
Abstract
We report a case of a 42-y-old female patient who sustained a sting to the neck from a Trachinus draco fish. She subsequently developed complications including arytenoid membrane edema secondary to either the local anesthetic agent administered to the wound or the dracotoxin itself. The patient was examined in the emergency department after the sting. Local anesthesia with lidocaine was administered to the areas of injury at another hospital before presenting to our hospital emergency department. The patient reported that her pain partially decreased but hoarseness developed and she had difficulty breathing after the local anesthetic was administered. Laryngeal examination by our hospital's otolaryngologist revealed edema of the patient's right arytenoid membrane without evidence of vocal cord swelling. Computed tomography of the neck revealed edema in the right arytenoid membrane on the side of the neck where the local anesthetic had been injected. The patient, who was given supplementary treatment, was discharged without any complications on the seventh day of hospitalization. The principle treatment for these types of stings includes immersion in hot water, analgesic therapy, and observation for signs of local and systemic envenomation. We recommend using caution when injecting local anesthetic agents in the neck because of underlying vital structures.
Introduction
In recent years, recreational diving and other water-related activities have gained popularity, resulting in an increased number of traumatic bites and toxic stings. Contact with aquatic creatures that envenomate using their spines can cause local and systemic toxicity. 1 According to data from the American Association of Poison Control Centers, in 2017, 572 fish sting-related poisoning cases were reported. Serious systemic findings were observed in only 3 of the reported cases with no recorded deaths. 2
In this case report, we present guidelines for treating stings from the Trachinus draco fish and discuss potential complications of using local anesthetic agents when treating these wounds.
Case
A 42-y-old female presented to the emergency department with severe pain and redness in the legs, left hand, and front of the neck due to being stung by a T draco 4 h before admission to the hospital. It was learned that local anesthesia with lidocaine had been administered to the wounds at the outside state hospital before the patient presented to our tertiary care hospital emergency department. She was administered 3 mL (60 mg) to the neck, 4 mL (80 mg) to the left hand, and 5 mL (100 mg) to the lower extremity for a total of 240 mg 2% lidocaine for local anesthesia. After lidocaine administration, her pain was self-described as a 60% reduction before she was discharged from the state hospital, although she reported shortness of breath and hoarseness.
When she presented to our hospital’s emergency department, vital signs were as follows: blood pressure of 130/70 mm Hg, pulse of 98 beats·min-1, O2 saturation of 99%, respiration rate of 22 breaths·min-1, and Glasgow Coma Score of 15 (G4M6S5). Sinus tachycardia was recorded on the electrocardiogram. No abnormality was found on the patient's cardiopulmonary or neurological examination. There were painful ecchymosis and hyperemic lesions on the front of the neck close to the midline, on the proximal phalanx of the flexor face of the left second finger, on the middle third of the medial side of the right thigh, and the upper third of the medial side of the left leg (Figure 1). The peripheral pulses were palpable and symmetrical. There was no limitation of movement in the extremities. There was no uvula edema on the oropharynx examination. Edema was visualized on the right arytenoid membrane, but there was no edema or swelling surrounding the vocal cords as per the laryngeal examination performed by our otorhinolaryngologist. Computed tomography of the neck revealed edema in the right arytenoid membrane on the side of the neck where the local anesthetic had been injected (Figure 2).

Lesions on the neck, leg, and arm stung by the T draco.
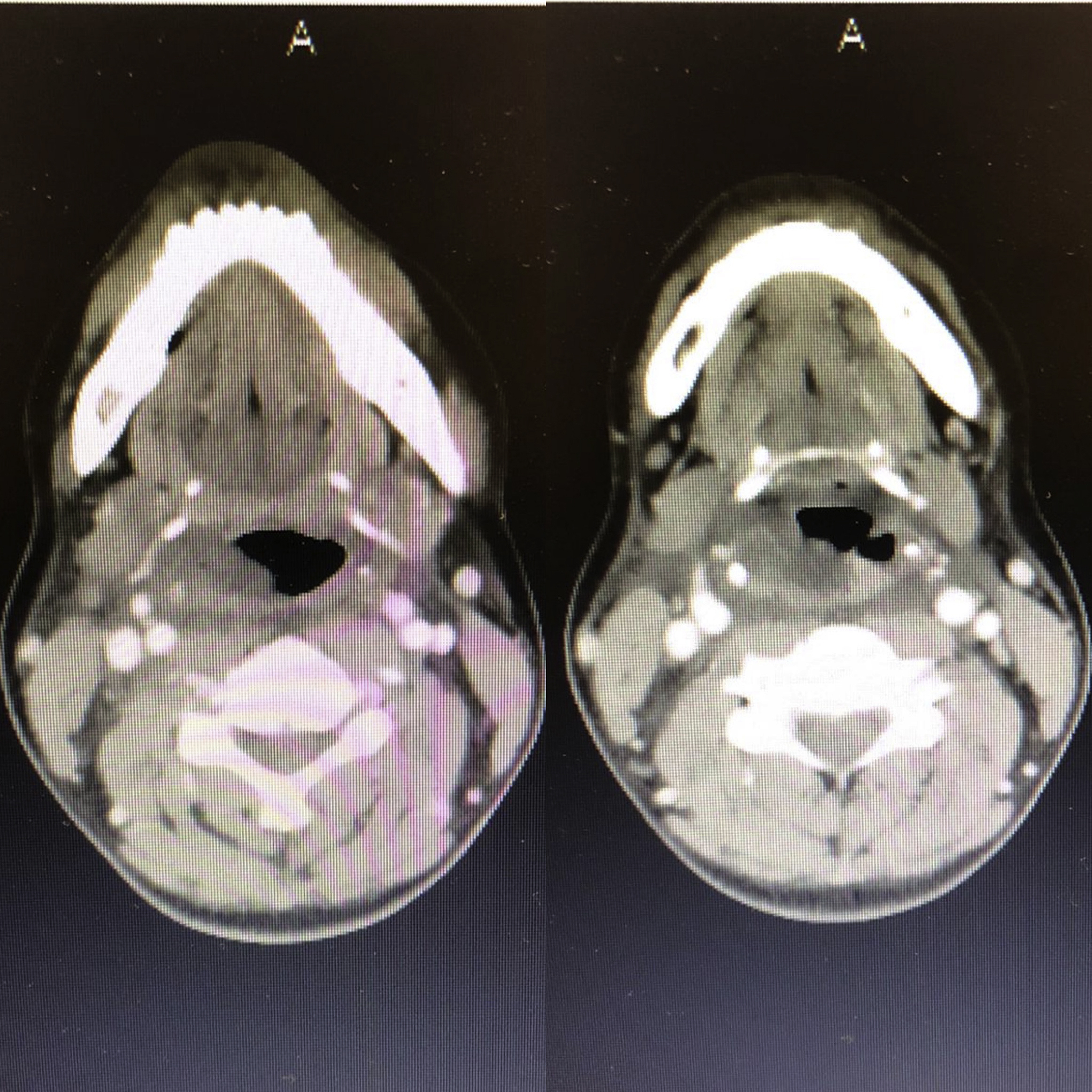
Computed tomography of the neck demonstrating edema in the right arytenoid membrane on the side where the local anesthetic injection was made.
The patient underwent urgent wound care. Spines that could be visualized were removed under sterile technique. The extremities were immersed in hot water at a temperature that the patient was able to tolerate, and a hot compress was applied on the neck. The patient was administered 1 mg·kg-1 diphenhydramine, 0.5 mg·kg-1 ranitidine, and 1 mg·kg-1 methylprednisolone. Doses of 1000 mg paracetamol and 20 mg tenoksikam were administered by intravenous infusion for analgesia. Tetanus toxoid prophylaxis was administered.
The patient was hospitalized. The laboratory values when the patient presented to the emergency department and the follow-up values are summarized in Table 1. Hematocrit values decreased and amylase and creatine kinase values increased on subsequent blood draws. Hemoglobin values were 13.4 g·dL-1 at the time of admission and decreased to 10 g·dL-1 on the second day of hospitalization. The patient did not require a blood transfusion. The amylase value was 132 IU·L-1 at the time of admission and increased to 629 IU·L-1 on the first day of hospitalization. The lipase value was 15 IU·L-1 at the time of admission, and there was no increase in serial serum lipase levels.
Blood test findings
ALT, alanine transferase; AST, aspartate transferase; CK-MB, creatinine kinase-myocardial band; WBC, white blood cells.
Value other than reference values.
The patient did not have abdominal pain, and no acute pathology was detected on abdominal ultrasonography. The patient's hyperamylasemia was considered to be toxin related and not attributed to acute pancreatitis. Salivary gland or duct obstruction secondary to the local anesthetic injection was also considered as a possible etiology. The creatine kinase value was 2379 IU·L-1 at the time of admission and increased to 5475 IU·L-1 on the first day of hospitalization. Fluid deficits were corrected, and hourly urine output was monitored. Fluid replacement was performed with 1 to 2 mL·kg-1·min-1 urine output per hour. The patient, who was given supplementary treatment, was discharged without complications on the seventh day of hospitalization.
Discussion
Trachinus fish are found in the bottom and coastal regions of the Mediterranean and eastern Atlantic. They live at a depth ranging from a few meters up to 150 m (in winter) in sandy, muddy, or pebbly bottom regions. 3 The most well-known member of the Trachinidae family, which also causes most of the fish stings in Turkey, is the Echichthys vipera (its previous name being Trachinus vipera/Trachinus draco) or the stinging fish.4,5 It has an average length of 14 cm and carries a venom called dracotoxin in a spine on the operculum. There are 5 to 8 dorsal spines that beam out of the first dorsal fin, and tissue extends along the sheaths covering the spines 3 (Figure 3).

Five to 8 dorsal spine beams on the first dorsal fin of T draco, Dracotoxin is in the spine on the operculum.
Dracotoxin contains a number of high-molecular-weight proteins that are unresistant to heat, such as 5-hydroxytryptamine which causes characteristic pain, histamine which causes redness and itching, epinephrine which causes cardiovascular effects, norepinephrine, seratonin, and quinine which induces vasodilation. As with other natural poisons, dracotoxin contains mucopolysaccharide and albumin.3,4,6 It is known to cause membrane depolarization, hemolysis, rhabdomyolysis, an increase in vascular permeability, and pain. 5
In our case, hematocrit values decreased, and creatine kinase values and amylase values increased. We believe that the decrease in hematocrit values was caused by membrane depolarization and the hemolyzing effect of dracotoxin. The hemolysis was self-limited and did not require transfusion. Myonecrosis developed as a result of stings on the affected extremities and caused creatine kinase levels to increase. For rhabdomyolysis, fluid replacement was performed, urine output was monitored hourly, and renal function tests were conducted. Our patient responded to the treatment, and there were no complications such as cellulitis of the extremities or compartment syndrome. Because P-isoamylase and S-isoamylase tests could not be performed in our laboratory, it was not possible to determine the subtype of the hyperamylasemia. Lipase values remained within normal limits. There was no abdominal pain during the follow-up, and there were no abnormal pancreatic findings on abdominal ultrasonography. Therefore, no pancreatitis was considered. We postulate that the hyperamylasemia was dracotoxin induced or from salivary gland or duct obstruction.
Human poisoning by fish also occurs in fishermen who walk on sandy shores, swim, and collect fish from nets. Pain with a sudden onset and severe burning occurs, and a searing pain spreads toward the affected extremity. When left untreated, the pain decreases within 2 to 24 h.3,6 Rarely, nausea, vomiting, seizures, shortness of breath, hypotension, cardiac arrhythmia, systemic allergic reaction, anaphylactic respiratory depression, and death occur. However, such reactions are usually attributable to the stings of the greater T draco, which lives in deeper offshore waters, rather than those of the lesser weever fish. 7 Our patient was stung on various parts of her body while swimming in the shallow sandy sea.
The treatment required in cases of stinging by Trachinus fish is cleaning the wound and immersing the affected part of the body in water as hot as the patient can tolerate (40–45°C; 104–113°F) for at least 30 min. Because the toxin is thermolabile, it will denature in hot water immersion, and pain will be significantly reduced within a few minutes. In addition, hot water will help to reduce pain by modulating the pain receptors in the nervous system.4,8 Cold application, however, worsens pain. Calcium injection and washing the bitten area using soapy water or potassium permanganated water are treatment methods that have not been shown to be clinically efficacious. Tetanus prophylaxis is recommended for nonimmune patients. Infection is rare and prophylactic antibiotics are not recommended. However, if local infection develops, antibiotics will be necessary or may be considered for prophylaxis in patients whose immune systems have been suppressed.3,6 Common organisms associated with marine trauma include Mycobacterium marinum, Vibrio vulnificus, and Staphylococcus and Streptococcus spp. Therefore, in outpatient management ciprofloxacin, trimethoprim-sulfamethoxazole, and doxycycline can be used; in inpatient management, second-generation cephalosporin (cefuroxime), third-generation cephalosporin (cefoperazone, ceftazidime, ceftizoxime, ceftriaxone), ciprofloxacin, gentamicin, and trimethoprim-sulfamethoxazole can be used. 1
Antihistamines and steroids may alleviate the local inflammatory response. Simple analgesics are usually sufficient to control residual pain after application of hot water, but opioid analgesia may at times be required. For severe and uncontrolled pain, the injection of local anesthetics with infiltration, through regional nerve block, or through continuous epidural nerve block with bupivacaine may be considered.3,6 In our case, 3 mL of 2% lidocaine (60 mg) was administered to the right side of the midline of the neck. The patient reported that her pain regressed by 60% after local anesthetic. As in our case, however, the possible side effects of local anesthetic injection should be used with consideration in regions where subcutaneous fat and muscle tissue are diminished, such as regions of the neck. In our case, the absence of systemic allergic reaction after administration of local anesthesia and the absence of uvula edema or vocal cord edema suggest that unilateral edema in the arytenoid membrane was caused by the local accumulative effect of the local anesthetic agent.
Conclusions
Local or systemic envenomations may occur as a result of contact with the spines of the Trachinus fish during the summer season. The main principle of treatment is immersion in hot water, analgesic therapy, and supportive care with observation for signs of local and systemic toxicity. When treating these types of penetrating wounds, local anesthetic agents that are administered within the neck region should be used cautiously to avoid adverse side effects or complications.
Footnotes
Acknowledgements
Author Contributions: Study concept and design (MG, SS); acquisition of data (MG, SS); analysis of the data (MG, SS); drafting the manuscript (MG, SS); critical revision of manuscript (MG); approval of final manuscript (MG, SS).
Financial/Material Support: None.
Disclosures: None.