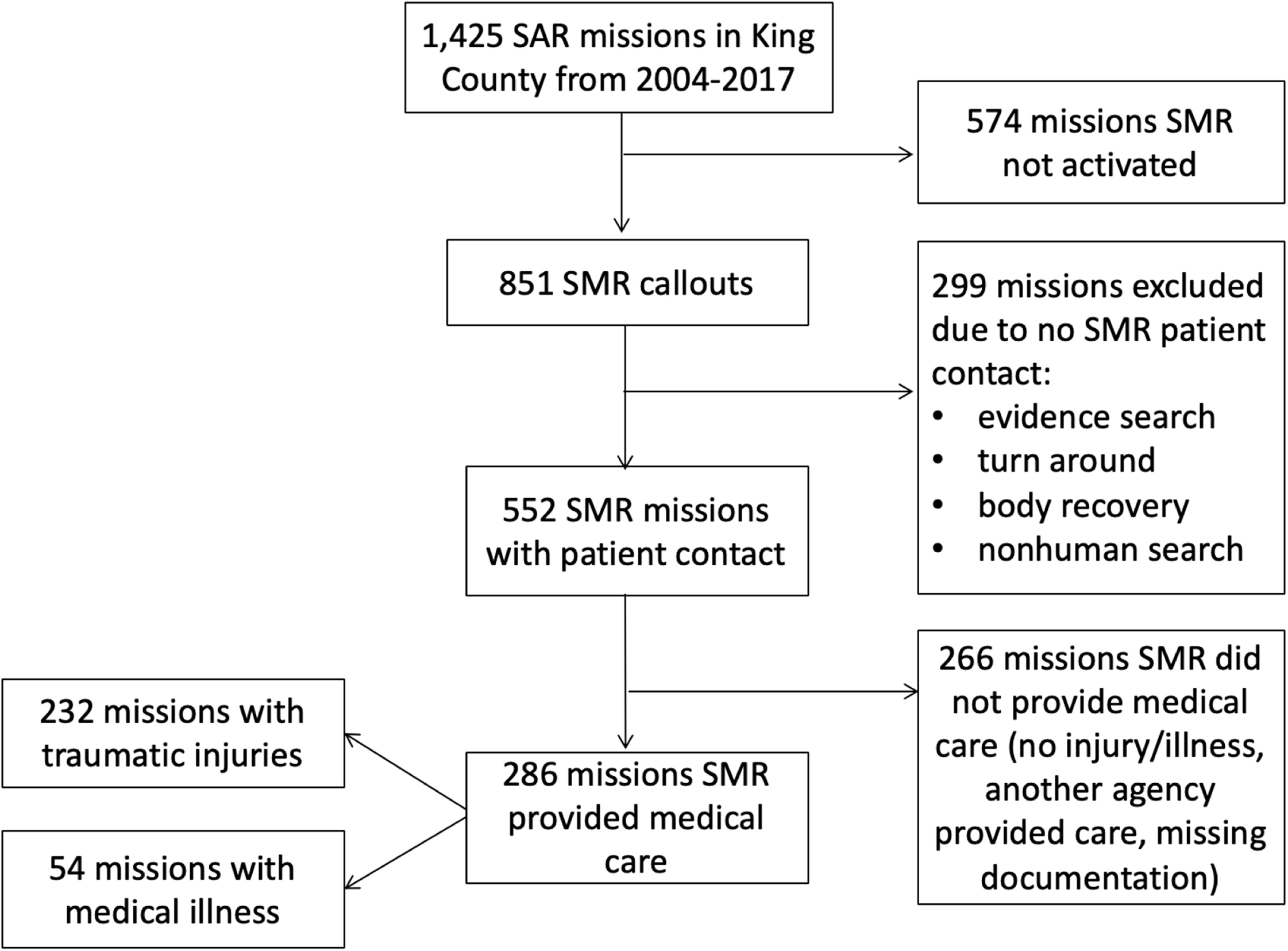
Flow chart of included missions.
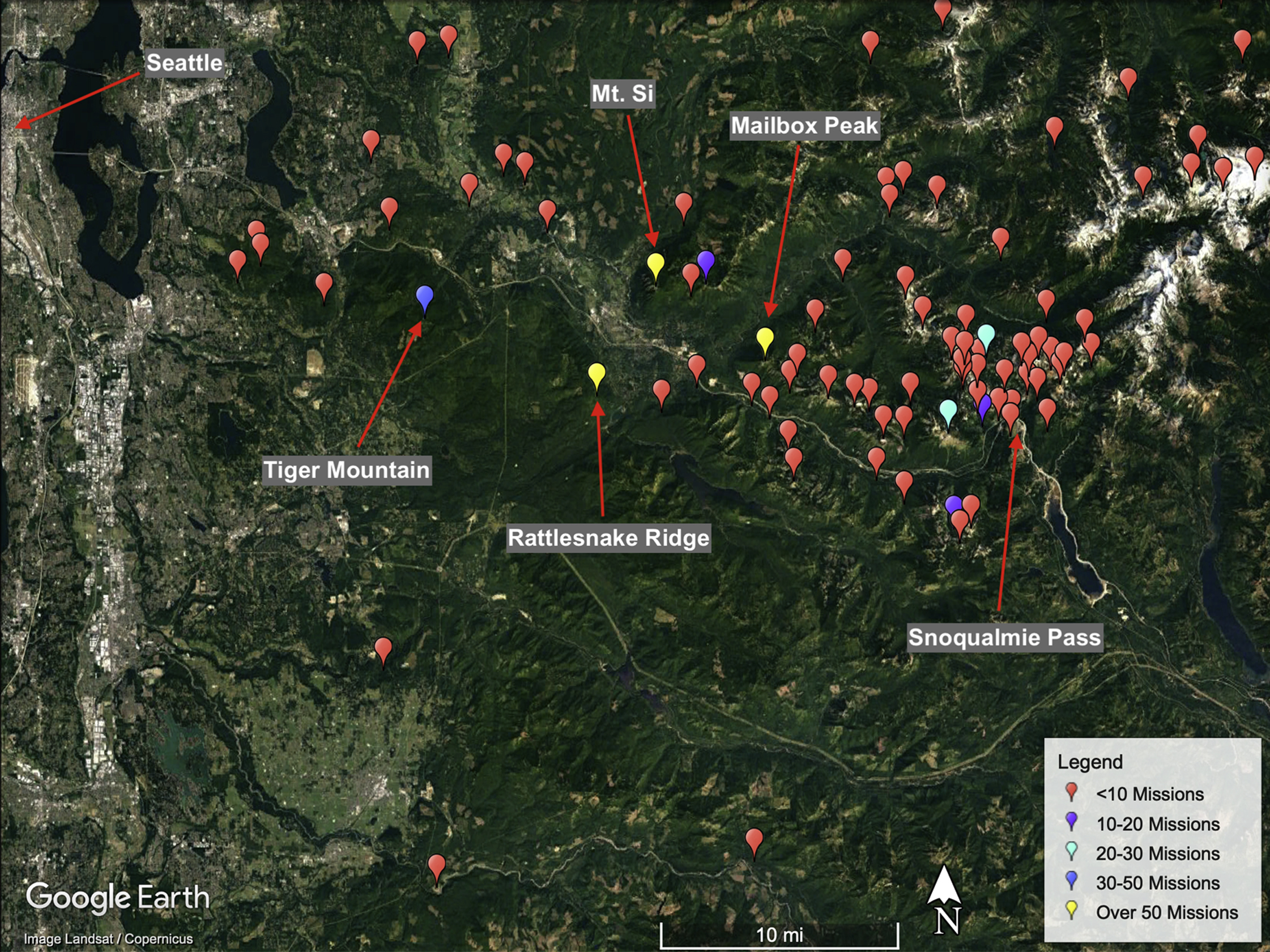
Seattle Mountain Rescue geographic mission distribution 2004 through 2017.
The number of missions per year from 2006 to 2017 was 45±16 (23–74), with an estimated increase of 4 missions per year by linear regression model (95% CI 2–6, P<0.001) (Figure 3). For this analysis, 2004 and 2005 data were excluded because only 10 reports were archived during this time period, indicating multiple missing mission reports based on comparison with the KCSARA mission numbers for those years.
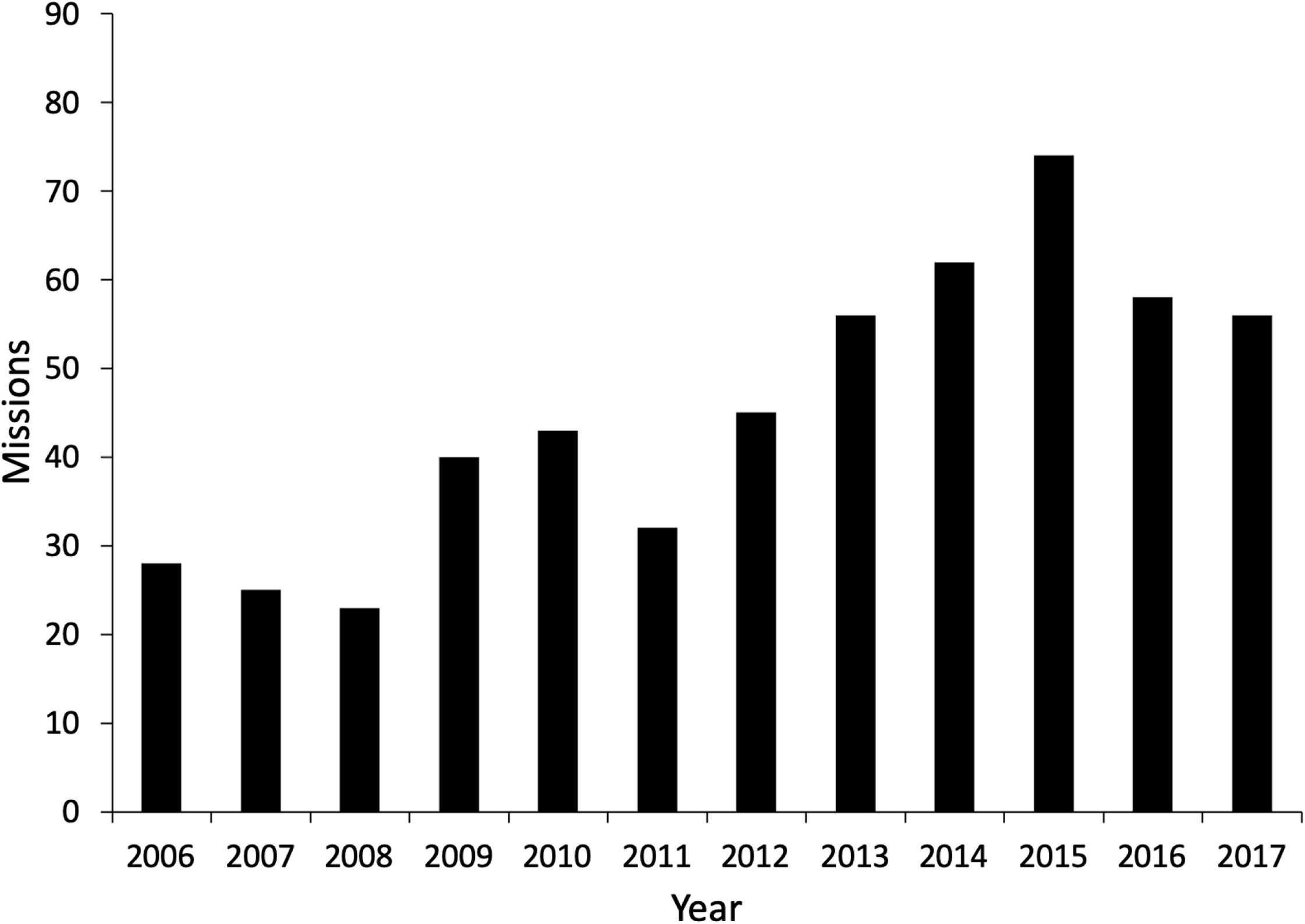
Seattle Mountain Rescue mission trend 2006 through 2017.
The majority of missions were for hikers (80%; Table 1). Other activities included climbing (8%), backcountry skiing or snowboarding (3%), motorized vehicle usage (2%), snowshoeing (1%), and mountain biking (1%). Of the included missions, 98% have a listed callout reason (Table 2); 261 missions (47%) were paged out for a traumatic injury, 26% for lost subjects, 11% for medical illness, 9% for stranded subjects, and 5% for overdue subjects.
Outdoor activity of subjects involved in SMR missions
Callout reasons for SMR mission requests
SMR provided documented medical care on 52% (286 of 552) of the included missions. The remaining missions featured lost or stranded subjects who were uninjured or injured subjects for whom medical care was managed by a different organization. For these missions in which SMR provided medical care, chief complaints are listed in Table 3. Traumatic injuries (81%) significantly outnumbered medical illness (19%). Of all traumatic complaints, 79% involved an injury to an extremity. Among medical complaints, heat injury/dehydration was the most common (32%), followed by cardiac complaints (15%) and general malaise (13%). For the missions on which SMR provided medical care, 64% of patients were extricated by patient packaging in a litter, 35% involved splinting or immobilization, and only 1% involved oxygen administration of advanced life support care.
Types of injuries and illness treated by Seattle Mountain Rescue
Of the included missions, 113 (14%) involved a helicopter in some capacity. The majority of these missions (69%) involved hoist operations, <1% involved short-haul operations, and the remaining 30% included helicopter use for searching, transporting resources, or aborted flights.
Discussion
This study represents an effort to quantify and understand the evolution of mountain rescue medical care and mission volume in an area known for outdoor recreation that is experiencing rapid population growth. Our data show that the number of SMR missions has increased since 2006, correlating with the significant increase in the Seattle metropolitan population during this same time period. 5 A 2017 study also reported an increase in Seattle-area hikers, which roughly doubled from 2008 to 2017; 41% of adults in the survey said they had hiked at least once in the past year in 2017. 2 Although the total number of wilderness users in King County is unknown for this time, the data suggest that there has been an increase in mountain rescue missions along with an increase in population and outdoor users.
The MRA maintains a national database of mountain rescue missions; this database offers a comparison with other teams in western Washington. In 2017, Everett Mountain Rescue Unit, Olympic Mountain Rescue, and Tacoma Mountain Rescue were the next 3 busiest teams in Washington with 69, 60, and 13 missions, respectively, entered into the MRA database. 6 In comparison, SMR was involved in 104 missions in 2017 (only 56 of which met criteria for inclusion in this study). The fidelity of these data is reliant on volunteer members submitting data regarding mission volume to the MRA, however, so there may be higher numbers of callouts and actual patient care occurring. In addition, the type of missions for which each team is called is unclear (eg, how many reported missions are mountain rescues vs urban searches for lost people or body recoveries).
In our study, the sex discrepancy between subjects (59% male and 41% female) and the subject age (36±18 y) generally correlates with data published in other descriptive studies of mountain rescue operations in the United States.3,7 It is impossible to know if men pursuing outdoor recreation are injured more often than women on average, as we do not have a total number of users by sex, but it does inform rescuers that their typical subject is a male in his 30s. Likewise, summer weekends being the most popular time for mountain rescue missions likely reflects the underlying number of wilderness users at that time, and the top locations for missions correlate with popular and accessible trailheads in our region. The fact that 4 trailheads account for over one-third of SMR’s missions during the study timeframe supports anecdotal evidence that mountain rescue “hotspots” exist. Understanding local hotspots can help stakeholders work together to both prevent and respond to events in the most expedient and effective way and can inform public education and outreach. Preventative Search and Rescue (PSAR) programs may help reduce future calls and allow rapid access to subjects at peak times; Grand Canyon National Park, for example, has continued to demonstrate an overall decrease in SAR operations since implementing a PSAR program in 1997. 8
Hiking (80%) was the most frequent activity during which a rescue was needed. This finding is consistent with a 2005 study of wilderness recreational injuries in Washington State that found hiking and camping (61%), snow activities (15%), and mountaineering (12%) to be the most common activities leading to injury. 9 Large groups of users should be a main focus of education and prevention efforts in any given area. Therefore, hikers should be targeted in King County for PSAR efforts because they represent the majority of mountain rescue missions, even if the total percentage of hikers needing rescue may be low.
The majority of patient care missions (81%) were for a traumatic injury, which has implications for training, equipment, and operations. For example, with 79% of all traumatic injuries involving an extremity, it is likely that every member of SMR will encounter a subject with this chief complaint on at least a few missions per year. As such, each team member is trained in extremity immobilization and first aid, as well as patient packaging for such injuries. An analysis such as this can give mountain rescue medical leadership a clear picture of the topics on which to focus for core competencies.
Limitations
In general, this study is limited by the retrospective analysis of nonstandardized mission reports from a single, regional mountain rescue team. Up to 30% of some variables of interest were missing from mission reports over this time period. In addition, the early years of electronically archived mission reports do not appear to reflect the true number of missions SMR attended, which limits the conclusions we can draw from 2004 and 2005. Finally, missions in which SMR was turned around before contacting the subject may indeed have included ill or injured patients, such as a subject for whom SMR was responding on foot who was then rescued via helicopter before ground teams arrived; thus, although the 552 missions included in this study are an accurate representation of the patient care incidents in which SMR was involved from 2004 through 2017, they do not represent the complete set of backcountry incidents and rescue responses in King County during this time frame. Even on missions in which SMR did respond, another resource may have provided medical care to an ill or injured subject that was not recorded in SMR’s mission report and thus not captured in our dataset. Data are difficult to compare across the region because there is no standardized data reporting or centralized repository, and different numbers may be reported on team websites, local press, and other sources (eg, total mission callouts vs actual missions on which the mountain rescue team encounters a live patient in mountainous terrain). Finally, our data are based on the medical observations of first responders; outcomes for patients were not known, and actual injuries may have differed from the impression of rescuers at the scene.
The difficulty of determining accurate descriptions of injuries and illnesses encountered and medical care provided by SMR led the authors to design and implement a new standardized patient care report (see online Appendix 1) that is used by all field members, regardless of their level of medical training, to capture pertinent mission and medical data. This is an example of the impact of the study on the team. Although true patient follow-up with hospital medical records and outcomes will still be a challenge, standardized medical documentation will increase the level of professionalism and research potential in the future.
Conclusions
This study represents an effort to quantify the medical care provided by a mountain rescue team covering a region known for its outdoor recreation opportunities. Mission volume is increasing, and medical care is provided on a majority of mountain rescue missions, with traumatic injuries being the most common reason for encounter. Having robust data collection from standardized patient care reports is important for any team providing medical care; mountain rescue organizations are no different. With this dataset and analysis in hand, the medical leadership for SMR has made specific advances, such as implementing a standardized patient care report. Our research methods and organizational changes may be generalizable to similar mountain rescue teams throughout the world.
Footnotes
Acknowledgements
Author Contributions: Study concept and design (MJM, BAF, GEW, AEC); acquisition of data (MJM, BAF, GEW, AEC); drafting of manuscript (MJM, AEC); critical revision of the manuscript (MJM, BAF, GEW, AEC); and approval of final manuscript (MJM, BAF, GEW, AEC).
Financial/Material Support: None
Disclosures: All four authors are SMR members. AEC and MJM are board members for the Pacific Northwest Wilderness Medicine nonprofit organization. GEW is a flight paramedic for the King County Sheriff’s Office. MJM is a member of Everett Mountain Rescue Unit and the Snohomish County Helicopter Rescue Team.
Supplementary data
Supplementary material associated with this article can be found in the online version at
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.