
Abstract
Upper extremity injuries are common among the growing population of climbers. Although conditions affecting musculoskeletal structures are the most common causes of symptoms, a comprehensive differential diagnosis is necessary to avoid the misdiagnosis of high-morbidity conditions in this patient population. We present a case of a climber with acute edema, erythema, and pain of the entire right upper extremity. After confirmation of an upper extremity deep vein thrombosis by ultrasound, and in the absence of secondary causes for his thrombotic process, he was diagnosed with effort thrombosis. The patient was treated acutely with anticoagulation, catheter thrombectomy, direct thrombolysis, and balloon angioplasty followed by surgical decompression of the subclavian vein. Owing to the importance of early diagnosis and initiation of treatment, it is critical to keep disorders affecting the upper thoracic vascular structures in consideration.
Keywords
Introduction
Recreational climbing continues to grow in popularity worldwide, and the rescheduled debut of climbing as an Olympic sport is expected to draw additional attention to the activity. 1 Alongside this increase in the climbing population, US emergency departments have seen an increase in climbing-related injuries. A total of 40,282 patients with rock-climbing related injuries were seen in US emergency departments between 1990 and 2007, at an average of 2237 injuries per year; a total of 34,785 were seen in US emergency departments between 2008 and 2016 alone, at a considerably higher average of 3816 injuries per year.2,3
Due to the unique set of risks associated with each subdiscipline, climbing injuries tend to vary by setting. For example, lower extremity injuries caused by falls are predominant in traditional alpine climbing, 4 in which individuals must place their own protective gear on outdoor rock, snow, or ice formations. Upper extremity injuries are more prevalent in indoor climbing, in which individuals scale human-made walls with fixed and bolted protection; they account for 42% of the injuries sustained during indoor climbing. 5
A majority of climbers participate in indoor sport climbing, so healthcare providers must be aware of the potential mechanisms through which indoor climbers may injure an upper extremity. Although strain injuries account for most upper extremity-related complaints incurred while climbing,6,7 a comprehensive differential diagnosis is necessary to avoid the misdiagnosis of high-morbidity conditions in this patient population.
Case Presentation
A 38-y-old male recreational climber, right-arm dominant and with a surgical history of left shoulder labrum repair, presented to a tertiary care emergency department with the chief symptom of right arm pain and swelling. Two days before arrival, the patient felt a vague, asymmetric, and dull bilateral ache in his shoulders, biceps, and forearms after an indoor lead climbing session at a local gym. Although the patient initially found this pain similar to post-workout discomfort, he noticed that his right side felt more “pumped” than his left (“pumped” is a common term used by climbers to refer to muscle fatigue in the upper extremities). The dull pain in his right arm progressed in intensity over the next several hours. By the following morning, he noticed swelling and erythema of the entire right upper extremity. He remained able to use his arm, however, and experienced no difficulty with activities of daily living. Moving through his joints’ range of motion did not exacerbate the pain. Inability to find relief with rest, ice, and elevation throughout the day ultimately brought him to the emergency department.
The patient denied significant lead falls during his climbing session, and he denied acute strain or direct trauma to the arm. A review of systems was negative for fever, dyspnea, chest pain, lower extremity edema, and rash. His social history was positive for smoking, but he denied recent travel, allergies, and the use of the use of intravenous drugs, prescribed medications, and hormonal medications. He had no family history of malignancy or coagulopathies.
The patient’s physical examination revealed a young male in no acute distress and with normal vital signs. His right upper extremity had subtle edema and erythema, extending from the proximal humeral head through the distal radius. The venous structures in his chest and shoulder were not distended, nor was there tenderness on palpation of the cervical spine, clavicle, shoulder, arm, or forearm. There was no adenopathy or mass in the supraclavicular space or the axilla. The active and passive range of motion of his right shoulder, elbow, and wrist were intact. Axial loading of the spine did not exacerbate his pain. Both his superficial sensation to light touch and his reflexes were normal. He exhibited equal arm strength bilaterally, as well as symmetric radial and axillary pulses.
A venous thrombotic syndrome was suspected owing to the edema involving his entire right upper extremity. A duplex venous ultrasound demonstrated occlusive thrombus involving the right subclavian and axillary veins (Figure 1) with extension to the innominate vein (Figure 2) and nonocclusive superficial venous thrombosis of the right cephalic vein. The results of complete blood count, coagulation, renal function, glucose, and electrolyte studies were unremarkable. A chest radiograph showed no evidence of bony abnormalities or masses at the apices of the lungs.
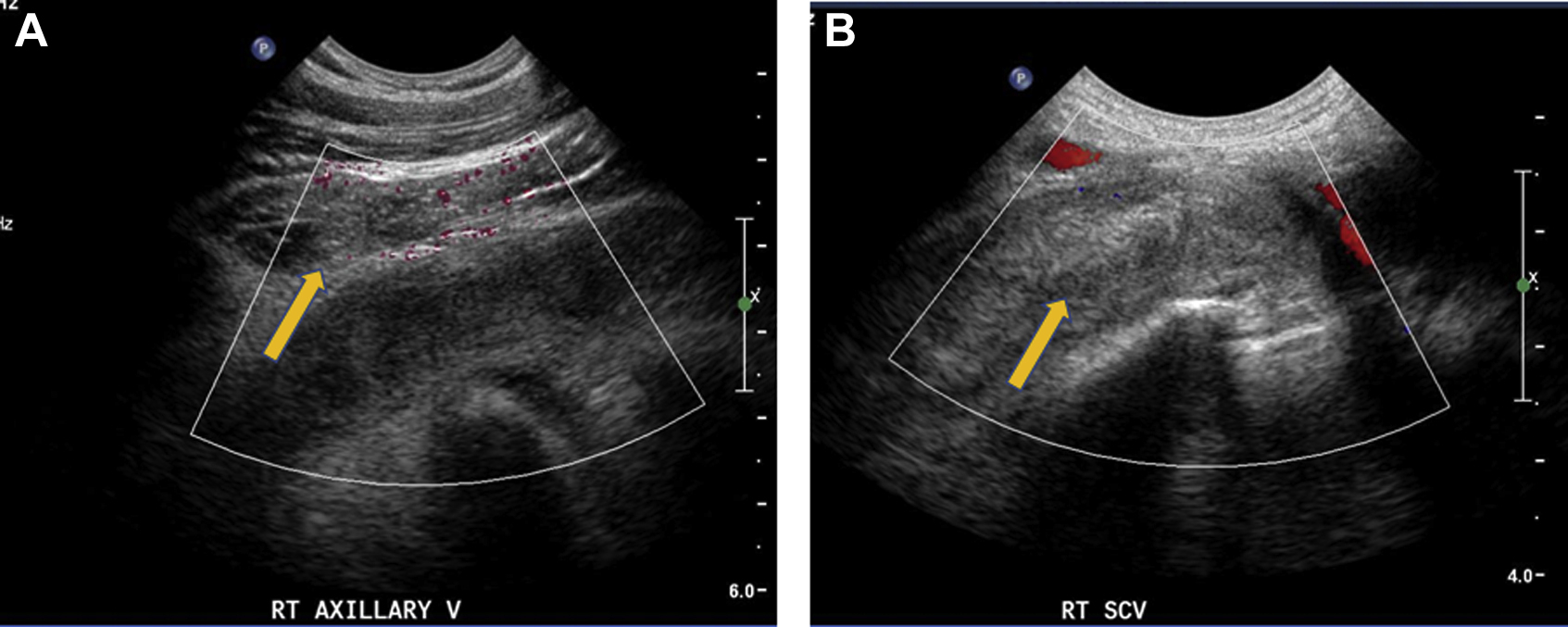
Power Doppler ultrasound images of the right axillary vein (A) and color Doppler of the right subclavian vein (B) demonstrate a heterogeneous filling defect consistent with thrombus (arrow).
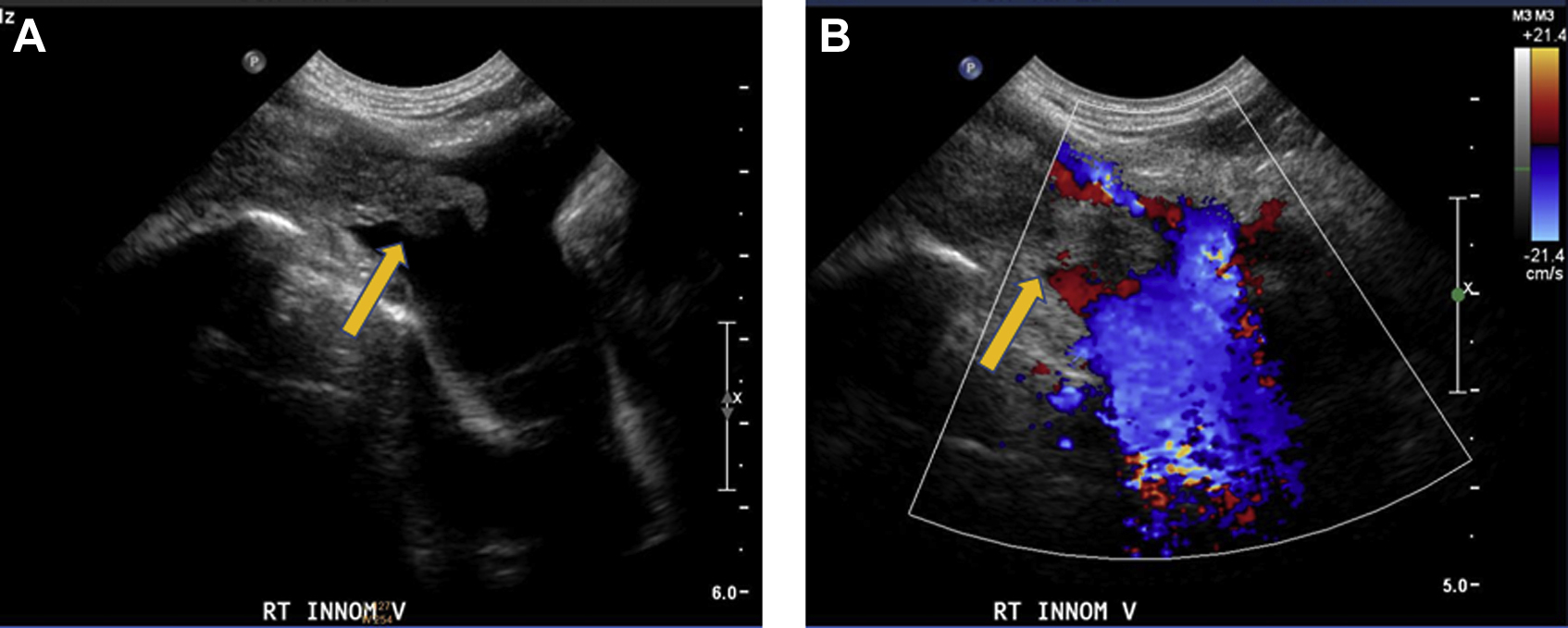
Ultrasound image of the right innominate vein demonstrates a heterogeneous filling defect consistent with thrombus (arrow). Ultrasound grayscale (A) and color Doppler (B).
Upon diagnosis of a thrombotic disorder, the patient was started on a continuous infusion of unfractionated heparin, and the vascular service was consulted. A venogram revealed an extensive thrombus burden throughout the first rib and clavicular zone (Figure 3). Catheter-directed suction thrombectomy with direct infusion of tissue plasmin activator was performed with extensive thrombus removal. Because a subsequent venogram revealed residual clot burden, balloon angioplasty was performed over a guidewire, and adequate post-procedural flow was achieved (Figures 4 and 5).

Fluoroscopic contrast image of the right axillary and subclavian veins demonstrates filling defects consistent with thrombus (arrows).
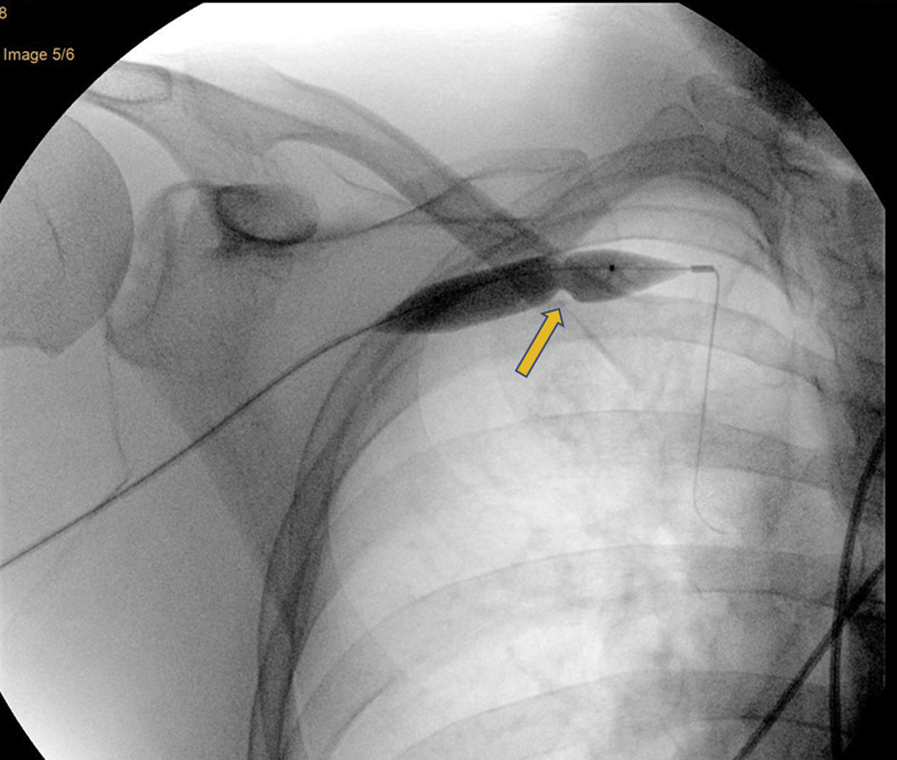
Fluoroscopic image of the right subclavian vein and balloon with “waist” indicating area of stenosis between first rib and clavicle (arrow).

Fluoroscopic image of right subclavian vein after thrombectomy demonstrating a decrease in thrombus and area of stenosis between first rib and clavicle (arrow).
The patient remained in the hospital for catheter-directed tissue plasmin activator and heparin infusion. He was discharged on the third day of his hospitalization, with a home regimen of 81 mg of aspirin daily and 15 mg of rivaroxaban twice daily. He returned 2 wk later for a scheduled elective resection of the first rib and anterior scalenectomy with venolysis (resection of fibrotic tissue surrounding the subclavian vein); an intraoperative ultrasound found no additional thrombus. Three weeks after surgery, an ultrasound examination of the right upper extremity demonstrated patency of the previously thrombosed veins (Figure 6). At that time, the patient experienced no edema or arm pain. He continued to take aspirin and rivaroxaban for 90 and 30 d, respectively, after his initial hospitalization and was given instructions to avoid trauma during the anticoagulation period.
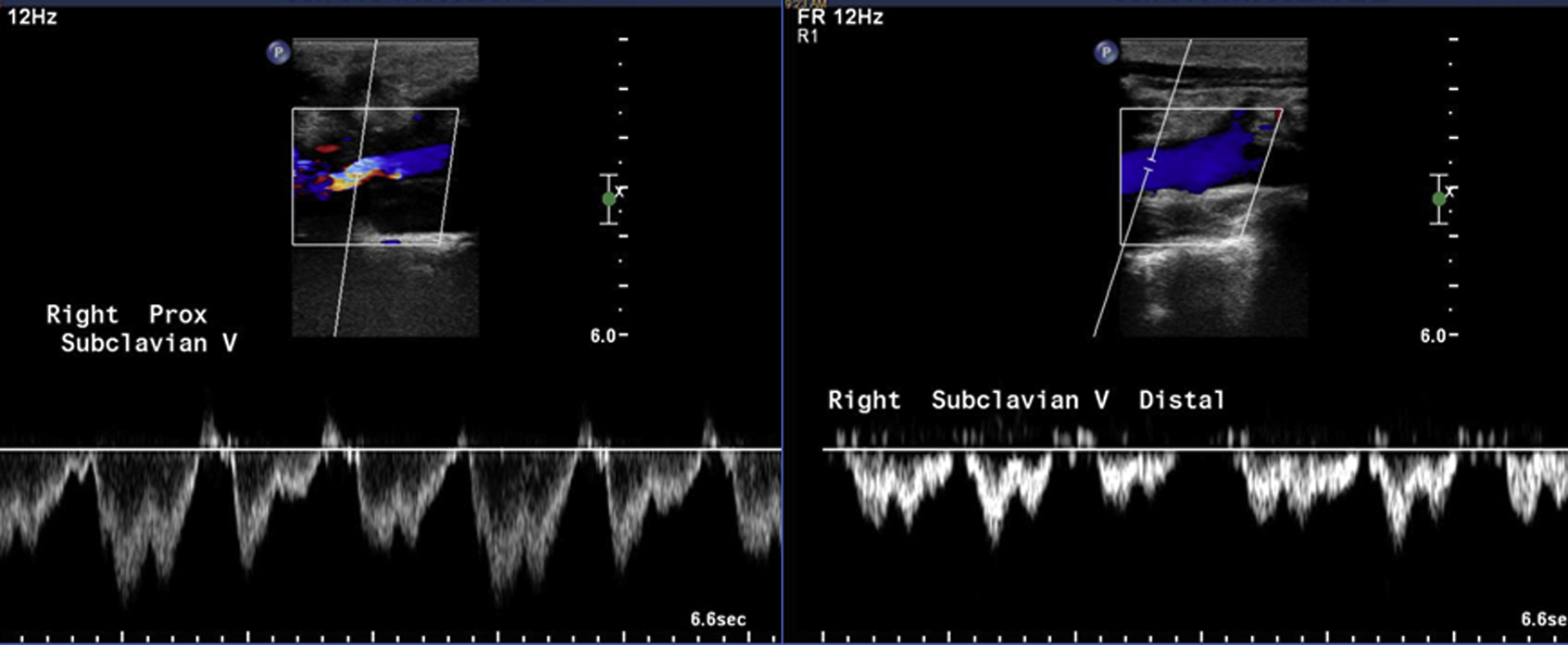
Duplex ultrasound of right subclavian vein after right first rib resection and scalenectomy with venolysis demonstrates venous patency.
Discussion
Because a majority of climbing-induced injuries are related to inflammatory conditions affecting the bursa, ligaments, or tendons,6,7 overuse syndromes were considered as potential differential diagnoses. However, the lack of point tenderness, the preserved range of motion, and the presence of generalized upper extremity edema made overuse syndromes unlikely. Acute injuries such as fractures or sprains were also improbable due to the absence of direct trauma or sudden pain with forced movements. Furthermore, the clinical and radiographic evaluation of the supraclavicular space did not show masses or clavicular or costal abnormalities.
Upper extremity exertional compartment syndrome, previously described in climbers, is a condition caused by elevated muscle compartment pressures and could also be included in the differential diagnosis. 8 In its acute form, exertional compartment syndrome can present with edema and painful contracture of the flexor muscles of the forearm or the interosseous muscles of the hands, with or without rhabdomyolysis. Early perceived muscle fatigue of the affected muscle groups can be indicative of chronic, recurrent elevation of pressure. Although measurement of forearm compartmental pressure was not performed, the lack of worsening pain during flexor muscle extension in our patient did not correlate with previously described cases.
Our patient was ultimately diagnosed with upper extremity deep vein thrombosis (UEDVT). UEDVT, a manifestation of thoracic outlet syndrome (TOS), occurs rarely in comparison to lower extremity thrombosis and has an annual reported incidence ranging from 2.0 to 3.6 per 100,000 in the general population.9,10 The signs and symptoms of TOS are provoked by the compression of the thoracic outlet structures as they exit the thoracic cavity. TOS can be neurogenic (95%), venous (4%), or arterial (1%). When the venous system is affected, as in our patient, compression of the thoracic outlet structures may be intermittent and positional, or it may lead to the formation of a local thrombus. 11
The majority of UEDVT presentations are promoted by secondary causes such as systemic or local predisposing factors (eg, central venous catheters, pacemakers, malignancy, thrombophilia). Primary thrombosis or Paget-Schroetter syndrome, on the other hand, lacks an evident cause. Although most thrombotic disorders develop in older patients with decreased mobility, Paget-Schroetter syndrome is generally diagnosed in young, athletic individuals after physical activity and is therefore commonly referred to as effort thrombosis.9,12
Cases of effort thrombosis have been described in a wide range of activities, from high-effort sports such as baseball and basketball to low-effort activities such as playing video games or the violin. 13 Although effort thrombosis in climbers has been reported, previously described cases were diagnosed in the subacute and chronic stages of the disease. 14 Our patient, however, was diagnosed less than 48 h after the onset of the syndrome’s initial symptoms and in the acute stage.
Many patients with effort thrombosis have a reduced costoclavicular space due to an abnormal lateral insertion of the costoclavicular ligament. Hypertrophy of the subclavius and anterior scalene muscle due to exercise can further reduce this space. In some patients, the presence of a cervical rib, a congenital anatomic variation, can also compress the structures in this anatomical region. 15 Repetitive compression of the vein can generate lesions of the intimal tunica, inflammation, and local fibrosis and thereby promote activation of the coagulation cascade and thrombus formation. Overhead movement of the upper extremities, a foundational component of climbing technique across disciplines, only exacerbates this phenomenon. 16
The classical clinical presentation of effort thrombosis includes unilateral tenderness over the upper extremity and a congested appearance of the chest, with edema, erythema, and cyanosis. Superficial veins can appear engorged, and thrombosed veins can be palpated in the axilla. Dilated veins and ecchymosis over the anterior shoulder and the entire arm, known as Urschel’s sign, may also be present.11,13 This syndrome may present with, or be complicated by, pulmonary embolism, although the incidence of clinically significant pulmonary embolism with UEDVT is lower than that observed with lower extremity DVT. 9 In addition to edema, clinical examination may reveal the absence of a radial pulse if there is concomitant compression of the arterial components of the thoracic outlet. 17
Confirmatory imaging modalities include ultrasound, computed tomography venography, magnetic resonance venography, and catheter-directed venography. Duplex ultrasonography is the initial modality of choice with a sensitivity of 80% and specificity of 100%. 18 Alternative diagnostic modalities should be used in patients with negative studies and high clinical suspicion.19,20
There is a lack of consensus regarding the optimal treatment for this condition, and significant differences exist in the management of patients diagnosed in the acute phase and patients diagnosed in the subacute phase. 14 Anticoagulation alone may be appropriate for patients who present more than 2 wk after the onset of initial symptoms (chronic UEDVT). It may also be appropriate for patients with very mild symptoms or limited clot burden. 21 On the other hand, patients diagnosed with UEDVT less than 2 wk after the onset of initial symptoms (acute UEDVT) and patients who have an extensive clot burden may benefit from endovascular treatment modalities. These modalities may prevent complications such as embolic events and post-thrombotic syndrome (PTS). PTS reportedly occurs in 27 to 44% of patients with UEDVT and is characterized by chronic pain, heaviness, and edema of the affected extremity with potential loss of function. A retrospective review of 30 patients revealed fewer incidences of PTS among patients treated with catheter-directed thrombolysis. 22 If used, thrombolytic therapy should be initiated as early as possible. Treatment is typically maintained for 24 to 72 h and can be accompanied by both anticoagulation (usually unfractionated heparin) and aspirin. 20
Catheters for percutaneous mechanical thrombectomy techniques that remove thrombus through aspiration, fragmentation, or maceration have recently become available. Stents placed at the subclavian vein have a high reocclusion rate.23,24
Although a complete review of the indications and surgical techniques used to relieve the compression of the thoracic outlet structures is outside the scope of this article, multiple approaches exist.15,25,26,27 A combination of thrombolysis and prompt resection of the first rib seemed to result in the best functional outcomes over a large cohort of patients treated with these combined modalities. Continuation of anticoagulation after resection of the first rib or vein resection does not seem to provide additional benefits. 15
Conclusions
Upper extremity injuries are common among the growing population of climbers. Inflammatory processes or overuse syndromes of the musculoskeletal structures comprise a majority of these injuries; however, as evidenced by the case described, the movement of climbing can exacerbate disorders affecting the vascular structures of the upper thoracic region as well.
To our knowledge, this is the first reported climber diagnosed in the acute phase of UEDVT and treated with thrombectomy and catheter-directed thrombolysis followed by surgical resection of the first rib. Although there is a lack of high-quality studies that demonstrate the benefits of this approach, early diagnosis and aggressive treatment may reduce the rate of post-thrombotic syndrome and provide satisfactory functional outcomes. Because of the importance of early diagnosis and initiation of treatment, it is critical to consider disorders affecting the upper thoracic vascular structures, such as effort thrombosis, in a differential diagnosis for upper extremity injuries among the population of climbers.
Footnotes
Acknowledgements
Acknowledgments: The authors thank Ilaria Ferrari for extensive editing.
Author Contributions: Drafting of the manuscript (MM, AM); critical revision of the manuscript, references and abstract (AB, CD, PR); interpretation of images (PR); approval of final manuscript (MM, AM, AB, PJR, CD).
Financial/Material Support: None.
Disclosures: None.