
Abstract
The case of a 42-y-old rock climber who sustained a complete, isolated rupture of the short head of the biceps brachii muscle after falling onto his upper arm while bouldering is presented. This is the first description of this rare injury after a climbing accident. Moreover, there is no definitive consensus on whether and when surgical intervention is necessary in such a case. We performed a direct end-to-end suture of the muscle belly through an open surgical approach. Postoperatively, we performed a detailed follow-up, including clinical examinations and sonography and magnetic resonance imaging to check the integrity of the suture. After 6 mo, our patient had regained a full range of motion without functional complaints or pain. Concerning the sports-specific outcome, we only found a slight decrease in rock-climbing abilities (Union Internationale des Associations d’Alpinisme Scale of Difficulty grade VII+ postsurgery compared to VIII preinjury). In conclusion, we suggest that early surgical reapproximation of the muscle belly might be the best treatment option for this severe but rare injury in athletes.
Introduction
Injuries of the upper extremity, especially the fingers and shoulders, are the most common injuries in rock climbers.1,2 The number of these injuries has been increasing recently, not least as a result of the quickly increasing number of indoor bouldering gyms and concomitant increasing popularity of sport climbing and bouldering. Consequently, the understanding of most of these pathologies and the treatment algorithms has improved over the last couple of years. The following report presents the first documented case of a complete rupture of the short head of the biceps muscle belly due to a rock-climbing accident, including a thorough follow-up until return to sports.
Case Report
A 42-y-old, otherwise healthy (nonsmoker, no medications used, no preexisting conditions, body mass index 23.0 kg·m-2) male rock climber fell while climbing in a bouldering gym. His preinjury rock climbing ability on the Union Internationale des Associations d’Alpinisme Scale of Difficulty 3 –5 was grade VIII redpoint (to climb a route in redpoint style means to climb it using only one’s strength and using only the rock structures themselves—without any additional technical aids and without putting weight on any of the belay points). He was climbing around a volume (wooden or fiberglass modular structures—mostly prism shaped—protruding from a rock-climbing wall that are used as foot- or handholds) when his foot slipped. Consequently, his right upper arm hit the edge of the volume while the biceps muscle was fully tensed, a blunt trauma that resulted in a rupture of the short head biceps muscle belly. This led to immediate pain, swelling, and a palpable gap in the mid-portion of the upper right arm (Figure 1A).
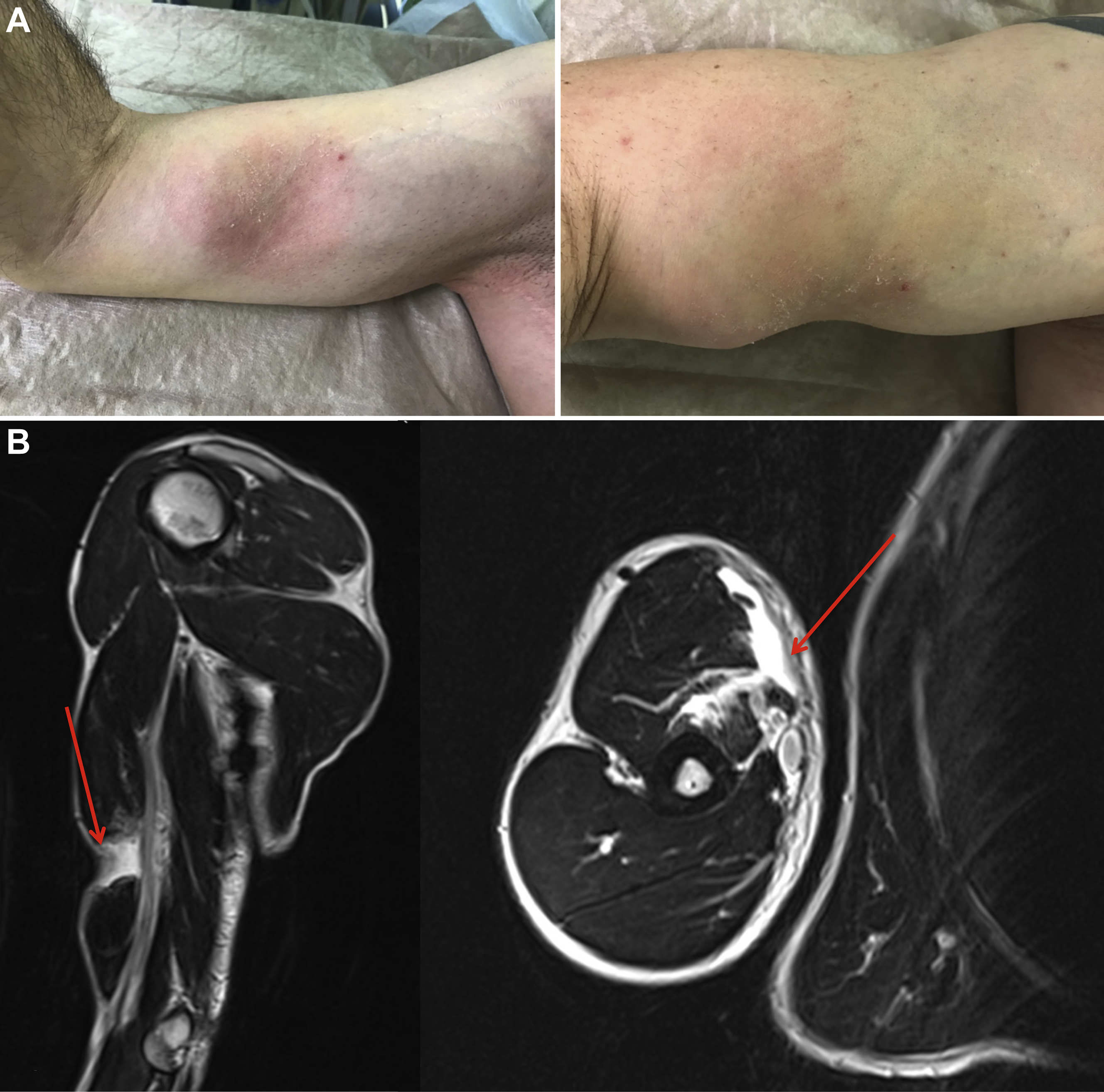
A, The patient’s right upper arm with the vast gap resulting in the rupture of the biceps short head muscle belly. B, Magnetic resonance imaging of the patient’s injured upper arm. The arrows highlight the complete, isolated rupture of the muscle belly of the short head of the biceps brachii.
Seven days after the injury, he presented to our department after having consulted 2 orthopedic surgeons who had recommended a magnetic resonance imaging (MRI) scan but, owing to their lack of experience with this type of rare injury, were not sure about the best treatment after having obtained the images. The existing x-ray and MRI showed a complete, isolated rupture of the short head of the biceps brachii muscle but no fracture (Figure 1B). The clinical examination showed a depression in the medial, mid-portion of the upper right arm with hematoma and tenderness and without an open wound. Furthermore, there was decreased strength, especially for supination and flexion in the elbow joint (Medical Research Council Manual Muscle Testing scale 6 : III/V).
Consequently, we briefed the patient about the treatment options and the potential risks associated with them. Although our patient was left-handed and the injury was in his nondominant arm, we recommended surgical therapy to reduce deformity and to enable our patient to regain full strength and functionality in both arms. This is necessary for rock climbing and for most activities of daily life.
We performed an operation with an open surgical approach 10 d after the trauma to prevent the ruptured muscle belly from further retraction, which would hinder anatomical reduction. In line with the recent literature, we restored anatomical integrity of the muscle belly itself through direct end-to-end modified Mason-Allen stitches (2.0 Vicryl). Additionally, we placed adapting sutures of the epimysium 7 (PDS 3.0; Polydioxanone Suture) (Figure 2A).7,8
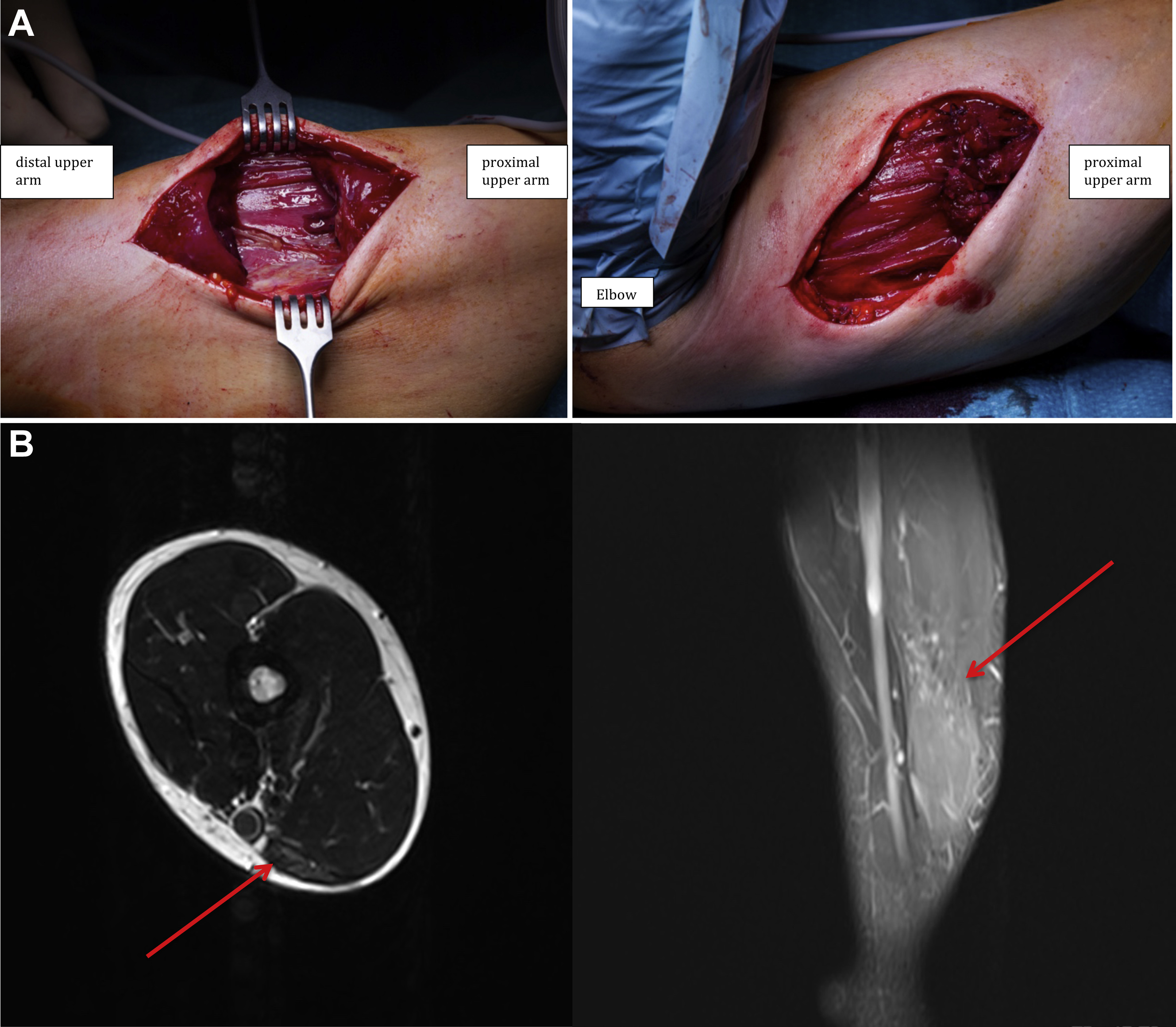
A, The intraoperative situs before (left) and after surgical reconstruction (right) of the of the muscle belly of the short head of the biceps brachii. B, Magnetic resonance imaging of the patient’s right upper arm 24 wk after surgery. The muscle belly of the short head of the biceps brachii is continuous. The arrows highlight the area of the former rupture where, in comparison with the surroundings, a higher percentage of fibrous scar tissue can be seen.
Postoperatively, the patient’s upper arm was immobilized in a Gilchrist sling (shoulder and arm immobilizer) for 6 wk. Passive physiotherapy with gradual progression was allowed 3 wk after surgery. After 8 wk, our patient was able to begin an intensified rehabilitation program for muscle growth and mobilization of the adjoining joints. Twelve weeks after surgery, there was an absence of pain with rest and weight bearing. Furthermore, ultrasound showed the integrity of the muscle belly repair at this point.
Thus, the patient was allowed to resume sports-specific exercises. Twenty-four weeks postoperatively, we performed an MRI, which showed successful anatomical reconstruction of the medial biceps muscle belly. In the area of the former rupture, a high percentage of fibrous scar tissue was found. This was expected, considering the stage of the healing process at this point in time after surgery (Figure 2B). At this time, the clinical investigation showed a full range of motion without functional complaints or pain.
Concerning the sports-specific outcome, 2.5 y after surgery we found only a slight decrease in rock-climbing ability (Union Internationale des Associations d’Alpinisme grade [red point]: preinjury VIII, 30 mo postsurgery VII+). Moreover, we determined a Single Assessment Numerical Evaluation Score 9 for activities of daily life and rock climbing. To evaluate this score, the patient rates the current status of the injured body part on a scale of 0 to 100 (0=complete disability; 100=no complaints at all). For activities of both daily life and rock climbing, a score of 100 was achieved.
Discussion
To date, only a very limited number of cases of this kind of injury have been reported, mainly related to accidents of military paratroopers using static lines, waterskiing, and traffic accidents. 10 –14 What all injuries reported in the literature have in common is that a sudden direct blunt force on the body of the tensed biceps muscle belly led to a complete transection of the muscle tissue. All patients were male with an age between 15 and 26 y. 14 Our patient is by far the oldest person (42 y) reported with this kind of injury. Although the reported injury mechanism is possible in other scenarios, the increasing popularity of sport climbing and especially indoor bouldering, where volumes are increasingly used, is likely to make this injury more frequent in the future.
Whether there are any predisposing factors for such an injury is difficult to determine. All patients seem to have been otherwise healthy, physically active individuals at the time of the injury. In our case, the tensed biceps brachii muscle belly might have been more vulnerable to the impact owing to a minimal amount of subcutaneous fat. Unfortunately, to the best of our knowledge, there are no studies yet hinting at a relationship between the amount of subcutaneous fat and the severity of muscle tears after trauma. This might be an interesting avenue for further research.
In general, the majority of muscle injuries can be managed conservatively with measures such as rest, nonsteroidal anti-inflammatory drugs, and physiotherapy. There are only a few indications for surgery: a large intramuscular hematoma, tears of more than half of the muscle belly (grade 3b-4), and the occurrence of a compartment syndrome, which is an absolute emergency.15,16 In these cases, however, surgery seems to be the therapy of choice; the existing studies, although limited in number, show a significant advantage concerning function, appearance, and patient satisfaction compared to conservative treatment.8,17–19 For example, a study comparing the outcome of paratroopers with a traumatic closed transection of the biceps muscle belly after surgical repair (n=9) and conservative treatment (n=3) showed significant improvement in terms of function, appearance, and patient satisfaction after the surgical repair. 17 For tendinous injuries of the biceps and triceps muscle, on which more studies have been performed over the last few years, the results after surgery are superior to conservative treatment and thus indicate surgical therapy as the treatment of choice for athletes. 20 Furthermore, in cases of persisting extension pain (duration >4-6 mo) in a previously injured muscle, which sometimes also includes an extension deficit, the formation of scar adhesions restricting the movement of the muscle might be the cause of pain. In these cases, surgery might be a viable treatment option that needs to be discussed with the patient. 19 Nonetheless, there is no definitive consensus on when and whether surgical intervention is necessary in such cases. 19
The biceps brachii muscle is the strongest supinator of the elbow joint and an accessory flexor of both the glenohumeral and the elbow joints. 21 Furthermore, a recent biomechanical study showed that it might enhance the dynamic stability of the shoulder joint in the initial 30° of elevation through its long head. 22 Because pathologies of the long head of the biceps brachii (eg, biceps tendinitis, instability, and tendon rupture) have a high incidence, much research has been performed over the last few years, leading to a better understanding of the pathologies and treatment options. 23 Studies have reported that proximal tendon ruptures could cause a loss of as much as 29% of flexion and supination strength without surgical treatment. Thus, surgery (biceps tenodesis) is only recommended for very active patients who cannot tolerate the relatively small amount of strength loss, given their activities or occupations. 23 This leads to the conclusion that most of the function and power of the biceps brachii muscle is provided through the short head. Hence, appropriate therapy is very important to prevent a severe loss of strength and function. Thus, to reduce deformity and enable our patient to regain full strength and functionality, we made the decision to perform surgery to restore anatomical integrity.
Muscle fibers are difficult to handle during surgery because the tissue quality is soft; thus, sutures are more likely to tear out in comparison to use in injuries of the tendon and the myotendinous junction. 19 Therefore, we used a combination of core stitches (Mason-Allen) and adaptation of sutures of the epimysium: Biomechanical studies show significantly improved biomechanical properties of such a combination in comparison to core stitches alone.7,8
The strength of the suture might be of great importance; a stronger repair might allow earlier return to function and strengthening, leading to decreased scar formation and better functional outcome. As a future prospect, the use of barbed sutures seems to be very promising. Recent findings of a biomechanical in vitro study showed an even stronger repair through the use of barbed sutures in comparison with nonbarbed sutures. 24
Furthermore, the timing of the operative treatment might be an important aspect. If surgery is delayed, softening of the epimysium and muscle fibers could compromise the strength of the repair. 17
In light of our patient’s robust recovery and ability to return to rock climbing at a level near his preinjury level, our report is in line with the current literature, which has demonstrated excellent functional results after surgical repair of similar injuries of the biceps brachii muscle belly. 17 Thus, early surgical reapproximation of the muscle belly for this kind of injury might be the best treatment option for athletes. However, because the best method of muscle belly repair remains controversial, more studies, including long-term follow-up, are needed to strengthen this promising hypothesis.
Footnotes
Acknowledgements
Author Contributions: Study concept and design (MS, CL, VS); acquisition of data (MS, VS); drafting the manuscript (MS, CL); critical revision of the manuscript (CL, VS); final approval of the manuscript (MS, CL, VS).
Financial/Material Support: None. Disclosures: None.