
Abstract
Objectives
To investigate whether a traction splint made from improvised materials is as efficacious as commercially available devices in terms of traction provided and perceived comfort and stability.
Methods
This was a prospective randomized crossover study utilizing 10 healthy, uninjured volunteers. The subjects were randomized to be placed in 4 different traction devices, in differing order, each for 30 minutes. Three of the traction splints are commercially available: The HARE, Sager, and Faretech CT-EMS. The fourth traction device was an improvised splint made as described in Medicine for the Backcountry: A Practical Guide to Wilderness First Aid. At the end of 30 minutes the pounds of force created by each device was measured. The volunteers were also asked at that time to subjectively report the comfort and stability of the splint separately on a scale from 1 to 10.
Results
All traction splints performed similarly with regard to the primary outcome measure of mean pounds of traction created at the end of 30 minutes of application with results ranging from 10.4 to 13.3 pounds. There was little difference reported by participants in regard to stability or comfort between the 4 traction devices.
Conclusions
In this small pilot study, an improvised traction splint was not inferior to commercially available devices. Further research in needed in this area.
Introduction
In wilderness and austere environments far from definitive medical care, a femur fracture is a potentially life-threatening injury. Long bone fractures can cause significant blood loss, and the high force mechanisms associated with such injuries frequently result in multisystem trauma. Femur fractures in remote settings also can require significant resources to stabilize, package, and evacuate the patient.
First developed for treatment of mid-shaft femur fractures in 1860 by Hilton and further refined by Thomas, traction splints gained recognition in World War I when they were reported to decrease mortality from 80% to 15.6%. 1 Since 1961, the American College of Surgeons (ACS) has mandated that all ambulances in the United States carry traction splint devices. 2
This recommendation currently is jointly endorsed by the ACS and the American College of Emergency Physicians. This practice has carried over to wilderness and remote settings, with the construction and placement of improvised traction splints being promoted in most wilderness medicine textbooks.
Despite the fact that traction splint placement is considered the standard of care, there are no definitive studies demonstrating efficacy or decreased morbidity or mortality from their prehospital application. Similarly, there is no research supporting use of improvised splints in the wilderness. The potential benefits of traction splints are thought to include decreased pain and amount of potential bleeding space in the thigh; stabilization and realignment of the fractured bony ends; and diminished soft tissue injury including progression to an open fracture. 3 Recent authors have questioned the utility of traction splints in the prehospital setting, citing occurrences of inappropriate application, skin ulcerations, peroneal nerve injuries, and increased on-scene time for emergency medical services (EMS) crews with subsequent delay to definitive care. 1 ,4,5 The Wilderness Medicine Society's most recent Practice Guidelines for Wilderness Emergency Care in 2006 even stated, “a traction splint is no more efficacious than a good packaging technique.” 6
Clearly, there is controversy regarding the risks and benefits of the use of traction splints in the prehospital setting, and the debate regarding the use of these devices is not well supported on either side by recent research. Improvised traction splints in the wilderness setting take some knowledge and time to create and should only be used if they can be shown to be efficacious.
The goal of this pilot study is to investigate whether a traction splint made from improvised materials is not inferior to commercially available devices in terms of traction provided and perceived comfort and stability.
Methods
This was a prospective randomized crossover study using 10 healthy, uninjured volunteers. Subjects were recruited using e-mail and posted notices to employees and residents at Community Regional Medical Center and the University of California, San Francisco—Fresno Medical Education and Research Center. Only individuals older than 18 years of age, who self-reported being in good health and who were capable of signing informed consent, were eligible to participate in the study. Once the 10 selected subjects were educated on the specifics of the study and had signed the consent form, they were randomly assigned to be placed in 4 different traction devices, in differing order, each for 30 minutes. Traction splints were consistently placed on the same leg within subject testing. Three of the traction splints are commercially available: the Hare, Sager, and Faretech CT-EMS. The Hare and Sager traction splints are frequently used in urban and rural prehospital settings and in the emergency department. The Faretech CT-EMS is a more lightweight device designed for use in remote settings including search and rescue and ski patrol. The fourth traction device was an improvised splint made as described in Medicine for the Backcountry: A Practical Guide to Wilderness First Aid. 7 Creation of this splint involved using a strip of something long and soft to tie around the ankle with a loop at the sole of the foot, securing a shaft that is at least 1 foot longer than the injured leg to the patient's upper thigh with a strap of material that is well padded, and using a piece of rope or cord to make a trucker's hitch that is pulled from the loop at the sole of the foot and the end of the shaft until traction is achieved. 7 For our study, we used a 1-inch webbing for the foot strap, a 4-foot (1.22 m) stick as a shaft, and a 1-inch webbing for the leg strap with a Prusik knot with cord at each end. A similar cord was used to create traction.
Three of the commercial traction splints were applied to the volunteers by one of the principal investigators following the instructions provided by the manufacturers of the devices. 8 –10 The improvised traction splint was constructed and applied by the same investigator for consistency in application. All subjects were monitored through the study period and were instructed to notify an investigator at any time if a traction device became too uncomfortable, at which time the splint would be removed.
At the end of 30 minutes, an inline Lewis N Clark BZ200 digital scale (Balanzza, Miami, FL) was placed on each traction splint to measure the pounds of force created by each device. The volunteers were also asked at that time to subjectively report the comfort and stability of the splint separately on a scale from 1 to 10. For comfort, 1 was equal to nothing noticeable on the leg, and 10 was the rating for the splint being unbearable. The scale for stability ranged from 1, meaning no added stability, to 10 representing complete immobilization of the leg. Subjects were also asked to report any perceived side effects such as pain or paresthesia.
All collected data were entered into an Excel (Microsoft Corp, Redmond, WA) spreadsheet, where mean and standard deviation were calculated. This information was then imported to SAS (SAS Institute Inc, Cary, NC), where means were compared and 95% confidence intervals were determined.
This study was approved by the Community Regional Medical Center institutional review board.
Results
The mean age of the 10 study participants was 27 years, and there were 5 women and 5 men. The mean weight of the participants was 72.7 kg (160 pounds). All traction splints performed similarly with regard to the primary outcome measure of mean pounds of traction created at the end of 30 minutes of application, with results ranging from 10.4 to 13.3 pounds. The mean pounds of traction created for each device with the 95 % confidence intervals listed in parentheses were Hare traction, mean of 13.3 (2.56); Sager splint, mean of 10.8 (3.33); Faretech CT-EMS, mean of 10.4 (2.85); and improvised splint, mean of 11.6 (3.77). There was little difference reported by participants in regard to stability or comfort among the 4 traction devices (Figures 1 and 2, respectively).
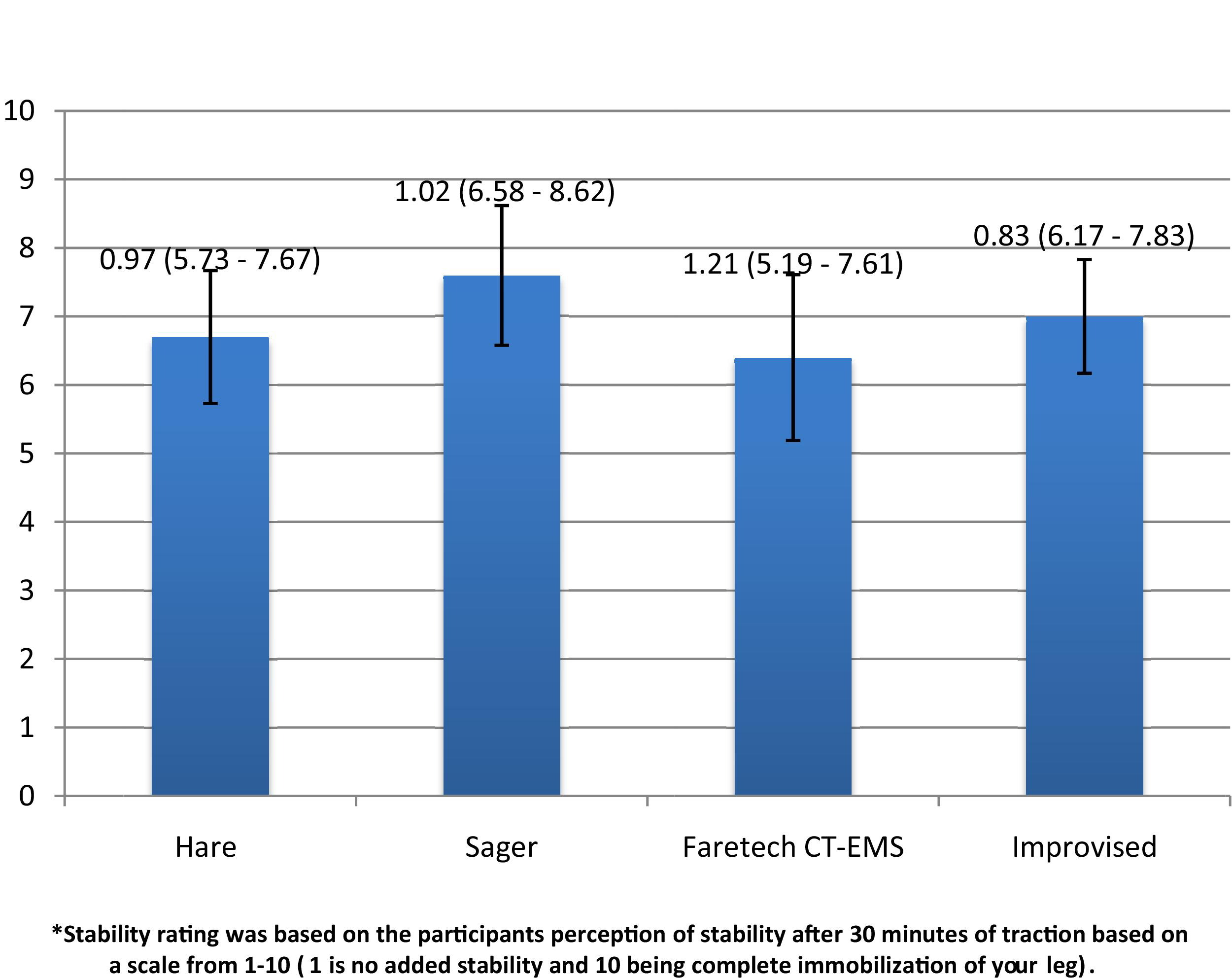
Subjective stability rating for traction devices on a scale of 0–10 (mean is graphed with bar representing 95% confidence interval).
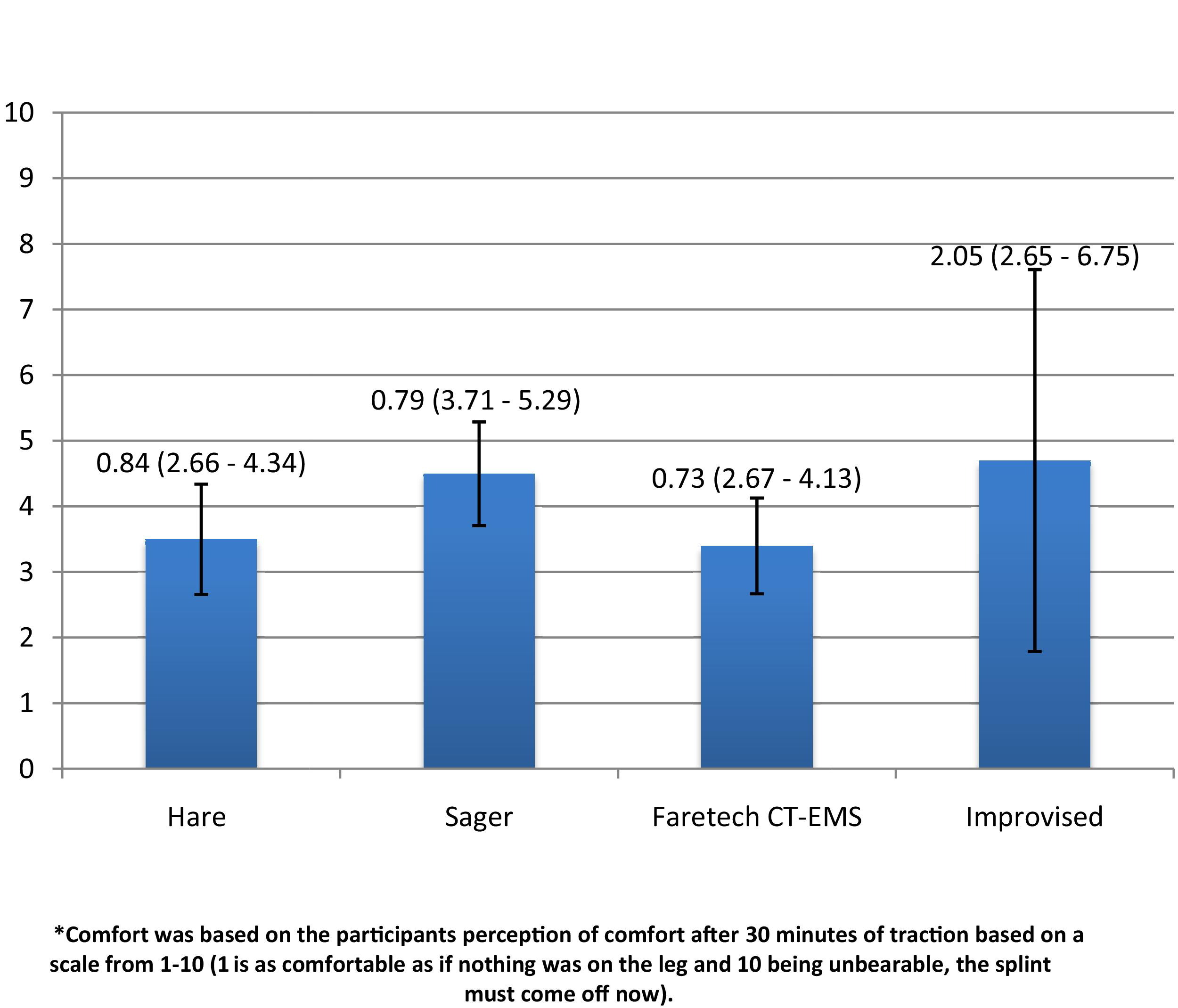
Subjective comfort rating on a scale of 1–10 (mean is graphed with bar representing 95% confidence interval).
The majority of side effects reported by volunteers occurred with the Faretech CT-EMS (8 of 10 subjects) followed by the Sager splint (7 of 10 subjects). The least number was reported with the improvised splint (2 of 10). The 3 most commonly reported side effects were pain in the ankle, pain in the hip, and numbness in the foot. No side effect was so severe that the subject requested early removal of a traction device.
Discussion
Our study suggests that an improvised traction splint is not inferior when compared with 3 commercially available traction devices in healthy and uninjured volunteers, both in regard to measured pounds of traction created and with respect to subjective evaluations of stability and comfort.
Guidelines for the application of traction splints recommend applying a force equal to 10% of the body weight of the patient not exceeding 15 pounds. A recent study of the Hare traction splint showed that 30 minutes after application only half of the initial traction force remained. 4 At 30 minutes in our study, all of the splints tested had an applied traction of at least 10 pounds or 7.4% of the mean volunteer body weight. These results were achieved while also scoring good subjective evaluations of stability and comfort with limited reported side effects.
Limitations
This study is a first step at looking at the efficacy of improvised traction splints in the wilderness setting. Its results are limited by the small size of the study, the use of healthy, uninjured volunteers, and the fact that the commercially available devices that the improvised splint is being compared with have not been well validated. Further limitations include that these devices were not subject to the prehospital and wilderness environments of long carries and transfers that might reveal instabilities of these devices not recognized in the more controlled environment of this study.
Further areas that need to be investigated include elucidating the role of commercially available traction splints in the wilderness, rural, and urban prehospital settings; comparing improvised traction splints with good packaging techniques in the wilderness setting; evaluation of the stability of these devices in long transports and transfers; and further clarification of the potential side effects of these devices, especially during long transports.
Conclusions
In this small pilot study, improvised traction splints were not inferior to commercially available devices. Further research is needed in this area including, but not limited to, how these devices hold up during prolonged transport and transfer scenarios that are common to wilderness settings.