
Abstract
Objective
To determine the epidemiology of injuries from hunting stands presenting to US emergency departments (EDs).
Methods
The National Electronic Injury Surveillance System (NEISS) database was queried for ED visits for the period 2008 through 2013 for hunting stand injuries and analyzed for age, diagnosis, sex, race, anatomic location of the injury, the use of alcohol, and association with a gunshot wound.
Results
There were an estimated 38,308 visits with an average age of 40.0 years (range, 1–83 years). The patients were predominantly male (93.3%), white (99.1%), and seen at small- or medium-size hospitals (80.6%). Disposition from the ED was admission in 20.1% and released in 79.9%. A fall occurred in 80.3%, a gunshot wound in 0.4%, and alcohol was involved in 0.6%. The most common diagnoses were a fracture (34.7%), contusion or abrasion (24.0%), strain or sprain (16.8%), laceration (7.7%), and internal organ injury (5.4%). Those injured in a fall were more frequently admitted (23.0% vs. 8.7%) and more likely to have a fracture (37.9% vs. 9.1%). Those with a fracture were older (44.6% vs. 37.9%). Those with internal organ injuries were more frequently admitted (44.8% vs 18.6%).
Conclusions
This study has characterized the epidemiology of hunting stand injuries with most occurring from falls. A fracture was the most common injury with a very low alcohol intoxication rate. These baseline data can now be used to compare other studies of hunting stand injuries and guide prevention strategies, such as education regarding the need for safety measures to prevent falls.
Introduction
Recreational hunting is a popular sport in the United States. The US Fish and Wildlife Service estimated that approximately 13 million people annually participated in hunting activities between 1991 and 2011. 1 Hunting stand injuries (Figure 1) have a higher associated mortality than gunshot injuries for hunters.2,3 There have been several small studies evaluating the injuries associated with such stands, 2 –9 and one has investigated the overall pattern of injuries across a national database to include all patients. 10 The purpose of this study was to expand the pattern of injuries from hunting stands using a national database, and specifically focus on fracture location as well as if the patient fell from the stand, sustained a fracture or gun shot wound, and/or was alcohol involved. This will provide a comprehensive perspective of this issue and the associated injuries. These data can then be used to propose future prevention programs for patients and education of first responders (eg, emergency medical technicians), and to guide medical kit development and future studies.

A hunter sitting in a hunting stand during the winter. A fall from such a height can result in serious injury. (Figure courtesy of the Indiana Department of Natural Resources.)
Methods
The data for this study were obtained from the National Electronic Injury Surveillance System (NEISS). The NEISS collects data from a probability sample of hospitals in the United States and its territories that have at least 6 beds and an emergency department (ED). The sample contains 5 strata, 4 based on size (the total number of ED visits reported by the hospital: small [0–16,830], medium [16,831–21,850], large [28,151–41,130], and very large [>41,130]) and 1 stratum consisting of children’s hospitals of all sizes. Currently there are 100 hospitals in the NEISS. Each hospital has an associated weight based on its ED size and geographic location. To produce national estimates of injuries, the statistical weights must be used rather than raw case counts. Estimates across the entire data set (in this instance the United States and its territories) are thus calculated using appropriate statistical software that accounts for the stratified, weighted data. This database is in the public domain and can be found at
The detailed data for ED visits for the 6-year period from January 2008 through December 2013 owing to hunting stands (NEISS product code 1895) was downloaded from the NEISS website and analyzed for age, diagnosis, sex, race, anatomic location of the injury, and the use of alcohol. Race was classified as White, Black, Amerindian (Hispanic and Native American), and Indo-Malay (Asian origins). 11 The years 2008 through 2013 were chosen to amplify the data from the previous published study which stopped at 2007. 10 This study received an exemption from the local institutional review board.
The narrative features for each case were analyzed to determine whether the patient fell from the stand or sustained a gunshot wound, or whether alcohol was involved. The terms used for gunshot wound were shot, gunshot, and GSW. The terms used for a fall were fall, fell, and fallen. The terms used to search for alcohol were alcohol, EtOH, intoxicated, drinking, drank, drunk, club, ethanol, saloon, tavern, liquor, booze, beer, whiskey, brandy, rum, vodka, scotch, tequila, wine, sake, champagne, and cognac.
Statistical Analyses
Statistical analyses were performed with SUDAAN 10 software (RTI International, Research Triangle Park, NC, 2008), which accounts for the weighted and stratified nature of the data. Continuous data are reported as the mean, and discrete data, as frequencies. Analyses between groups of continuous data (age) were performed with the Student’s t test (2 groups) or analysis of variance (3 or more groups). Differences between groups of discrete data (sex, race, ED disposition, stratum, diagnosis, month, weekday, and yes or no for internal organ injury, fall from stand, gunshot wound, alcohol involvement, and fracture) were analyzed by the χ2 test. A probability value of less than .05 was considered statistically significant. As this was an exploratory descriptive study, there were no preconceived outcomes. However, I did analyze for any differences between those who had or had not fallen from the stand, sustained a gunshot wound, sustained a fracture, or sustained an internal organ injury.
Results
During the 6-year period there were an estimated 38,308 ED visits (95% CI [35,595, 40,925]) owing to hunting stand injuries (Table 1). This gives an annual average of 6385 patients sustaining injuries from hunting stands. The average age of the patients was 40 years (Figure 2). The demographics are shown in Table 1; most patients were white men. The distribution of injuries is shown in Table 1 and Figure 3. One fifth of the patients were admitted, and approximately 80% fell from the stand. Alcohol use and sustaining a gunshot wound were very rare. The most common diagnosis was a fracture. Detailed analyses of the internal organ injuries revealed that 2126 (83.2%) involved the brain or head (from a simple concussion to intracranial bleed, excluding skull fractures), 301 (11.8%) the chest (eg pneumothorax, mediastinal hemorrhage), and 177 (5.0%) the abdomen (eg, liver or spleen laceration). Detailed analyses of the disposition are shown in Table 2. With increasing hospital size there were fewer patients transferred to another hospital, but more were directly admitted.
Demographics of patients sustaining injuries from hunting stands
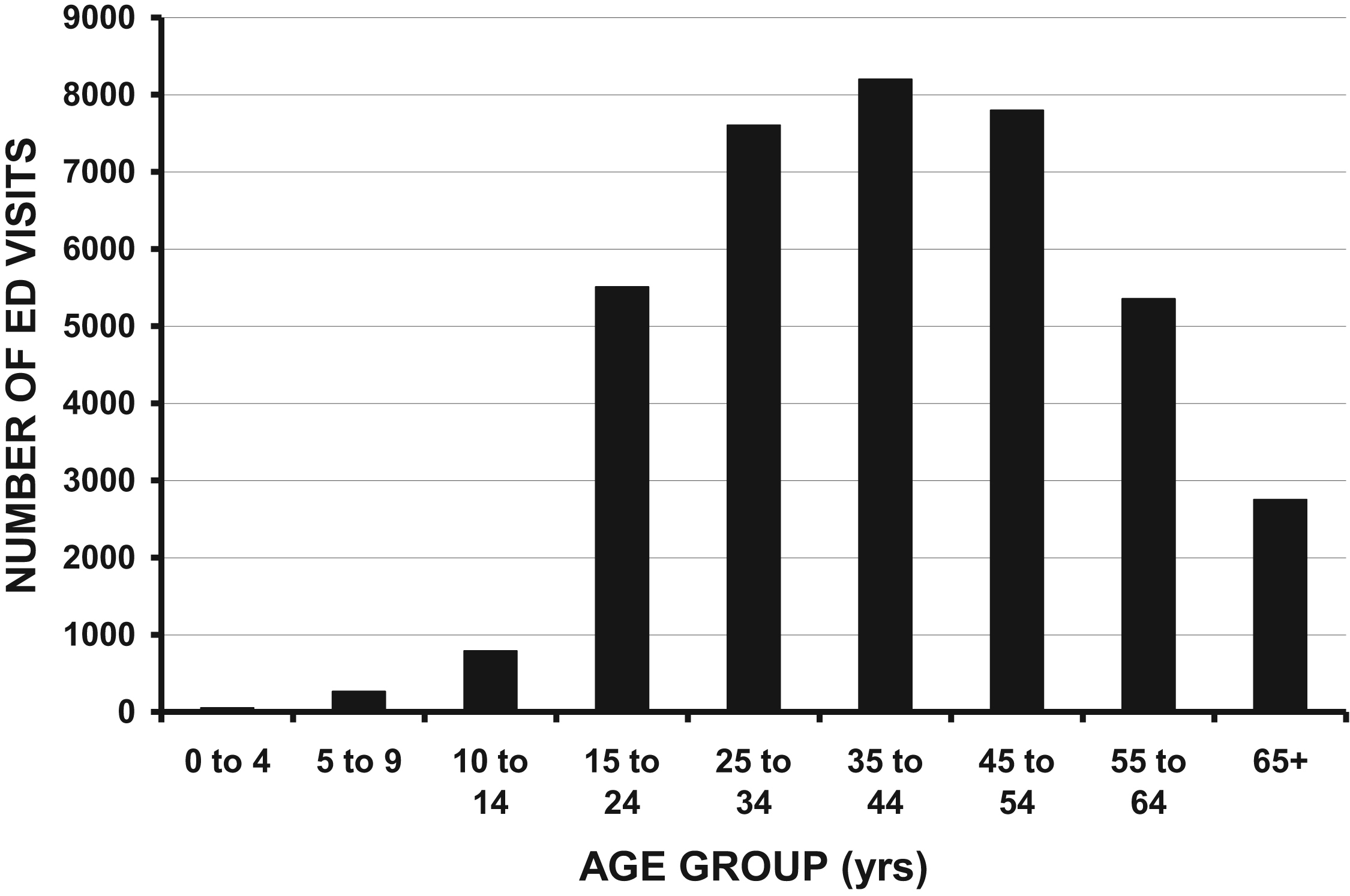
The number of emergency department (ED) visits for injuries associated with hunting stands by age.
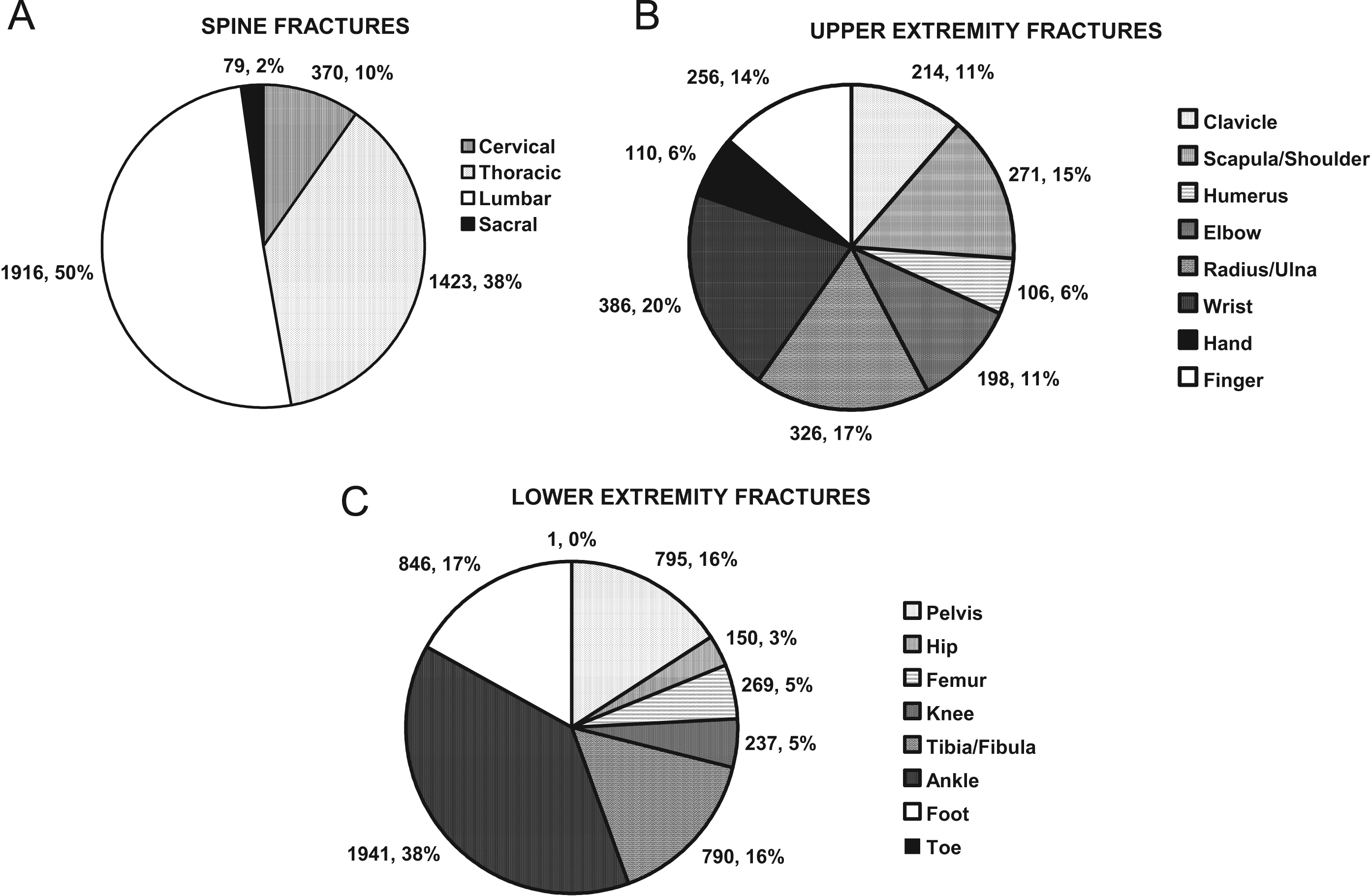
(A) Anatomic distribution of spine fractures associated with hunting stand injuries. (B) Anatomic distribution of upper-extremity fractures associated with hunting stand injuries. (C) Anatomic distribution of lower-extremity fractures associated with hunting stand injuries.
Detailed disposition from the emergency department for hunting stand injuries
% is row percentages
p value for differences between those released, transferred, admitted, or observed for each of the parameters
Discussion
There are several studies that discuss falls from tree or hunting stands (Table 3). 2 –10 There is one previous study that examines all injuries with hunting stands using the NEISS database. 10 That study, however, included only those aged 16 years or older, nor were analyses performed by groups of falling/not falling from the stand, sustaining/not sustaining a gunshot wound, association with alcohol use, or detailed analyses regarding the anatomic site for those with fractures which is of interest to orthopaedic surgeons. Some review all hunting injuries, including those associated with stands.3,9 Others review only falls from hunting stands 2 ,4,5 or only spinal injuries from hunting stand falls. 6 –8 One reviews both those released and admitted. 12 The exclusion and inclusion criteria in these studies do introduce an element of bias. However, in spite of these different inclusion and exclusion criteria, all studies demonstrate an age range (38 to 45 years) similar to the average age of 40 years in this study, and a similar proportion of males (90% to 100%) compared with 93.3% in this study.
Hunting stand injuries compiled from the literature
Many studies record fatalities (Table 3). No fatalities were noted in this series. This is likely because very seriously injured patients with potentially fatal injuries were immediately transferred to major trauma centers. Hunting, by its particular nature, occurs in rural areas with small hospitals, and those with serious injuries are likely transferred to major trauma centers. A fatality occurring at the subsequent hospital would not be captured by the NEISS database, explaining the lack of fatalities in this study. Finally, it is possible that not all the injuries are included because some might have been coded as a gunshot wound rather than associated with a hunting stand.
Spine fractures are another serious injury, with most occurring in the lumbar and thoracic spine. The proportion of cervical spine fractures in this study is similar to that of Crites et al 6 but less than that of Fayssoux et al, 8 whose patients were treated at a major spinal cord injury center. Such a study skews the data toward those with more severe injuries or paralysis and is not an accurate global description of the different levels for spine fractures from hunting stands. Another serious injury involves internal organs. In this study the most frequent organ system injured was the brain, followed by the thorax and finally the abdomen. These are similar to those observed by Gates et al, 5 but different from those of Metz et al. 4 Overall the differences between this study and the literature in the proportion of spine fractures and internal organ injuries is likely attributable to the use of a large national database, which adds more representative values.
Alcohol use and hunting stand injury has been previously noted, ranging from 2.3% to 21%, 2 ,3,6,8 although it was much less in the current study at 0.6%. This is likely owing to the fact that all injuries were included, not just those admitted or seen at major trauma referral centers with more serious injuries.
In addition to the limitations noted above, there are other limitations to this study. One is that the NEISS only identifies individuals who sought care in an ED. The overall number of injuries in this study is therefore lower than the real number of injuries. The NEISS is skewed to more serious injuries, because patients sustaining significant injuries will likely seek immediate care in the ED. Another potential limitation is the accuracy of the NEISS data. However, it has been demonstrated to have more than 90% accuracy. I thus believe the numbers in the current study to be accurate. With this in mind, these results can serve as a reference for future studies regarding injuries associated with hunting stands.
Conclusions
This study has characterized the epidemiology of hunting stand injuries. Approximately 6385 patients annually sustain injuries from hunting stands with an average age of 40 years. The patients are predominantly male, white, and seen at small- or medium-size hospitals. A fracture is the most common injury and there is a very low alcohol intoxication rate. This baseline data can now be used to educate first responders, guide medical kit development, and serve as an epidemiological basis for future studies.
Footnotes
Acknowledgments
This research was supported in part by the Garceau Professorship Endowment, Indiana University, Department of Orthopaedic Surgery, and the Rapp Pediatric Orthopaedic Research Endowment, Riley Children’s Foundation, Indianapolis, Indiana.